Embed Size (px)
Citation preview

RESUSCITATION
EMERGENCY MEDICINE TRAINING
Presented By:
Dr. Murad Karajah
Thursday,1st of Dec,2011

Adult Cardiopulmonary Resuscitation
• Survival from in-hospital cardiac arrest has been reported to be 17%
• The survival is dependent on the actions of many people, acting as a team
The most important new recommendation chest compressions.
And change A-B-C to C-A-B

Adult Cardiopulmonary Resuscitation
patients with a witnessed VF arrest, or time is< 5 minutes, early def ibr i l lat ion is the preferred
However, in patients un witnessed VF arrest, or an arrest of unclear length of time Ini t ia l CPR has been shown to improve outcomes

The New Guidelines Recommend
It is now recommended that rescuers should make chest compressions , at a rate at least 100 compressions per minute
Another recent change to the guidelines for CPR has been the recommendation of a ratio of 30 compressions to 2 ventilations
The only exception is for rescuer CPR delivered to newborn and pt with respiratory arrest .
The chest compressions should depress the adult sternum at least 2 inches, rather than the previous recommendation of 1 ½ to 2 inches

The New Guidelines Recommend
• If an advanced airway is in place delivery of respirations should occur without pauses in compressions at a rate of 8–10 per minute

The New Guidelines Recommend
Airway Management And Ventilation• Rescue breathing and airway management are
of less importance than uninterrupted chest compressions
• Insertion of (ETT) may not be the critical airway/ventilation management intervention
• All breaths, whether delivered by (BVM) or advanced airway device should be done over 1 second and at a rate of approximately 12BPM. Hyperventilation should be avoided

Approach To Cardiac Arrest AndLife-Threatening Arrhythmias
• Cardiac arrest is characterized by an abrupt LOC because of absence of blood flow
• The most common electrical mechanisms of cardiac arrest are the ventricular tachyarrhythmia's

Adult BLS Healthcare Providers
• Patient unresponsive or gasping
First: call help or send some one to do this
Second: check pulse if present give 1 breath q 5 sec check P q 2 min
no pulse start Compression 30 then 2 breath
3d check rhythm- if shockable give one shock then CPR 2 min
not shockable start CPR 2 min then check again rhythm until patient start to move or ALS provider take over
Un Shockable rhythm – a systole – pulseless electrical activity

Adult Cardiac Arrest Shout for help/active EMS
START CPRGIVE O2
ATTACH MONITOR
ASYSTOLEPEA
VF/VT
SHOCK
CPR 2 min EPINEPHRINE every 3-5 min
Consider advanced AW
Give shock then CPR for 2 min Iv access
YES
YES
NO
NO
CPR 2 min Iv epinephrine every 3-5
minConsider advanced AW
CHECK RHYTHMTREAT
REVERSIBLE CAUSE
If rhythm shockable give 3d shock
Then start amiodarone Treat reversible cause
RHYTHMSHOCHABLE
RhythmSHOCKABLE
CPR

Post Cardiac Arrest Care
After return to spontaneous circulation optimize ventilation and oxygenation by O2 sat < 94% Don’t hyperventilate Considered intubation Treat hypotension give IV fluids bolus If no response give vasopressore infusion Do ECG 12 leads Patient not follow commands consider induced
hypothermia Signs of AMI cardiac reperfusion is indicated

CPR Quality• Push hard (>=2inches [5cm]) and fast (>=100/min) and allow complete chest recoil• Minimize interruptions in compressions• Avoid excessive ventilation• Rotate compressor every 2 minutes• If no advanced airway, 30:2 compression-ventilation ratio• Quantitative waveform capnography
-If relaxation phase (diastolic) pressure <20 mm Hg, attempt to improve CPR quality
Return of spontaneous Circulation (ROSC)• Pulse and blood pressure• Abrupt sustained increase in PETCO2 (typically>40 mm Hg)• Spontaneous arterial pressure waves with intra-arterial monitoring
Shock Energy• Biphasic: Manufacturer recommendation (120-200 J);if unknown, use maximum available. Second and subsequent
doses should be equivalent, and higher doses may be considered.
• Drug Therapy• Monophasic:360 J• Epinephrine IV/IO Dose:1 mg every 3-5 minutes• Vasopressin IV/IO Dose:40 units can replace first or second dose of epinephrine• Amiodarone IV/IO Dose: First dose:300 mg bolus. Second dose: 150 mg.
Advanced Airway• Supraglottic advanced airway or endotracheal intubation• Waveform capnography to confirm and monitor ET tube placement• 8-10 breaths per minute with continuous chest compressions
Reversible causes• Hypovolemia -Tension pneumothorax• Hypoxia -Tamponade, cardiac• Hydrogen Ion (acidosis) - Toxins• Hypo-/hyperkalemia -Thrombosis,pulmonary• Hypothermia -Thrombosis,coronary

