Embed Size (px)
Citation preview
Kushal Shah BS, Matthew Stonestreet MD, Kerwyn Jones MD, Marcus Kirkpatrick MD, Caroline Frampton, Melanie Morscher PT,
John J Elias PhD
Akron General Medical CenterAkron Children’s Hospital
GrantsAkron General Medical Center Development Foundation
Akron Children’s Hospital FoundationAkron Chamber of Commerce
No Other Disclosures
ACL injuries in skeletally immature children are increasing
Non-operative management may lead to meniscal injuries & osteoarthritis
Adult ACL techniques cross the growth plate: possible leg length & angular deformities
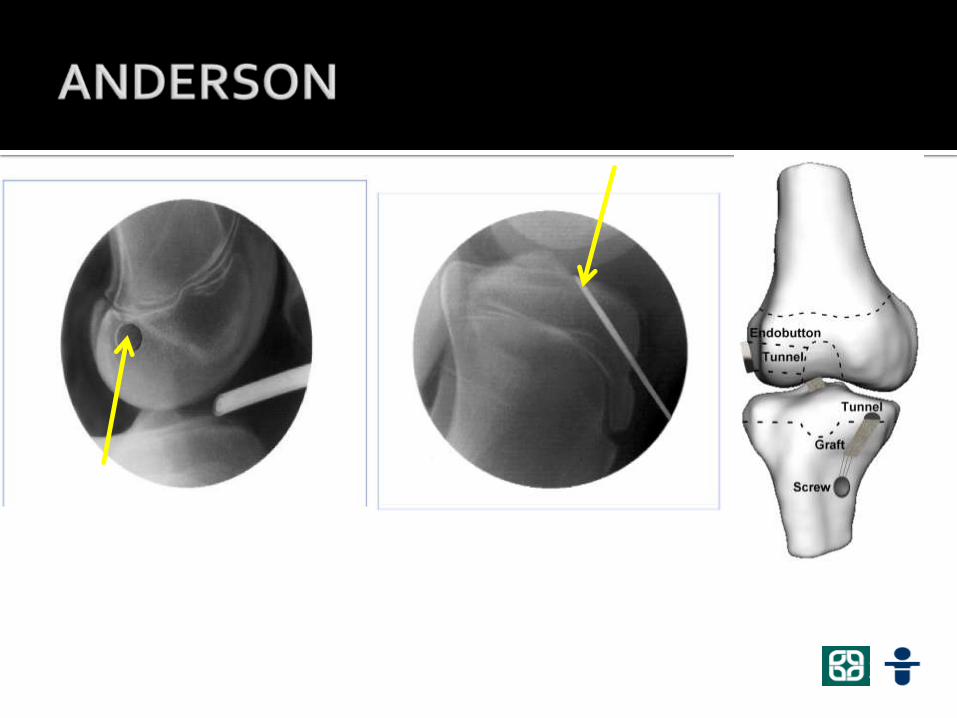
Anderson developed an All-Epiphyseal drill technique Anderson, JBJS . 2004;86- A Suppl 201-9
ACL-deficient knee increases anterior translation, shifts contact posteriorly on tibia, and increases cartilage deformation
Yoo et al. Am J Sports Med 33:240-6, 2005, Li et al., J Bone Joint Surg Am. 2006 88:1826-34, 2006
Hypothesis: All-epiphyseal ACL reconstruction will improve tibiofemoralcontact, shifting force anteriorly on the tibia and reducing contact force magnitudes as compared to the ACL-deficient knee
