Embed Size (px)
Citation preview

ACID BASE ABNOMALITIES ANDMANAGEMENT
(causes and treatment)
Presenter: Dr PASHIModerator: Dr Sergii Yakubiuk
Date: 29-11-2016

OUTLINE
• Introduction• Definitions• Regulatory Mechanisms• Anion gap• Acid Base Disorders• Causes• Treatment

Introduction
• Daily acid production: 15,000 mmol of CO2 and 50-100 meq of non-volatile acid (mostly sulfuric acid from metabolism of amino acids)
• Balance maintained by renal and pulmonary excretion
• Renal excretion: combination of H+ with titratable acids, mainly phosphate and ammonia

Introduction• Balance assessed in terms of bicarbonate-carbon
dioxide buffer system, Henderson-Hasselbalch equation– pH = 6.10 x log ([HCO3] / [0.03 x pCO2])
• Acid-base homeostasis critically affects tissue and organ performance
• Both acidosis and alkalosis can have severe and life threatening consequences
• It is the nature of the responsible condition that determines the prognosis

Definitions
• An acid is a substance that can release or donate H+;
• A base is a substance that can combine with or accept H.
• Acid base balance : maintenance of normal pH within the body systems.
• Normal body pH : 7.35 - 7.45• Acidosis < 7.35 alkalosis >7.45

Definitions
• Base Excess refer to an excess or deficit, respectively, in the amount of base present in the blood. Reference range is – 2 to +2 mEq/L
• Normal pH is accomplished by regulation of hydrogen ion balance.
• When an acid (HA) is added to water, it dissociates reversibly ,
HA H+ + A- ; yielding a free H+ and its conjugate base, A-.

Definitions
• At equilibrium, the rate of dissociation of an acid , and the rate of association of H+ and A- to form HA, are equal. the acid dissociation constant, (Ka), is
• Ka = [H+]x[A-] [HA] pKa = -log10Ka (logarithmic expression of Ka)
• The higher Ka the more an acid dissociates and the stronger the acid

Definitions
• pH is a logarithmic measure of hydrogen ion concentration.
pH= -log10 [H+]
• pH is inversely proportional to [H+] . Each whole number on the pH scale represents a 10fold (logarithmic) change in acidity.

Definitions
• The pH of a solution is determined by the pKa of the acid and the ratio of the concentration of the conjugate base to acid.
pH= pKa + log [A-] [HA] (Henderson-Hasselbalch equation)

Definitions
• Most enzymes function only within narrow pH ranges
• Acid base balance can also affect electrolytes • Can also affect hormones

Regulatory Mechanisms
• Buffer system• Respiratory• Renal

Buffer system
• Take up H+ or release H+ as conditions change
• Buffer pairs – weak acid and a base• Exchange a strong acid or base for a weak
one• Results in a much smaller pH change• In the ECF, the main chemical buffers are
bicarbonate, inorganic phosphate and plasma proteins.

Bicarbonate buffer
• Sodium Bicarbonate (NaHCO3) and carbonic acid (H2CO3)
• Maintain a 20:1 ratio : HCO3- : H2CO3
HCl + NaHCO3 ↔ H2CO3 + NaClNaOH + H2CO3 ↔ NaHCO3 + H2O• It is in very high concentration and is the main
buffer pair• It is controlled both by lungs and kidneys

Phosphate Buffer
• Major intracellular buffer• H+ + HPO4
2- ↔ H2PO4-
• OH- + H2PO4- ↔ H2O + H2PO4
2-

Protein Buffers
• Includes hemoglobin, work in blood • Carboxyl group gives up H+ • Amino Group accepts H+
• Side chains that can buffer H+ are present on 27 amino acids.

Respiratory Mechanism
• Exhalation of carbon dioxide• Powerful, but only works with volatile acids• Doesn’t affect fixed acids like lactic acid• CO2 + H20 ↔ H2CO3 ↔ H+ + HCO3
-
• Body pH can be adjusted by changing rate and depth of breathing

Respiratory Mechanisms
• Arterial PCO2 stimulates chemorecptors in the medulla oblongata
• An elevated arterial blood PCO2 is a stimulus to increase ventilation leading to increased expiration of CO2 hence increase blood pH
• Conversely, a drop in blood PCO2 inhibits ventilation; the consequent rise in blood [H2CO3] reduces the alkaline shift in blood pH

Renal Mechanisms
• Can eliminate large amounts of acid• Can also excrete base• Can conserve and produce bicarb ions• Most effective regulator of pH• If kidneys fail, pH balance fails

Renal Mechanisms
• Acidification of the glomerular ultrafiltrate as the H+ is secreted into the lumen by a Na+/H+ exchanger and H+-ATPase in the brush border membrane.
• At the end of the tubule the pH would have dropped from 7.4 to 6.7
• The H+ is buffered by the HCO3- and H2PO4- (present in filtrate) and NH3 (from epith cells)

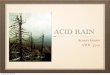
Renal Excretion of Acid, Sodium/Hydrogen Ion Exchange and Formation of Ammonia

