Embed Size (px)
Citation preview
COMPARATIVE EVALUATION OF
ULTRASOUND GUIDED SUPRA INGUINAL
VERSUS INFRA INGUINAL APPROACH TO
FASCIA ILIACA COMPARTMENT BLOCK –
A RANDOMISED CLINICAL TRIAL
DR . ABHIMANYU SINGH
REG . NO: 1601021006 | AUGUST 2016 | APRIL 2018
M.D Anaesthesiology, MGMCRI
GUIDE
DR . T. SIVASHANMUGAM
PROF ESSOR & HEAD
DEPARTMENT OFANAESTHESIOLOGY AND CRITICAL CARE, MGMCRI
Co-GUIDE
DR . ANNIE SHEEBA . J
ASSI STANT PROF ESSO R
DEPARTMENT OF ANAESTHESIOLOGY AND CRITICAL CARE, MGMCRI
MAHATMA GANDHI MEDICAL COLLEGE & RESEARCH INSTITUTE
2
CANDIDATE
Candidate Name : DR.ABHIMANYU SINGH
Course of Study : MD ANAESTHESIALOGY
University Identity No : 1601021006
Mobile Phone No : +919999636613
E-mail Address : [email protected]
Month/Yr of Admission : JULY 2016
Month/Yr of Examination : APRIL 2019
GUIDES
GUIDE: DR. T. SIVASHANMUGAM
HOD and Professor
Department of Anaesthesiology and Critical Care
9442505567
CO GUIDE: DR. ANNIE SHEEBA. J
Assistant Professor
Department of Anaesthesiology and Critical Care
9655035791
3
PART II – THE PROTOCOL
1 INTRODUCTION
Fascia Iliaca Compartment Block (FICB) has been used for perioperative analgesia
in patients undergoing lower limb surgeries particularly hip arthroplasty, femur
fractures and surgeries on the thigh.1To provide better analgesia, all three nerves
supplying the thigh has to be blocked. FICB successfully blocks the femoral and the
lateral femoral cutaneous nerve and some extent involves the obturator nerve.2Fascia
Iliaca Compartment Block is an anterior approach to lumbar plexus and was first
described by dalensin in 1989.Different approaches for FICB has been explained,
conventional infra-inguinal approach by Dalens and the modified supra-inguinal
approach by Stevens.3Studies comparing the two approaches shown that supra-
inguinal FICB has better postoperative analgesia and reduced opioid consumption.In
the supra-inguinal area, the femoral and obturator nerve lie on either side of the psoas
major muscle which can cause better spread of local anaesthetic drug to block
obturator nerve. Whereas in the infra-inguinal region the obturator nerve enters the
obturator foramen to supply medial compartment of thigh and less likely to be
blocked.
Hence this study is designed to identify the incidence of 3-in-1 nerve block in both
supra and infra-inguinal approach to FICB under Ultrasound guidance.
4
AIMS AND OBJECTIVES
Aim:
To quantitatively compare the incidence of 3 nerves block in ultrasound guided
supra-inguinal versus infra-inguinal approach to fascia iliaca compartment block.
Objectives:
Primary Outcome-
a. Incidence of 3nerves block ( Femoral Nerve, Lateral Femoral
Cutaneous Nerve and Obturator Nerve )
Secondary Outcome-
a. Time of onset of block of all three nerves
b. Distance between Supra- inguinal and Infra – inguinal injection
points from inguinal ligament
5
2 REVIEW OF LITERATURE
Kumar et al4 in 2015 conducted a study to compare the analgesic efficacy of
conventional infra-inguinal versus modified proximal supra-inguinal of fascia iliac
compartment block for post op analgesia in total hip arthroplasty. 40 patient
scheduled for THA were recruited for intervention and randomized to receive
landmark guided FICB either by supra inguinal approach (group S) or infra-inguinal
approach (group I) for post-operative analgesia with 40 ml of 0.2% bupivacaine, in
addition to postoperative patient controlled analgesia (PCA) with morphine. Visual
analog scale and PCA morphine consumption was used to access the postoperative
pain at 3, 6, 12 and 24 hours. The primary outcome was cumulative PCA morphine
consumption in 24 hours. The pain intensity measured by VAS score showed
significant reduction of intensity at 6-hour post block in 'group S' than compared to
'group I' but there was no significant difference in VAS at 12 and 24 hours.