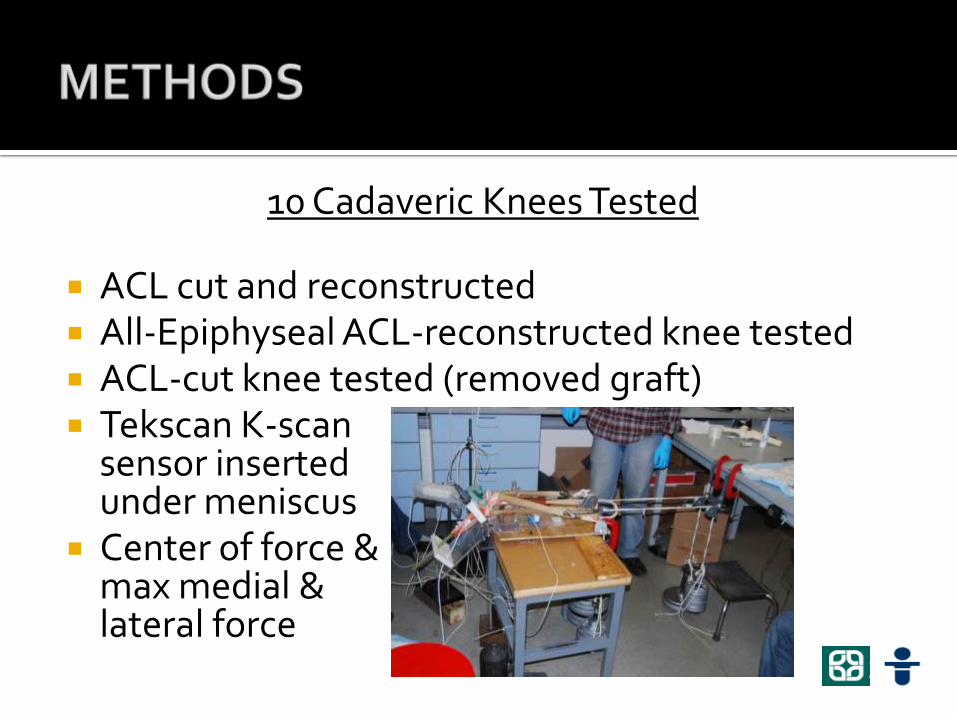
10 Cadaveric Knees Tested
ACL cut and reconstructed All-Epiphyseal ACL-reconstructed knee tested ACL-cut knee tested (removed graft) Tekscan K-scan
sensor inserted under meniscus
Center of force &max medial & lateral force
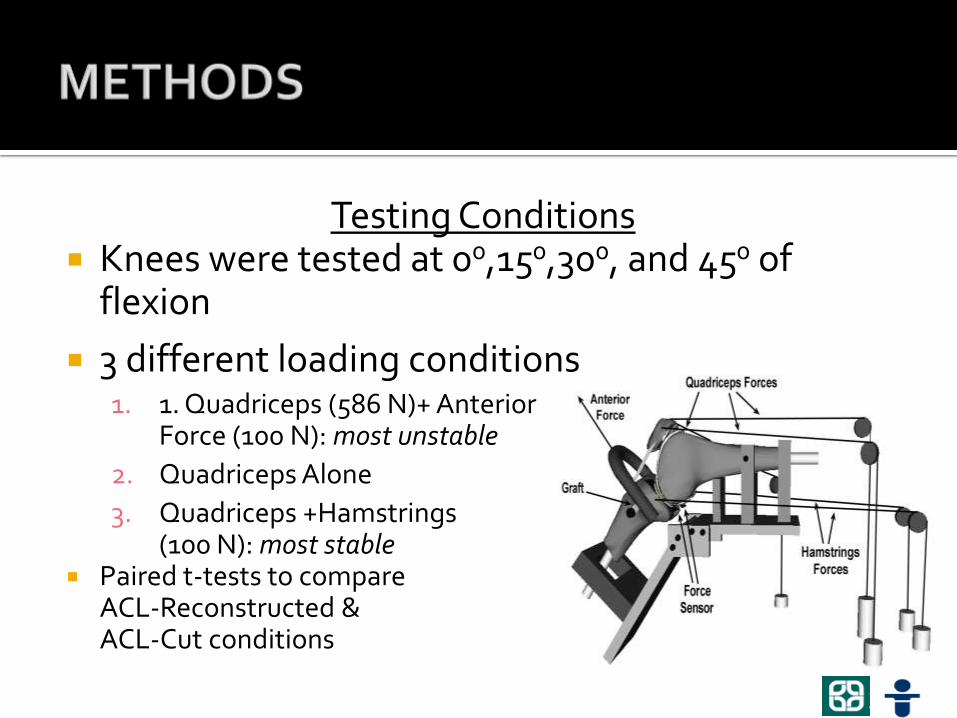
Testing Conditions Knees were tested at 00,150,300, and 450 of
flexion
3 different loading conditions1. 1. Quadriceps (586 N)+ Anterior
Force (100 N): most unstable
2. Quadriceps Alone
3. Quadriceps +Hamstrings (100 N): most stable
