Embed Size (px)
Citation preview

Acromegaly
Dr Thomas foxSpR Diabetes and Endocrinology
Derriford Hospital

Learning outcomes
• Incidence and presentation• The roles of IGF-1 and GH• An approach to management 2009• Prognosis• Novel therapies

Definition
• Disproportionate skeletal tissue and soft tissue overgrowth
• Results from hyperplasia of pituitary somatotroph cells and excessive growth hormone production
• First described by Verga in 1864

Incidence and presentation• 5 cases per million• In a study of 600 cases commonest presenting
symptoms– Acral and facial changes– Hyperhydrosis– Headaches– Paraesthesia– Hypertension– Goitre– Rarely visual field defects– Frontal skull bossing

Diagnosis
• Historically variable reliability of GH assays• Acronegaly results in – Excessive GH throughout the day– Loss of bursts
• High random GH not useful• Low random GH <0.04µg/l makes diagnosis
unlikely• IGF-I vs OGTT

Loss of pulsatility of GH in acromegaly (umIU/L)

GH physiology
• Produced in anterior pituitary gland• Stimulated by – GHRH from hypothalamus– Ghrelin (gut)
• Inhibited by – somatostatin via SSTR 2 and 5 receptor subtypes
• SS regulates the timing and amplitude of GH release• GH receptors widely expressed in liver, fat and muscle

OGTT
• 75g oral glucose load is neuroendocrine stimulus that should suppress GH secretion
• GH should drop to <1.0µg/l during 2 hours following glucose load (sample at 0, 30, 60 and 120mins)
• False positives– Obesity– Renal failure– Oestrogen replacement– Diabetes mellitus

IGF-I
• Polypeptide target of GH• Synthesised– Liver (80%)– Bone– Muscle– Kidney
• Endocrine and paracrine hormone• Mediates growth actions of GH• IGF-I receptor found ubiquitously

IGF-I
• Relatively stable (unlike GH)• Positively correlated with GH• Age-matched controlled levels required (levels
fall 14% per decade)• Falsely low levels in– Renal failure– Hepatic failure– Oestrogen replacement

Mr IG• Referred in 2007 by ENT surgeons– 10 year history of snoring– Recent onset facial pain– Acromegalic features– CT scan arranged by ENT showed a 1cm pituitary adenoma
• On systems review he also had sweating but had not noticed increased size in his hands or feet.
• No headaches/visual disturbances• BP 185/65mm/Hg• On clinical examination features of acromegaly

Initial investigations
• IGF-I 85.5• OGTTT (GH 0-10mIU/L old units)– 12.4 0mins– 9.8 30– 8.5 60– 8.1 90– 10.9 120

Other endocrine parameters
• TSH 0.7• FT4 18.3• FSH 6.3• Lh 3.1• Testosterone 8.7• PRL 279• ITT cortisol peak 668

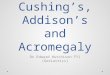
Pre-treatment MRI (pre and post-contrast)

Treatment• Acromegaly with macroadenoma– Enrolled in Medical Therapy For Acromegaly Trial
(MTAT) – Dose titrated up to 120mg monthly of lantreotide
Autogel• Disappointing response after 6 months treatment– IGF-I remained elevated at 94– OGTT
• Basal 10.7 mIU/L (reduced from 12.4) • Nadir 8.1 mIU/L
• On balance decided to continue in the trial

Interval MRI (pre and post-contrast)

At trial end
• No significant reduction in tumour size• He underwent transphenoidal
hypophysectomy• 3 month following surgery MRI
demonstrated tumour size reduction

Post TSH MRI (pre and post-contrast)


Post TSH • IGF-I 42.4• ITT (hypoglycaemia to glucose of 0.6 – seizure)– Peak cortisol 745– Basal GH 0.33 µg/L – Peak GH 19.9 µg/L– OGTT low basal level and supressed
• TSH 0.85• FT4 21.1• FSH 3.1• LH 2.5• PRL 73

Follow-up
• MR IG continued to feel unwell• Repeat MRI – no change• Repeat OGTT– Basal 0.19 µg/L– Nadir 0.1 µg/L
• Repeat IGF-I 45-48
• Discordant results • what to do next?

IGF-I and GH discordance
• Belgian registry• 229 patients• 65% concordance in GH and IGF=I results• Mostly IGF-I was not suppressed• General feeling that IGF-I gives a better idea of
cure and also determines clinical prognosis

The role of surgery
• Transphenoidal hypopyhsectomy gold standard in dedicated centre– `75-95% cure rate in intrasellar microadeomas– 40-65% cure for macroadenomas
• Complications on 1% of patients– Transient occulomotor palsies– Deterioration of vision– Carotid artery injury– Epistaxis/CSF leak– DI (transient or permanent)

Primary medical therapy?
• Only indicated in treatment of macroadenomas– ie invasion into the cavernous sinus
• May increase the cure rate with tumour shrinkage prior to surgery

Medical therapy
• 3 drug classes– Somatostatin receptor ligands– Dopamine agonists– GHRH antagonists

SRLs• Target the somatostatin 2 and 5 receptor subtypes in
pituitary and directly on the liver to inhibit IGF-I synthesis• Octreotide LAR and lanreotide Autogel no head-to-head
stduies• Indications
– Those who refuse surgery/are too unfit– Failure of surgical cure– Primary therapy if surgical cure unlikely– Whilst waiting for radiotherapy to take effect
• 75% will see a 25% tumour shrinkage• Biochemical control in 34-45% of patients• SE – abdominal bloating, gallstones/sludge• NB may interfere with GH response to OGTT

GHR antagonist• Pegvisomant
– Binds to peripheral GH receptors blocking function– GH levels increase ?due to impairment of IGF-I negative
feedback on somatotroph secretion• Daily injection 1030mg (£50-100 daily!)• Indicated
– No biochemical control despite surgical and medical therapy• Risks
– Tumour growth– Abnormal LFTs (25%)– lipohypertrophy
• ?GHR antagonist in combination with SRL

Radiotherapy
• Fractionated or gamma-knife• 50% biochemical cure at 10 years• Usually second or third line• Indicated in those– Not cured by surgery to remove need for lifelong
medical Rx– After debulking surgery– In those who have failed SRL therapy and are at
risk of tumour growth from GHR antagonist Rx

Risks of radiotherapy
• Hypopituitism in 50% • TSH 27%• LH/FSH 18%• ACTH 15%
• Visual defects 5%• Secondary tumours?• Radiation vasculopathy• Neurocognitive defects

Prognosis• Life expectancy reduced by 10%• Mortality determined by
Random GH<2.5µg/L or suppressed <1µg/L– Normalisation of IGF-1– Age– HTN– Diabetes– Cardiac disease– Duration of disease
• GH <2.5µg/L RR 1.1• GH > 2.5µg/L RR 1.9• IGF-I>95% confidence interval – SMR 3.4 fold increase• IGF-I <2SD below the mean had only 1.2 fold increase in
SMR• Effects on tumour mass

Follow-up
• IGF-I and OGTT at 3 months• Continued follow-up biochemically
• (GH is not measured in GHR antagonist therapy)• OGTT not helpful in SRL therapy
• MRI– 3-6 months post-op– May not need to be regular if biochemically “cured”6
months after commencing GHR antagonist• Pituitary function 3 months post-surgery• ITT


Summary
• Diagnosis and natural history of acromegaly• IGF-I and GH measurements and relevance as
prognostic indicators• Surgical, medical and radiotherapy options• A management and follow-up strategy for
acromegaly