Postoperative there is significant difference in time to first PCA morphine demand in
group S v/s group I. The postoperative morphine consumption was also lessin group
S compare to group I at 6, 12 and 24 hours and the cumulative morphine
consumption in 24 hours. They concluded that supra-inguinal FCIB provides better
postoperative analgesia compared infra-inguinal approach.
Capdevila X et al5 in 1998 conducted a radiological and clinical assessment of three
in one and fascia ilica compartment block.The 3-in-1 (Group 1) and fascia iliaca
compartment (Group 2). They recruited 100 adults posted for lower limb surgery.
Pain control, sensory and motor blockades, and radiographically visualized spread of
local anaesthetic solution were studied prospectively. Both approaches provided
6
efficient pain control using 30 mL of 2% lidocainewith adrenaline and 0.5%
bupivacaine and 5 mL of contrast media (iopamidol). Complete lumbar plexus
blockade was achieved in 18 (38%) Group 1 and 17 (34%) Group 2 patients (n = 50
patients per group). Sensory block of the femoral, obturator, genitofemoral, and LFC
nerves was obtained in 90% and 88%, 52% and 38%, 38% and 34%„ and 62% and
90% of the patients in Groups 1 and 2, respectively (P < 0.05). Sensory LFC
blockade was obtained more rapidly for the patients in Group 2 (P < 0.05).
Concurrent internal and external spread of the local anesthetic solution under the
fascia iliaca and between the iliacus and psoas muscles was noted in 62 of the 92
block procedures analyzedradiographically. They concluded that the fascia iliaca
com- partment block is more effective than the 3-in-1 block in producing
simultaneous blockade of the LFC and fem- oral nerves in adults. After both
procedures, blockade was obtained primarily by the spread of local anesthetic under
the fascia iliaca and only rarely by contact with the lumbar plexus. The fascia iliaca
compartment technique provides faster and more consistent simultaneous blockade
of the lateral femoral cutaneous and femoral nerves.
Swenson et al6 conducted radiological evaluation of spread of local anaesthetic and
its effects on obturator nerve when injected deep to the fascia iliaca at the level of
the inguinal ligament. Patients were prospectively studied, and images were
interpreted using a randomized and blinded protocol. Ten patients (ASA 1-2) having
anterior cruciate ligament reconstruction received either 3-in-1 or FI compartment
blocks for postoperative analgesia using the surface landmarks techniques .
Ultrasound was used to position the injecting needle immediately deep to the FI.
Local anesthetic distribution was studied using MRI. Patients were examined for
7
motor and/or sensory function of the femoral, obturator, and lateral femoral
cutaneous nerves. Magnetic resonance imaging was used to document the limits of
injectate distribution. Magnetic resonance imaging showed distribution of injectate
over the surface of the iliacus and psoas muscles to the level of the retroperitoneum.
No patient showed medial extension of injectate to the Obturatornerve . At the level
of the inguinal ligament, injectate extended laterally toward the anterior superior iliac
spine and medially to the femoral vein. All patients had significant weakness with
extension of the knee and sensory loss over the anterior, lateral, and medial thigh. No
patient demonstrated decreased hip adductor strength. Ultrasound and MRI show
consistent superior extension of local anesthetic to the level of the retroperitoneum
for both techniques. There was reliable clinical effect on the femoral and lateral
femoral cutaneous nerves. However, none of the injections produced evidence of ON
block either at the level of the retroperitoneum or the inguinal ligament.
McNamee DA et al7 hypothesized that addition of obturator nerve block to combined
femoral and sciatic nerve block improves the quality of postoperative analgesia for
total knee replacement. They recruited 60 patients posted for Total knee replacement
randomised into two groups. Group 1 received combined femoral- sciatic nerve
block with 15 ml of 0.75% ropivacaine at each nerve. Group 2 received combined
femoral- sciatic nerve block with 15 ml of 0.75% ropivacaine at each nerve and 5 ml
in obturator nerve block. Peripheral nerve blocks were successful in 85% of patients.