Paired t-tests to compare ACL-Reconstructed & ACL-Cut conditions
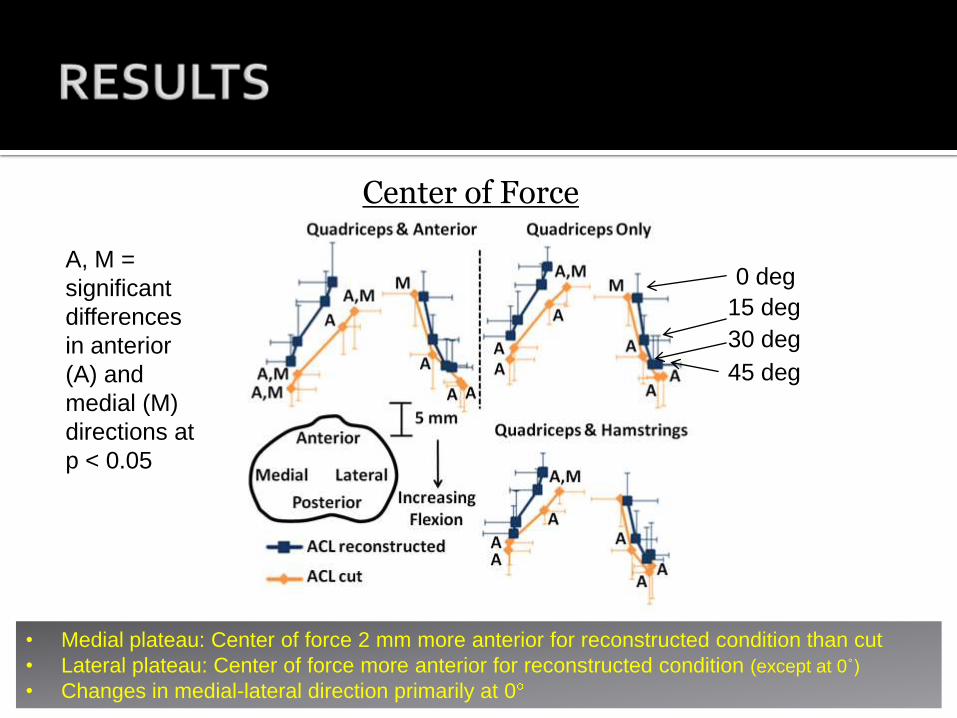
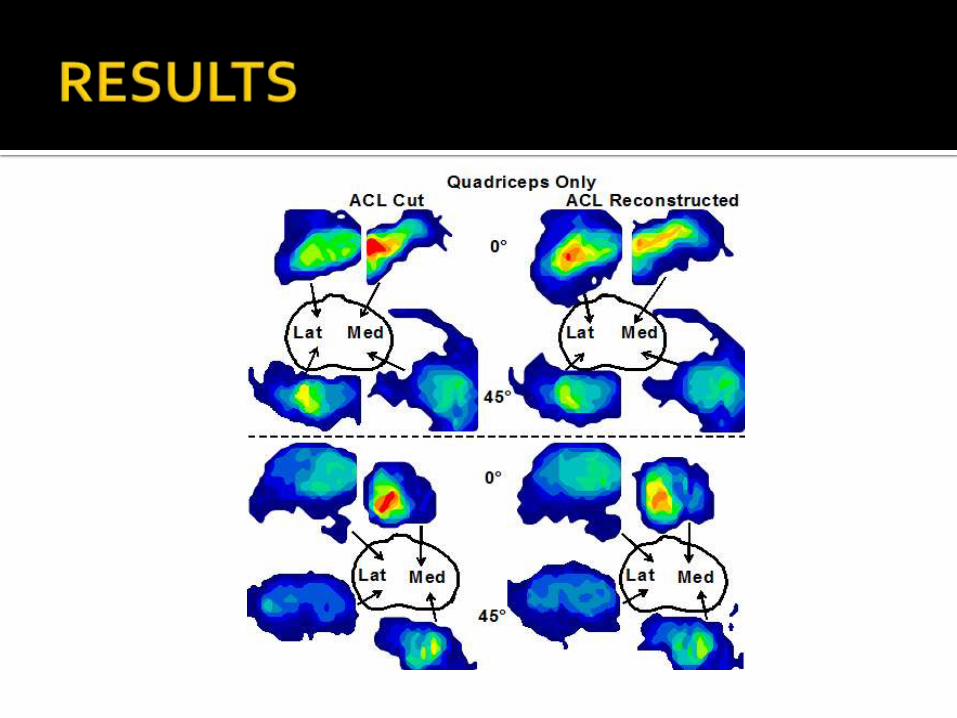
Center of Force
• Medial plateau: Center of force 2 mm more anterior for reconstructed condition than cut
• Lateral plateau: Center of force more anterior for reconstructed condition (except at 0˚)
• Changes in medial-lateral direction primarily at 0
A, M =
significant
differences
in anterior
(A) and
medial (M)
directions at
p < 0.05
0 deg
15 deg
30 deg
45 deg
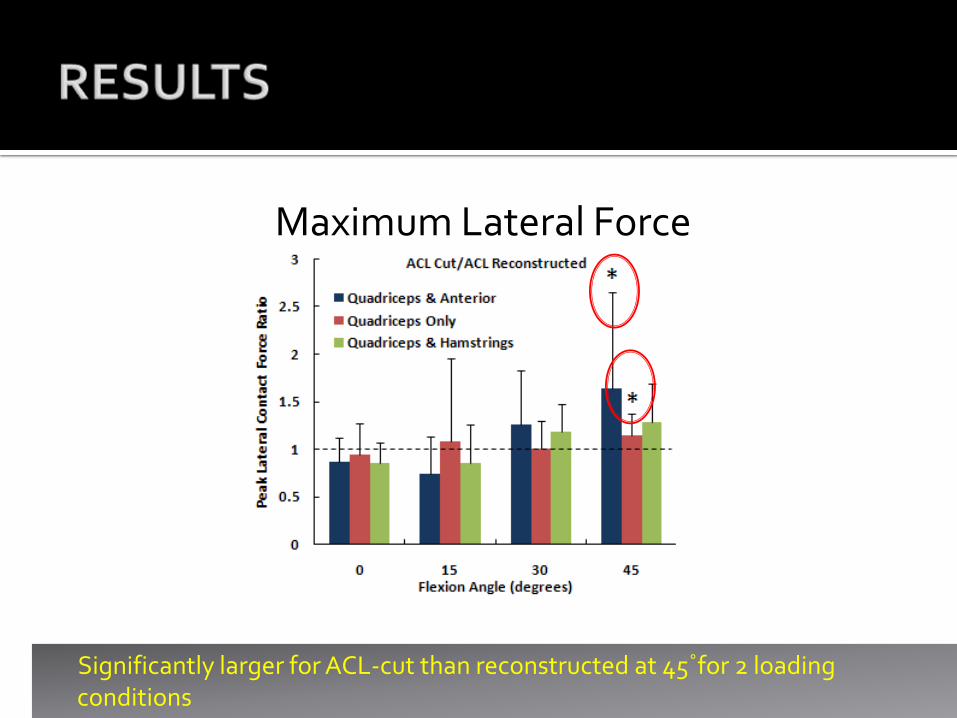
