Embed Size (px)
DESCRIPTION
ikram husm
Citation preview

Powerpoint TemplatesPage 2
Causes
FIGO Classification of Abnormal Uterine Bleeding (AUB)
Investigations
Management◦ Medical
◦ Surgical
◦ Interventional

Powerpoint TemplatesPage 3
Uterine fibroids
DUB
Adenomyosis/endometriosis
Uterine hyperplasia
Uterine malignancies
Genital infections
Coagulation disorders
Idiopathic
Polyps

Powerpoint TemplatesPage 4
Term “DUB” discarded
Menorrhagia replaced with heavy menstrual bleeding

Powerpoint TemplatesPage 5
New Classification of abnormal menstrual bleeding 2009

Powerpoint TemplatesPage 7
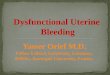
Notation. A. In all cases, the presence or absence of each criterion is noted using
“0” if absent, “1” if present, and “?” if not yet assessed. Each of the cases shown has 1
abnormality identified. From the top: at least one submucosal leiomyoma (LSM);
adenomyosis (A)—focal and/or diffuse; endometrial polyps (P); and an absence of any
abnormality, leaving endometrial causes (E) as a diagnosis of exclusion. B. Each of the cases
shown has more than 1 positive category. From the top: submucosal leiomyoma and
atypical endometrial hyperplasia (M), as diagnosed by endometrial sampling; endometrial
polyps and adenomyosis; endometrial polyps and subserosal leiomyoma (LO); and
adenomyosis, subserosal leiomyoma and coagulopathy (C), as determined by positive
screening test and subsequent biochemical confirmation of von Willebrand dis

Powerpoint TemplatesPage 10
General assessment
◦ Full blood count
Determine ovulatory status
◦ Detail structured history
◦ Progesterone assessment mid luteal
Screening for systemic hemostasis
◦ Bleeding disorders
◦ Von Willebrand factor
Evaluation endometrium
◦ Adequate endometrial sampling
Evaluation endometrial cavity
◦ Transvaginal ultrasound

Powerpoint TemplatesPage 11
Blood tests◦ FBC, thyroid, coagulation abnormalities
Pap test
Endometrial biopsy
Ultrasound scan

Powerpoint TemplatesPage 12
Exclusion of malignant causes is vital i.e. endometrial cancer or hyperplasia.
Benign organic causes of menorrhagia include endometrial polyps and sub mucous fibroids.

Powerpoint TemplatesPage 13
People with risk factors for endometrial cancer or hyperplasia. The following were found to be independently associated.
1. Obesity(>90kg);2. Infertility3. Nulliparity;4. Age >45 yrs; ( At 40 yrs 5/100,000, 45 yrs
13/100000, 55 yrs 32/100000)5. Family history of colon cancer

Powerpoint TemplatesPage 14
D&C is not performed as an initial work up. Should be performed in conjunction with hysteroscopy to evaluate endometrial cavity.
Pipelle endometrial biopsy appears at least as accurate as D&C, has high levels of patient acceptability, lower complication rates and do not require inpatient admission or GA.

Powerpoint TemplatesPage 18
No tissue found◦ Most likely endometrium is atrophic and
requires estrogen Simple proliferative
◦ This is normal and does not require treatment Endometrial hyperplasia
◦ Except atypical adenomatous requires progestins regimens
◦ Atypical adenomatous hyperplasia, hysterectomy advised
Endometrial carcinoma◦ Refer onco team

Powerpoint TemplatesPage 20
Overall health and the medical history
Cause and severity of condition
Tolerance of medications
Future childbearing plans
Effect of condition on lifestyle

Powerpoint TemplatesPage 21
Iron supplements Nonsteroidal anti-indflammatory
drugs(NSAIDs) Transnexamic acid Oral contraceptives Oral progestogen Hormonal IUS (Mirena) Danazol GNRH

Powerpoint TemplatesPage 22
MIRENA – now is first line medical therapy

Powerpoint TemplatesPage 23
Days of cycle
Ovulation
Ovulation
Menstruation

Powerpoint TemplatesPage 24
Bleeding patterns of LNG-containing intrauterine systems (Mirena®):
-3 -2 -1 1 2 3 4 5 6 7 8 9 10 11
In the first 3-6 months irregular bleeding and spotting
shorter, lighter and less painful periods
about 20% of women may have no bleeding after 1 year

Powerpoint TemplatesPage 25
Mirena effectively reduces menstrual blood loss (MBL)
0
50
100
150
200
Before
insertion
3 6 12
Months of Mirena use
Media
n M
BL (
mL)
* * *
* p<0.001
─86%─97%─91%
%
Reduction
(80mL MBL = menorrhagia)
Andersson JK, Rybo G. Levonorgestrel-releasing intrauterine device in the
treatment of menorrhagia. Br J Obstet Gynaecol. 1990; 97: 690-4

Powerpoint TemplatesPage 26
126
128
130
132
134
136
138
140
0 1 2 3 4 5 6 7 8 9 10 11 12
Months of Mirena use
Mean s
eru
m
haem
oglo
bin
(g/L
) **p<0.001###p<0.01

Powerpoint TemplatesPage 27
IUS
0
10
20
30
40
50
60
70
80
90
100
Mirena Control
Pro
po
rtio
n o
f w
om
en
(%
) *p<0.001; between groups
. Lähteenmäki P, Haukkamaa M, Puolakka J, et al. Open randomised study of use of
levonorgestrel releasing intrauterine system as an alternative to hysterectomy. BMJ
1998; 316: 1122-6

Powerpoint TemplatesPage 28
Compared to endometrial ablation◦ Slightly less mean reduction of blood loss but
equal patient satisfaction
◦ Similarly equal satisfaction to hysterectomy
◦ Higher continuation rate
◦ More cost effective
◦ Should be considered in women who failed medical therapy
◦ Added advantage of reliable contraception
◦ Risk of expulsion 10-20%
◦ Need trained staff for insertion

Powerpoint TemplatesPage 29
TCRE
Roller-ball
Laser
Thermal balloon
Heated free fluid
Cryoablation
Microwave endometrial ablation (MEA)
Radiofrequency electricity (NovaSure)

Powerpoint TemplatesPage 30
Better mean reduction of blood loss
Longer learning curve
Higher complication rate
Consider childbearing plan

Powerpoint TemplatesPage 31
Hysterectomy◦ Vaginal
◦ Abdominal
◦ Laparoscopic
Myomectomy

Powerpoint TemplatesPage 32
Hysterectomy◦ Provides definitive cure
◦ More expensive
◦ O.1 -1.1 cases of mortality per 1000 procedures
◦ Morbidity rate up to 40%

Powerpoint TemplatesPage 34
Percutaneous femoral artery puncture with selective catheterisation of each uterine artery in turn

Powerpoint TemplatesPage 35
Small vessels are accessed using a microcatheterOnce the catheter is in place, PVA particles are introduced until the blood flow stopped





![Clinicopathological analysis of abnormal uterine bleeding in … · 2020. 2. 21. · abnormal uterine bleeding [AUB].3,4 Abnormal uterine bleeding is a common clinical complaints](https://img.pdfslide.us/doc/110x75/60c479f05ea55521530b1040/clinicopathological-analysis-of-abnormal-uterine-bleeding-in-2020-2-21-abnormal.jpg)