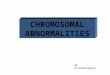
Renal Reclamation of Bicarbonate

Rates of Correction
• Buffers function almost instantaneously• Respiratory mechanisms take several minutes
to hours• Renal mechanisms may take several hours to
days

23

Acid Base Disorders
• Respiratory acidosis• Respiratory alkalosis• Metabolic acidosis• Metabolic alkalosis

Respiratory Acidosis• Acute increase in pCO2• Buffered primarily by intracellular buffersChronic state:• Kidneys compensation: - Increase net acid excretion, (48 hours for full
development)Underlying cause:• Central nervous system disease,• lung (COPD)and heart disease, • sedatives and opiates depressing the respiratory center• Hypercapnic encephalopathy can develop

Respiratory Acidosis
• Treatment - Restore ventilation - IV lactate solution - Nabicarb IV ( mmol = kg * 0.3 * BE ) - Treat underlying dysfunction or disease

27

Respiratory Alkalosis
• Carbonic acid deficit• pCO2 less than 35 mm Hg (hypocapnea)• Most common acid-base imbalance• Primary cause is hyperventilation

Respiratory Alkalosis
pCO2 , pH due to:Hypoxia (compensatory hyperventilation)• Acute: pulmonary edema or emboli, pneumonia, • Chronic: severe anemia, high altitude, hypotensionRespiratory center stimulation• Pregnancy, Anxiety, Fever, heat stroke, sepsis,
salisylate intox., cerebral disease, hepatic cirrhosis, Increased mechanical ventilation

Respiratory Alkalosis
Treatment• Treat underlying cause• Reduce ventilation, increase dead space• Breathe into a paper bag• IV Chloride containing solution – Cl- ions
replace lost bicarbonate ions

31

Metabolic Acidosis• Hallmark is [HCO3
-] • Acid production net acid intake
above net renal excretion (ketoacidosis, lactic acidosis, ammonium chloride loading)
• failure of renal net excretion (chronic renal failure, renal tubular acidosis)
• Bicarbonate loss via the gastroinestinal tract (diarrhea, gastrointestinal fistula)
• Nonbicarbonate solutions added to ECF (dilutional acidosis)

Metabolic Acidosis
Treatment - IV lactate solution - Nabicarb IV - Treat underlying cause

34

Metabolic Alkalosis
• Bicarbonate excess - concentration in blood is greater than 26 mEq/L
• Causes:– Excess vomiting = loss of stomach acid– Excessive use of alkaline drugs– Certain diuretics– Endocrine disorders– Heavy ingestion of antacids– Severe dehydration

Metabolic Alkalosis
• Alkalosis most commonly occurs with renal dysfunction, so can not count on kidneys
• Respiratory compensation difficult – hypoventilation limited by hypoxia

Metabolic Alkalosis
• Respiration slow and shallow• Hyperactive reflexes ; tetany• Often related to depletion of electrolytes• Atrial tachycardia• Dysrhythmias

Metabolic alkalosis
Treatment - Electrolytes to replace those lost - Ascorbic acid, tranexamic acid - IV chloride containing solution - Treat underlying disorder

39

Anion Gap
• The anion gap is the difference in the measured cations (positively charged ions) and the measured anions (negatively charged ions) in serum or urine.
• It is calculated as : ([Na+] + [K+]) − ([Cl−] + [HCO3−])• Anion gap is calculated when attempting to
identify the cause of metabolic acidosis.

Anion Gap
• The anion gap is influenced by changes of the unmeasured ions.
• The most frequent change is an increase of the anion gap, indicating acidosis due to accumulation of acid metabolites.
• Less frequently a decrease of the anion gap is seen, which may be due to hypoproteinemia, the presence of a cationic paraprotein as in multiple myeloma, or an increase in calcium or magnesium (“undetermined cations”).

Causes of Increased Anion Gap
• Ketoacidosis (diabetic, alcoholic, starvation) caused by acetoacetate and β-hydroxybutyrate
• Renal failure (accumulation of organic acids, sulfuric acid, phosphoric acid)
• Lactic acidosis• Treatment with substances that are unmeasured
anions at physiological pH, e.g. citrate, lactate, carbenicillin, penicillin
• Poisonings (all yield unmeasured anions) ◦Aspirin, salicylic acid, and other organic acids

Causes of Decreased Anion Gap
•Hypoalbuminemia (decrease in negative charge)•Hemodilution ◦Normal anion gap: (140 + 4) - (100 + 25) = 144 - 125 = 19 ◦But with 20% dilution: (112 + 3.2) - (80 + 20)
= 115.2 - 100 = 15.2

Causes of Acid Base Disorders
Metabolic Acidosis Anion Gap“MUDPILERS”
Metabolic Acidosis Non-Gap“HARDUPS”
Acute Resp. Acidosis“anything causing hypoventilation”
Metabolic Alkalosis“CLEVERPD”
Respiratory Alkalosis“CHAMPS”
•Methanol•Uremia•DKA/Alcoholic ketoacidosis•Paraldehyde•Isoniazid•Lactic acidosis•Ethanol•Renal failure/Rhabdo•Salicylates
•Hyperalimentation•Acetazolamide•Renal Tubular Acidosis•Diarrhea•Uretero-Pelvic shunt•Post-hypocapnia•Spironolactone
•CNS depression•Airway obstruction•Pulmonary edema•Pneumonia•Hemo/Pneumothorax•Neuromuscular
•Contraction•Licorice•Endocrine (Conn/Cushing/Bartters)•Vomiting•Excess alkali•Refeeding•Post-hypercapnia•Diuretics
•CNS disease•Hypocapnia•Anxiety•Mech. Ventilation•Progesterone•Salicylates•Sepsis