The group which received the obturator nerve block showed a significant increase in
the time until their first request for analgesia (mean 257.0 vs. 433.6 min) and a
significant reduction in the total requirements for morphine throughout the study
period (mean 83.8 vs. 63.0 mg) (P<0.05). There were no systemic or neurological
8
sequelae in any of the groups. They concluded addition of an obturator nerve block
to femoral and sciatic blockade improved post-operative analgesia following total
knee replacement.
Olivier Cuignetet al8conducted a randomised, prospective, double- blind study to
assess the efficacy of continuous FICB for pain management in burns patient
undergoing skin grafting from thigh donor site..Twentypatients,withatotalburnsurface
area of 16% ± 13% (mean ± SD) were randomized 1:1 to receive either ropivacaine
0.2% or saline 0.9%. All patients received a general anaesthetic followed by pre-
incision continuous FICB by landmark guided “ double pop” technique and 40 mL of
the randomized solution, then an infusion of 10 mL/h of either ropivacaine or saline
until the first resin change(72hlater) was given.Patientswith continuous FICB had
significantly reduced postoperative morphine consumption at all time points (23± 20
versus 88 ± 29 mg after 72 h, study versus control groups, respectively; P < 0.05). In
both groups, VAS scores remained low but were only significantly lower for patients
with continuous FICB during the first dressing change. They concluded that
continuous FICB is more effient method for diminishing pain at thigh donor site.
9
3 RESEARCH QUESTION OR HYPOTHESIS
Supra – inguinal approach to FacsiaIliaca Compartment can produce higher
incidence of 3 in 1 nerve block compared to Infra- inguinal Approach.
Subjects and Methods
3.1 STUDY SUBJECTS
The Study InvolvesHUMANS
3.2 TYPE OF STUDY
Randomised Clinical Trial
3.3 PLACE OF STUDY
Mahatma Gandhi Medical College and Research Institute
3.4 SELECTION PROCESS
3.4.1 STUDY POPULATION
All patients scheduled for lower limb surgery requiring Fascia Iliaca Compartment
Block for Analgesia
3.4.2 VOLUNTEERS RECRUITEMENT PROCESS
Not Applicable
10
3.4.3 INCLUSION CRITERIA
Age 18 to 65 years
ASA I – II
All surgeries requiring FICB for analgesia
3.4.4 EXCLUSION CRITERIA
Patient refusal
Lower limb fracture
Patients allergic to local anaesthetics
Patients with coagulopathy
Patients with neurological deficits and neuromuscular diseases
Patients with infection at the site of injection
Pregnant patients
3.4.5SAMPLING PROCEDURE
60 consecutive patients posted for lower limb surgeries will randomly selected using
a closed envelope technique.
11
3.4.6 STUDY GROUPS
The Number of Groups is:TWO
Specify the Groups:
GROUP- S: This group will receive ultrasound guided supra-inguinal FICB
with 10ml of 2% Lignociane with Adrenaline and 10ml of 0.5% Bupivacaine.
GROUP –I: This group will receive ultrasound guided infra-inguinal FICB
with 10ml of 2% Lignociane with Adrenaline and 10ml of 0.5% Bupivacaine.
3.4.7SAMPLE SIZE
PS Power and Sample Size Calculation Software (Version 3.0 January 2009) was
used to calculate sample size using “Incidence of 3 in 1 block” as primary outcome
variable.
Capdivela X et al showed 34% incidence of 3 in 1 block in infra- inguinal approach
to FICB. To find double this incidence (34% vs. 70%) of 3 in 1 block in supra-
inguinal approach with error of 0.05 and power 0.80, the calculated sample size is 30
patients in each group.
12
3.5 METHODOLOGY / PROCEDURES:
After obtaining approval from the institutional ethical committee and obtaining
patient consent, 60 patients schedule for lower limb surgeries ( fulfilling inclusion
criteria ) will be recruited for this study. All patients will be premedicated with tablet
Alprazolam 0.5 mg, tablet Ranitidine 150 mg, tablet Metoclopromide 10 mg on the
night before and on the morning of surgery. After arrival in the operating theatre,
18G cannula will be secured. Standard monitoring will be used including NIBP,
SpO2, Pulse Oximeter and baseline hemodynamic parameters will be recorded.
