Embed Size (px)
DESCRIPTION
swollen leg
Citation preview

A SWOLLEN LEGBy Maria Isabel Pino

SIMULATED CASE• All case details are put together to fit the clinical picture of the disease, and do not
represent a specific person. Pictures are open source internet content.
• 56 y/o WW
• CC: Swelling and tenderness of LLE
• History: Intermittent Swelling of Right lower extremity for the last few months, with minimal pain, erythema or warmth. Last 3 weeks swelling worsened w/ associated pain. Went to the ED 2 weeks ago, was prescribed levofloxacin and advised to elevate the leg. Swelling improved over the next days but after finishing treatment swelling and pain came back this time with associated erythema.
• ROS: absence of systemic sxs like fever, chills, night sweats throughout this course.
• PMHx: DM2 diagnosed age 38 yrs. Sometimes will have had previous trauma or surgery to the affected extremity.

Physical Exam: VTS: Afebrile and pretty normal vitals
Gen: WNL (except will usually be obese)HEENT: WNL
LUNGS: WNL
CV: WNL
GI: WNL (again, w abd obesity)
MSK: Right sided Limp, no muscle muscle weakness, good strength.SKIN: Right LE Swelling (+2) with erythema, warmth and tenderness from right foot to mild shin. Worse from ankle to toes. No clubbing or cyanosis, and no pain with passive movement of the ankle or knee joints. No raised demarcated areas
NEURO: AAOx3, CN intact, decreased sensation to light touch on dorsum and soles of feet b/l, decreased propioception, DTRs intact and symmetric.
HEM/ONC: WNL

Labs:
CBC, BMP unremarkable
Blood cultures, if obtained, negative
Imaging:
• Venous US (-) for DVT
• Right foot radiographs unremarkable

What’s the diagnosis? What should you do now?
Frequently, these patients will get another round of PO abx and sent home. If so, they fail to improve. They will say that it gets a little better if they stay off of it for 12-24 hours, but use definitely seems to make everything worse.
Now what?
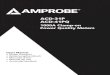
Ok, here’s your MRI

MRI with contrast
Will show lack of obvious osteomyelitis or other infection signs, but multiple small fractures secondary to…

CHARCOT FOOTDiabetic
neuropathic arthropathy
Rogers L C et al. Dia Care 2011;34:2123-2129

DEFINITION• Potentially limb threatening condition affecting bones, joints, and soft
tissues of the foot and ankle, characterized by inflammation in the
earliest phase.
• Consequence of various peripheral neuropathies, but diabetic
neuropathy has become the most common etiology.
• Interaction of several factors results in an acute localized inflammatory
condition that leads to bone destruction, subluxation, dislocation, and
deformity.
• Hallmark deformity is midfoot collapse, described as “rocker-bottom”
foot.

EPIDEMIOLOGY
• Its true prevalence and incidence are unknown but it is estimated to affect 0.8%-8% of diabetic populations.
• Up to 10% of diabetic patients with neuropathy when radiographic findings are used.
• Incidence rates ranging from 3 to 11.7/1000 patients per year have been described, but reportedly increasing.

PT CHARACTERISTICS
• Patients with COA are usually in their fifth and sixth
decades of life.
• 80% of them having had diabetes for at least 10 years.
• Bilateral COA has been reported as present in 9% of
patients with acute COA.
• However, bilateral changes of neuroarthropathy were
found by CT in 75% of patients.

PATHOGENESIS

CLINICAL MANIFESTATIONS
•Red, swollen, warm
foot in which pulses
are preserved
•Pain is not always
present or is less
than expectedBMJ 2012;344:e1397 doi: 10.1136/bmj.e1397

DIAGNOSIS• Bases on clinical presentation - the presence of an ulcer
favors the diagnosis of cellulitis or osteomyelitis, particularly if this can be probed to bone.
• Absence of skin break, stable insulin requirements, nl WBC or PCR are more suggestive of Acute Charcot.
• Plain X rays first line investigation, may initially be negative for a few days, up to three weeks.
• Bone scan or MRI. MRI more specific but equally sensitive
• MRI differentiates between Charcot from OM.



WHY IS ACUTE CHARCOT FOOT MISSED?
The acute phase may not be considered or mistaken for more common causes of leg foot swelling: cellulitis, gout, DVT or sprains.
Standard Radiographs may show no abnormalities at the stage.

KEY POINTS
(1) ACF should always be suspected in every diabetic patient with peripheral
neuropathy who presents with a red, hot, swollen foot. The virtual absence of pain
and the diffuse redness may help
differentiate this condition from cellulitis or deep venous thrombosis.
(2) Even when the diagnosis is only suspected, immediate immobilization and off-
loading and immediate refer to specialist is the wisest practice.
(3) Initially, plain X-rays may be normal but this should not deter off-loading
(4) MRI imaging should be considered when the suspicion of acute Charcot foot is
high.

Why does this matter?
Delay in diagnosis is harmful because during the acute phase the foot bones are vulnerable to fragmentation and dislocation. If the patient continues to walk on an insensitive foot, this may lead to irreversible deformities.
Deformities predispose to skin ulcer, an established risk factor for amputation.
If diagnosed in the acute phase, bone and joint damage can largely be prevented by avoiding weight bearing.
In one series, patients with acute Charcot foot or neuropathic foot ulcers had a 5-year mortality rate of 40%. Mortality may relate to co-existent renal disease in some patients, but neuropathy is also believed to independently increase cardiovascular risk by promoting vascular calcification.

KEY POINTS
• Suspect acute Charcot foot in a patient with diabetes and neuropathy who presents with a swollen warm foot
• If acute Charcot foot is suspected, arrange for offloading of the foot (to minimize further damage) and refer to a specialist foot clinicimmediately.
• Plain radiographs may be normal in the early stages of the disease
• Magnetic resonance imaging should be considered when the suspicion of acute Charcot foot is high










![LCD-Array Kit MEAT 5.0 - Specificity - CHIPRON GmbH · Donkey: ACD-005-025 Goat: ACD-006-025 Camel: ACD-007-025 Buffalo: ACD-008-025 [Equus asinus ] [Capra hircus ] [Camelus dromedarius](https://img.pdfslide.us/doc/110x75/60608c3fab6e5a6d06647729/lcd-array-kit-meat-50-specificity-chipron-gmbh-donkey-acd-005-025-goat-acd-006-025.jpg)
