Diagnosis of acid Base Disorder
1. Determine the primary disturbance:– Acidemia or Alkalemia: look at the pH
< 7.40 = acidemia> 7.40 = alkalemia
– Respiratory or Metabolic: look at HCO3 and CO2
HCO3 = primary metabolic acidosis pCO2 = primary respiratory acidosis
and vice versa for alkalosis

Diagnosis of acid Base Disorder
2. Determine acute or chronic for Respiratory Disturbance: o Compensation attempts to normalize pH
but can be present with an abnormal pHo Expected change in pCO2 best used for
primary metabolic disturbance and expected change in HCO3 for primary respiratory disturbance

Diagnosis of acid Base Disorder
3. Primary Metabolic Disturbance:o Calculate anion gap : Na – (Cl +
HCO3)o Normal = 12 +/- 2o If gap is >20 then there is primary
metabolic acidosis regardless of pH or bicarb.
o Helps narrow differential with a anion gap or non-anion gap metabolic acidosis

Diagnosis of acid Base Disorder
4. Assess appropriate respiratory compensation for metabolic disorder:o Respiratory compensation is fasto Winters formula:
Expected pCO2 = (1.5 * HCO3) + 8 (+/-2)o If measured pCO2 is
< expected then co-existing resp. alkalosis
> expected then co-existing resp. acidosis

Diagnosis of acid Base Disorder
5. Determine if other metabolic disturbances co-exist with AG metabolic acidosis:o Delta gap – accounts for increase in anion gap
and shows any variation in HCO3o If no other disorder is present then the
calculation should be 24Corrected HCO3 = measured HCO3 + (AG - 12)oSo if corrected HCO3 >24 then metabolic alkalosis co-exists
<24 then non-anion gap metabolic acidosis co-exists

Normal values
pH 7.35 – 7.45
PCO2 35 – 45mmHg
PO2 80 -100mmHg
K+ 3.5 – 5.0meq/l
Na+ 135 -145meq/l
Cl- 98 – 108mmol/l
HCO3- 22 – 26meq/l
Anion gap 9 - 16

51

Example
55 yo man collapsed in a bar and was brought to the ER. He was unresponsive, no BP was obtainable, a sinus tachycardia was present and he had peritoneal signs.
pH 6.86 pCO2 81 HCO3 14 Na 139 Cl 84 K 3.9 HCO3 16
He was intubated, started on pressors and treated with HCO3
pH 7.04 pCO2 34 HCO3 9 Na 148 Cl 93 K 4.5 HCO3 10

On Admission• pH: 6.85 low, acidosis• pCO2: 81 high, respiratory acidosis• HCO3: 16 low, metabolic acidosis• Anion Gap: 139 – (84 + 16) = 39• Winter’s equation (expected pCO2): (16 x 1.5 = 24) + 8 =
32 (lower than observed, 81) • Delta change HCO3: (39-12 = 27 )+16 (observed) = 43 • Answer:
– anion gap metabolic acidosis – respiratory acidosis– metabolic alkalosis

After Intubation• pH: 7.04 low, acidosis• pCO2: 34 low, respiratory alkalosis• HCO3:10 low, metabolic acidosis• Anion Gap: 148 – (93 + 10) = 45 (increasing)• Winter’s equation(expected pCO2): (10 x 1.5 = 15) + 8 = 23
(lower than observed, 34) • Delta change HCO3: (45-12 + 33)+10(observed) = 43 • Answer:
– anion gap metabolic acidosis (lactate was 24) – respiratory alkalosis– metabolic alkalosis

References• Alpern RJ: Renal acidification mechanisms. In Brenner BM (ed):The
Kidney, 6th ed. Philadelphia: WB Saunders, 2000, pp 455-519.• Capasso G, Unwin R, Rizzo M, et al: Bicarbonate transport along the
loop of Henle: molecular mechanisms and regulation J Nephrol 15(Suppl 5):S88, 2002.
• Decoursey TE: Voltage-gated proton channels and other proton transfer pathways. Physiol Rev 83:475, 2003.
• Gennari FJ, Maddox DA: Renal regulation of acid-base homeostasis. • Seldin DW, Giebisch G (eds): The Kidney—Physiology and
Pathophysiology, 3rd ed. New York: Raven Press, 2000, pp 2015-2054.


























![Ursodeoxycholic acid versus placebo in the treatment of ...ursodeoxycholic acid (UDCA) [9, 10] to improve mater-nal pruritus and biochemical abnormalities. However, there are currently](https://img.pdfslide.us/doc/110x75/61033dc0eaa17e1cf4173857/ursodeoxycholic-acid-versus-placebo-in-the-treatment-of-ursodeoxycholic-acid.jpg)