Adult Bradycardia
symptomatic
yes
NO
No symptoms Just observation Under monitor
symptoms:Hypotension
Mental changes Shock
Chest pain Acute heart failure
HR> 50 bpmIdentify the cause
Started ABCs IV access Give O2 Monitor ECG
12 Leads
Give atropine If not effective transfer for pacing Or adrenalin Or dopamine

Adult Tachycardia With Pulse
Wide QRS < 0.12
Synchronized cardioversion
yesNO
NO
YES
IDENTIFY AND TREAT UNDERLYING CAUSE
ABCSO2 therapyIv access
BP monitoring
Symptoms :Hypotension Chest pain
Mental status changesShock
IHD Acute heart failure
Considered adenosine
Antiarrhythmic
IV accessVagal
maneuverB blocker
Ca blocker
HR<150

Synchronized CardioversionInitial recommended doses:
• Narrow regular: 50-100 J
• Narow irregular: 120-200 J biphasic or 200 J monophasic
• Wide regular: 100J
• Wide irregular: defibrillation close (NOT synchronized)
Adenosine IV DoseFirst dose: 6 mg rapid IV push: follow with NS flush.
Second dose:12 mg if required.
______________________________________
Antiarrhythmic Infusions for Stable Wide=QRS TachycardiaProcainamide IV Dose:20-50 mg/min until arrhythmia suppressed. hypotension ensues.
QRS duration increases>50%.or maximum dose 17 mg/kg given. Maintenance infusion:1-4 mg/min. Avoid if prolonged QT or CHF.
Amiodarone IV Dose:First dose: 150 mg over 10 minutes.
Repeat as needed if VT recurs.
Follow by maintenance infusion of 1 mg/min for first 6 hours.
Sotalol IV Dose:100 mg (1.5 mg/kg) over 5 minutes. Avoid if prolonged QT.
Doses/Details

Approach to patient with arrhythmia
Identify and treat underlying cause Maintain patent airway: assist breathing as
necessary Oxygen if hypoxic Cardiac monitor Monitor blood pressure Iv access 12 leads ECG don't delay therapy

Persistent tachyarrhythmia causing
• Hypotension• • Acute altered mental status• • Acute heart failure
• Ischemic heart disease
• Signs of shock

Sinus Bradycardia

First degree AV Block
• Causes
Medication
Ischemic heart disease
Hypothyroidism
• Sinus bradycardia • P wave before QRS • PR interval < 0.2 sec
P

Second Degree AV Block:
Type 1 – Wenkenbach
Causes
Inferior MI
Digoxin toxocity
• consists of progressive prolongation of the PR interval until
a nonconducted P wave occurs
P
PR

Second-Degree AV Block, Type II
• Most patients will require permanent pacemaker
• the PR interval remains constant with intermittent conduction
of atrial impulses
Conduction block below the AV node.

Third Degree AV Block:
Complete AV Block
• These patients require transvenous pacer placement for stabilization
• occurs when there is no AV conduction. P waves
• and QRS complexes exist independently of each other
• ventricular escape beats typically occur at a rate of about 40 beats/min.
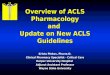
Sinus Tachycardia
Causes include• pain, fear, anxiety, • fever, hypovolemia,• pulmonary embolism,
hyperthyroidism, • CHF, ischemia,• sepsis, • alcohol, nicotine, caffeine,
catecholamine's, atropine, anticholinergic toxicity, and herbal weight
• accelerated sinus node discharge at a rate
Higher than 100 beats/min.
Normal • P wave• PR interval, and• QRS complex

SVT – Supraventricular Tachycardia
CAUSES• IHD • catecholamine's, • COPD, digoxin toxicity,
rheumatic heart disease,• (MVP), alcohol,
electrolyte abnormalities, • accessory pathways such
as (WPW).
• ectopic pacemaker or reentry
Most SVTs are AV nodal reentrant tachycardia's
• narrow QRS complexes • P waves are often
absent

Management of SVT
• Carotid massage• A denosine, • Beta blockers,• Calcium-channel blockers,• Amiodarone,• Procainamide, • Synchronized cardioversion. If the
patient’s condition is unstable