Baseline motor assessment for femoral and obturator nerve will be done by the
examiner who will not perform the block. Femoral nerve will be assessed by
Quadriceps manual muscle testing, this will performed by making the patient sit with
knee flexed, hanging freely and back rested against the wall ( to eliminate support
from hip flexors ), examiner will apply pressure on the anterior surface of the leg and
command the patient to extent the knee against the examiner‟s resistance. Similarly,
the technique will be repeated in supine position for gravity eliminated grading (if
required). Obturator Nerve assessment will be done by muscle strength test-adductor
manual muscle testing and adductor squeeze test. Adductor manual muscle test will
be done by placing the patient on lateral decubitus position with the leg to be
assessed on the non-dependent side with 450
abduction. Resistance will be applied on
the medial surface of the leg by the examiner and patient will be instructed to adduct
the test leg towards dependent leg against resistance. Similarly, the test will be
performed in supine position to eliminate gravity (if required). Adductor squeeze test
will be done by placing the patient in supine position with knee flexed to 450 and a
commercially available stabilizer bag- pressure biofeedback ( pre-inflated to
13
40mmHg ) will be placed between the thighs and patient will be instructed to
squeeze the bag as hard as possible and the pressure exerted will be noted from the
pressure gauge attached to the stabilizer bag.
After the initial assessment, patient will be randomisedbased on the allocation
number using closed envelope technique. Patient will be prepared for the FICB
procedure and the distance from supra- inguinal and infra- inguinal injection points
from the ligament will be measured using ultrasound.
GROUP S (supra-inguinal approach):
Patient will be in positioned supine with legs slightly abducted. After strict aseptic
precaution, SonositeXporte ( Sonosite, Bothwell, WA) ultrasound system with multi-
beam (compound array) capability and with high frequency linear array transducer
( HFL 50, 15-10 MHz) will be used to perform the block. The USG probe will be
placed on the inguinal ligament and scanned upwards till the iliacus muscle, fascia
iliaca, external iliac vessels and femoral nerve are identified and distance from this
point to the inguinal ligament will be noted. 23G spinal needle will be introduced in
an in-plane approach towards femoral nerve below fascia iliaca and a total volume
20ml Local anaesthetic drug will be injected after negative aspiration of blood and
under ultrasound imaging.(2% Lignocaine with Adrenaline and 10ml of 0.5%
Bupivacaine)
GROUP I:
Patient will be in positioned supine with legs slightly abducted. After strict aseptic
precaution, SonositeXporte( Sonosite, Bothwell, WA) ultrasound system with multi-
beam (compound array) capability and with high frequency linear array transducer
(HFL50, 15-10 MHz) will be used to perform the block. The USG probe will be
placed on the inguinal ligament and scanned downwards until the femoral vessels,
14
femoral nerve are identified. The point of injection will be just above the level of
division of femoral artery close to femoral nerve depositing the drug below the fascia
iliaca. This distance will be noted. 23G spinalneedle will be introduced in an in-
plane approach towards femoral nerve below fascia iliaca and a total volume 20 ml
local anaesthetic drug will be injected after negative aspiration of blood and under
ultrasound imaging. (2% Lignocaine with Adrenaline and 10ml of 0.5%
Bupivacaine)
Patient will be continuously monitored and hemodynamic parameters recorded every
10 minutes. The motor and sensory assessment after the block, will be done by the
examiner blinded to the approach used for FICB. Sensory assessment will be done at
30, 45 and 60 minutes after block. Sensation to cold will be noted in area of sensory
distribution of the three nerves- Femoral Nerve assessed on the anterior surface of
the thigh, Lateral Femoral Cutaneous Nerve on the lateral surface of the upper thigh
and Obturator Nerve on the the medial surface of the thigh and the postero-medial
surface of the knee. Motor assessment for quadriceps muscle and adductor muscle
strength will also be repeated at 30, 45 and 60 minutes. The scores will be recorded
on the data collection sheet. After 60 minutes of assessment and monitoring, patient
will be given surgical anaesthesia for the planned procedure by the in-charge OT
anaesthesiologist. A successful 3 nerve block is considered when the sensory
assessement score for cold sensation is 0 and motor power score for quadriceps and
adductor muscles is 1-0 and 50% decrease in pressure generated by adductor squeeze
test at the end of 60 minutes after block.