Maximum Lateral Force
Significantly larger for ACL-cut than reconstructed at 45˚for 2 loading conditions
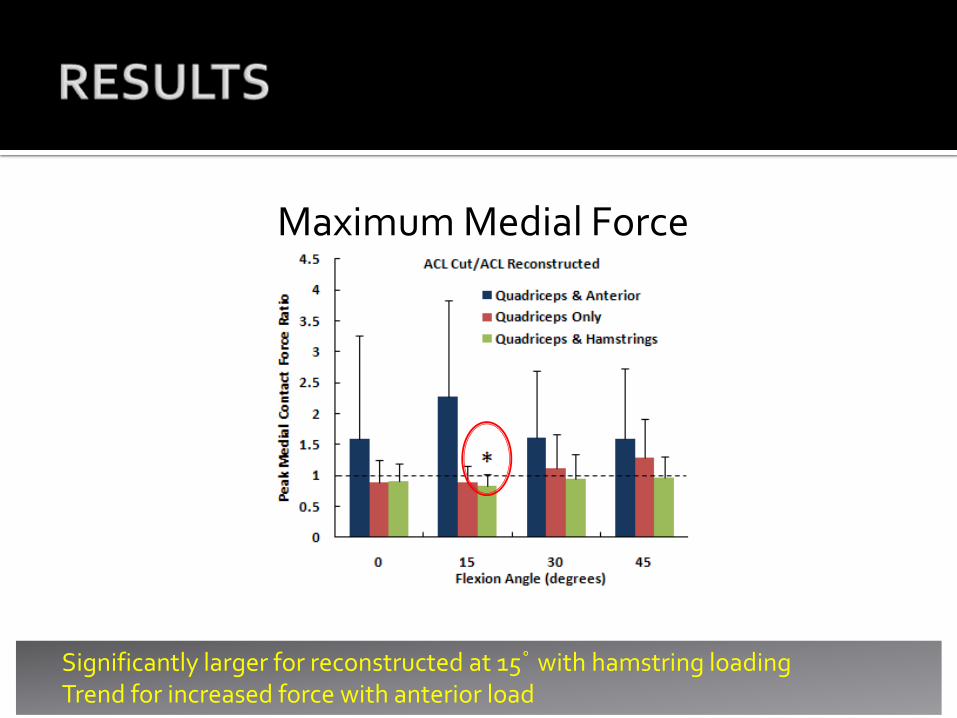
Maximum Medial Force
Significantly larger for reconstructed at 15˚ with hamstring loadingTrend for increased force with anterior load
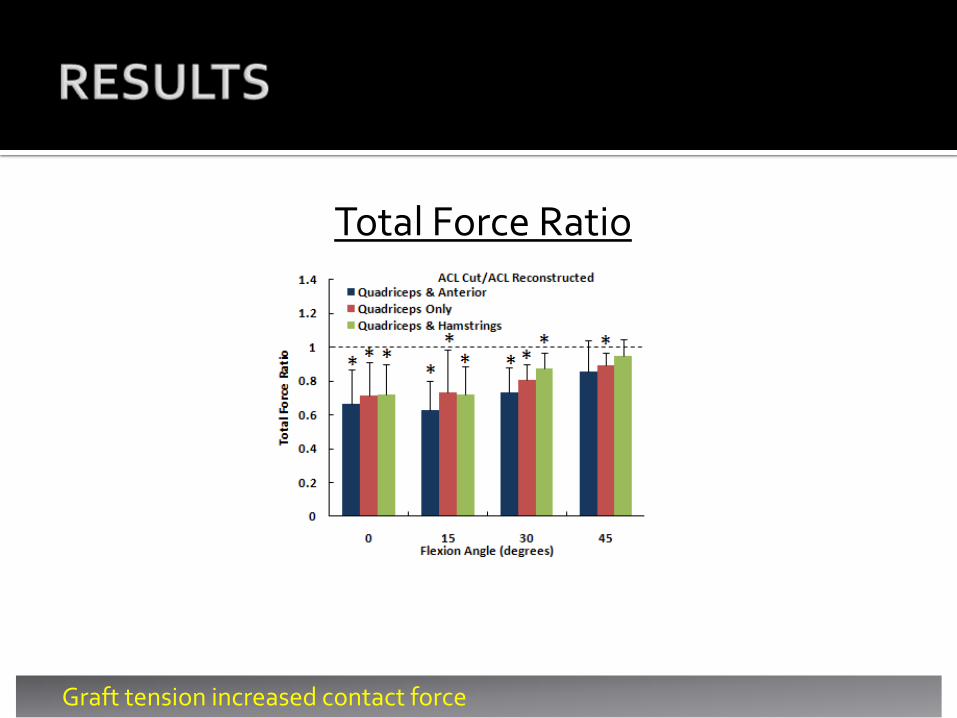
Total Force Ratio
Graft tension increased contact force
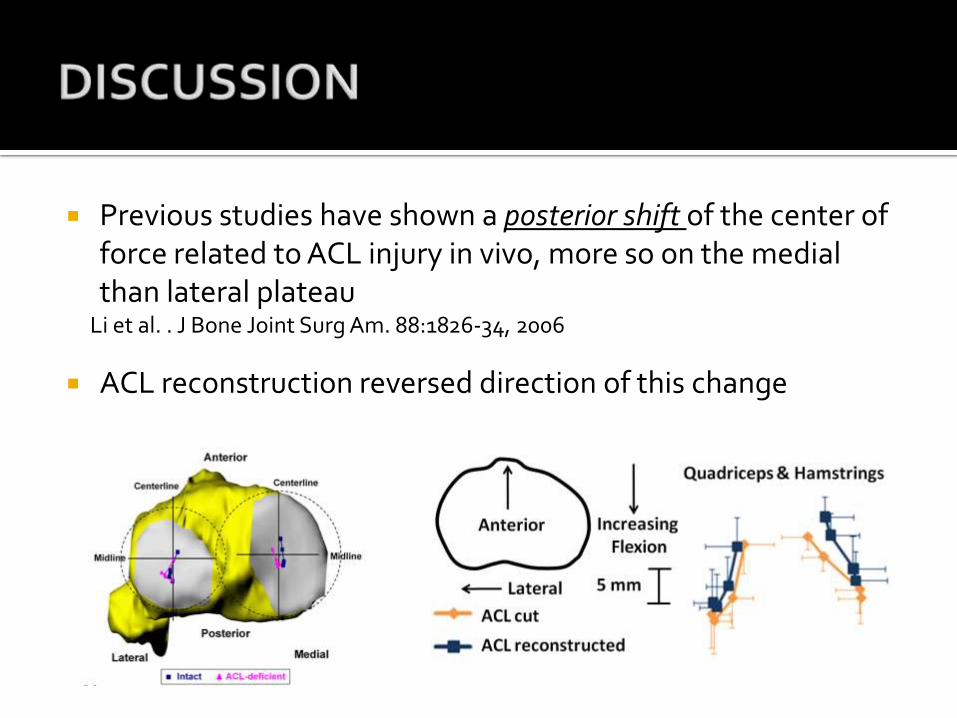
Previous studies have shown a posterior shift of the center of force related to ACL injury in vivo, more so on the medial than lateral plateau
Li et al. . J Bone Joint Surg Am. 88:1826-34, 2006
ACL reconstruction reversed direction of this change
Limitations
Cadaver study (tissue fatigue, skeletally mature specimens)
Time zero study (relaxation of the graft, bony ingrowth, loosening
of screws)
Absence of contact data for intact vs. cut knees (could
not maintain integrity and position of sensor while cutting ACL or performing reconstruction)
All-Epiphyseal ACL Reconstruction
Shifts contact anteriorly on the tibia
Decreases force for loading conditions more likely to induce instability