Atrial Fibrillation
Causes• hypertension,• rheumatic heart disease, • coronary artery disease
hyperthyroidism, • COPD,• CHF, and• alcohol intoxication
• multiple areas of atrial myocardium continuously
Discharging and contracting
The atrial rate is between 400 and 600
• ventricular contraction rate <100 beats/min, it is
• termed atrial fibrillation with rapid ventricular response

Management of atrial fibrillation If the duration of atrial fibrillation is less than 48 hours or no
thrombus is present on TEE - Treatment • chemical (pharmacological)• or electrical cardioversion. If the patient’s condition is unstable, immediate sedation and
synchronized cardioversion is indicated(100–200 J is usually effective).
If the duration of AF more than 48 hrs the treatment focused
to rate control • Calcium-channel blockers and beta blockers are first-line
agents • Then plan for cardioversion after 3-4 wk of anticoagulation

Atrial Flutter
Causes• CAD• AMI. • CHF,• pulmonary embolus• myocarditis,• digoxin toxicity
• a localized area of ectopy in the atrium
• regular atrial rate between 250 and 350 beats/min
• The degree of AV block
is usually 2:1 but may be greater

Management of flutter
• Treatment is directed at controlling the
ventricular rate.
Calcium-channel blockers and beta blocker are first-line
• Chemical and electrical cardioversion may also be considered. If
• the patient’s condition is unstable, immediate sedation and synchronized
• cardioversion is indicated (0.5–1 J/kg is usually effective).

Ventricular Tachycardia (Monomorphic)
• VT occurs when more than three depolarization's occur from a ventricular focus.
• VT less than 30 seconds duration is termed nonsustained ventricular tachycardia.
• QRS complex is generally wide and regular• rate higher than 100 beats/min (usually 150–200)
•Polymorphic Ventricular Tachycardia – Torsade de Pointes

Management of VT
• The most common causes of VT are ischemic heart disease . Other common causes include
• MVP, HOCM, hypoxia, electrolyte abnormalities,
• Treatment is administered according to ACLS guidelines. • Amiodarone and lidocaine are first-line agents for stable VT. • Magnesium, procainamide, and bicarbonate can also be
considered• for refractory VT. If the patient’s condition is unstable,
immediate sedation and synchronized cardioversion are indicated.

VENTRICULAR FIBRILLATION
• Treatment is administered
according to
ACLS guidelines.
• there are no organized depolarization or contractions of the ventricles.

ACUTE CORONARY SYNDROMSymptoms suggest IHD
Emergency assessment :out clinic
Monitor-IV access- bed rest
Aspirine-O2 therapy – nitroglycerin – morphine
Obtain ECG –
If ST elevation transfer urgent to hospital
If considering fibrinolysis give prehospital
Time should be recorded
ED assessment- <10 min
review rapid history ,physical exam , ECG, Monitor, cardiac enzyme,O2
Portable x ray , coagulation study
Review complete fibrinolytic checklist
Treatment in the emergency department :
O2 therapy >94% , morphine , NTG , ASA
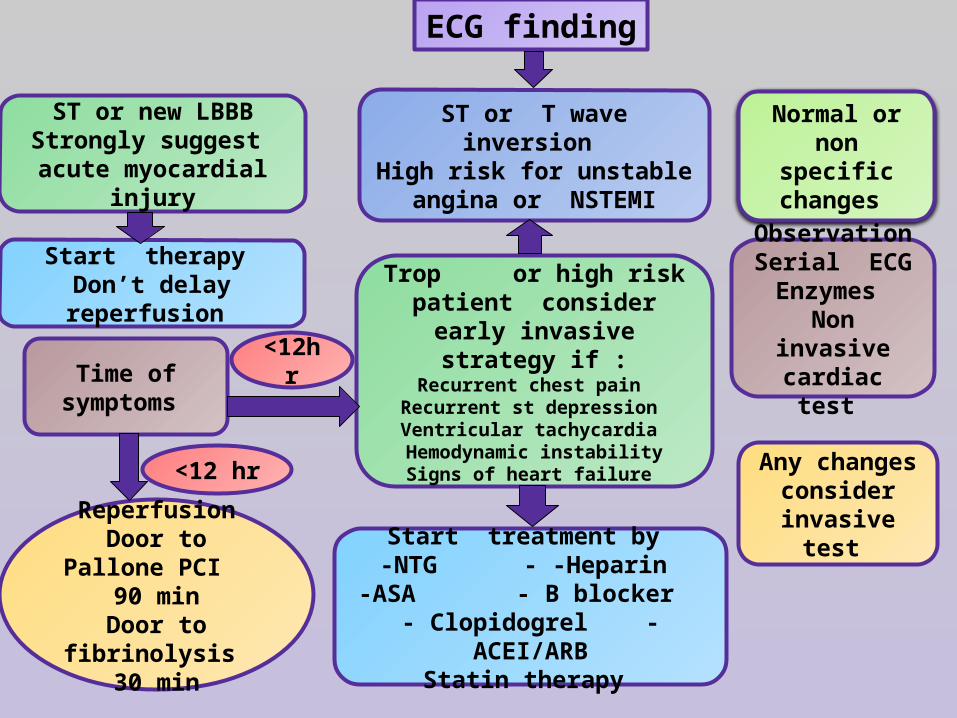
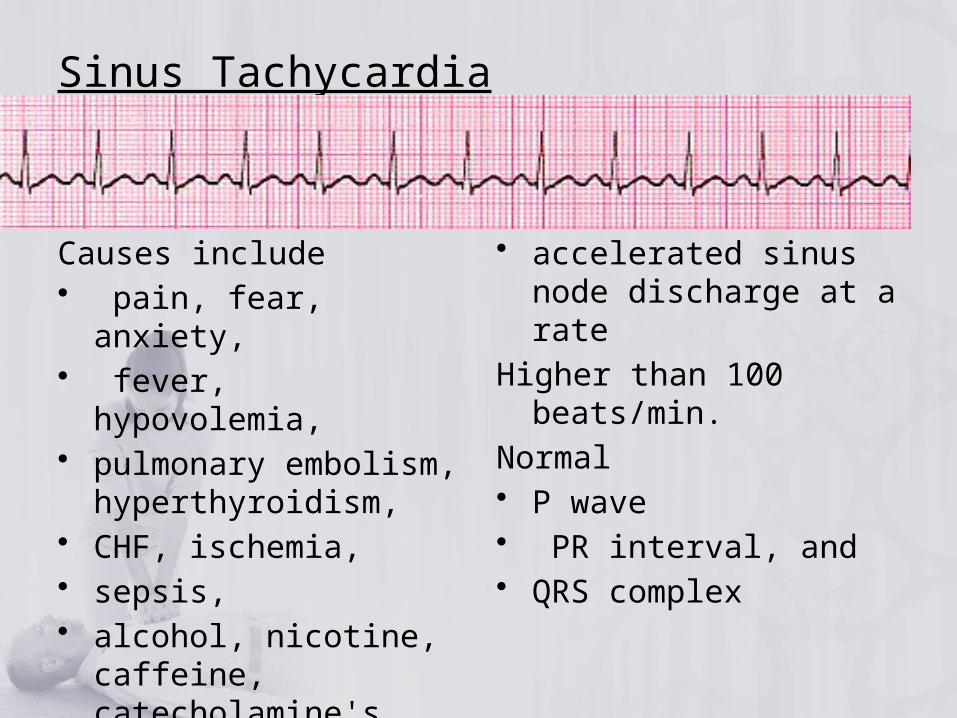
ECG finding
Normal or non specific
changes
ST or new LBBBStrongly suggest acute
myocardial injury
ST or T wave inversion High risk for unstable
angina or NSTEMI
Start therapy Don’t delay reperfusion Trop or high risk patient
consider early invasive strategy if :
Recurrent chest pain Recurrent st depression Ventricular tachycardia Hemodynamic instability
Signs of heart failure
ObservationSerial ECGEnzymes
Non invasive cardiac test Time of
symptoms
<12hr
<12 hr
ReperfusionDoor to Pallone
PCI 90 minDoor to
fibrinolysis 30 min
Start treatment by -NTG - -Heparin
-ASA - B blocker - Clopidogrel - ACEI/ARB
Statin therapy
Any changes consider
invasive test

ADULT SUSPECTED STROK
Candidate forFibrinolytic
Consult neurologist&Neurosurgery
Need admission
SIGNS&SYMPTOMS Active EMS
ASSESSMENT AND ACTIONABCs and give o2Obtain iv access
Check glucoseObtain 12 leads ECG
Order if possible urgent brain CT Alert hospital
Hemorrhagic Ischemia Yes NoCT showed bleeding
Give RtpaAnd give ASAHeparin after
24 h
Yes No
ASA

Thank You