15
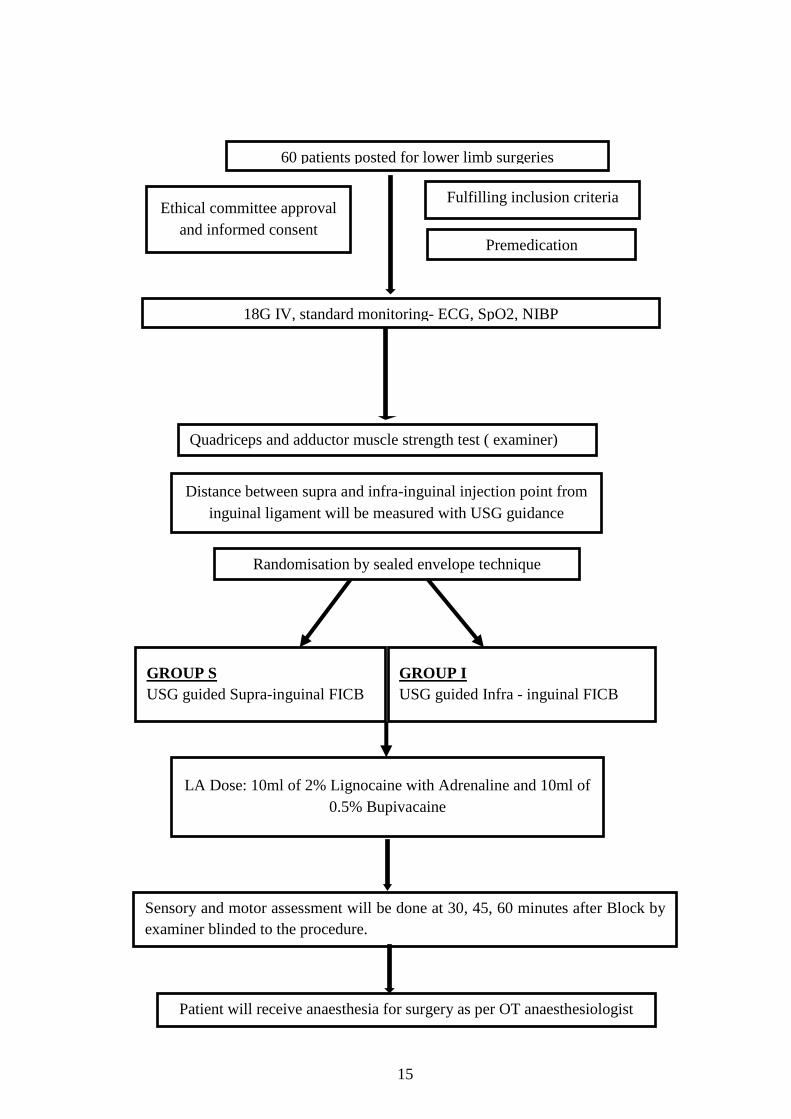
60 patients posted for lower limb surgeries
Ethical committee approval
and informed consent
Fulfilling inclusion criteria
Premedication
18G IV, standard monitoring- ECG, SpO2, NIBP
Randomisation by sealed envelope technique
GROUP S
USG guided Supra-inguinal FICB
Distance between supra and infra-inguinal injection point from
inguinal ligament will be measured with USG guidance
LA Dose: 10ml of 2% Lignocaine with Adrenaline and 10ml of
0.5% Bupivacaine
Sensory and motor assessment will be done at 30, 45, 60 minutes after Block by
examiner blinded to the procedure.
Patient will receive anaesthesia for surgery as per OT anaesthesiologist
Quadriceps and adductor muscle strength test ( examiner)
GROUP I
USG guided Infra - inguinal FICB
16
3.5.1 INTERVENTIONS/DRUGS USED
DRUGS:
10ml of 2% Lignocaine with Adrenaline and 10ml of 0.5% Bupivacaine.
PROCEDURE:
Ultrasound guided fascia iliaca block will be performed either in a supra- inguinal
region or infra- inguinal region based on the randomisation. Once the site of injection
is identified by USG guidance, 20ml of Local Anaesthetic drugwillbedepositedbelow
the fascia Iliaca. (2% lignocaine with adrenaline and 0.5% Bupivacaine)
3.5.2 PROCUREMENT OF INVESTIGATIONAL DRUGS,
STORAGE, DISPENSING, ETC.
Available from Pharmacy
3.6 STUDY TERMINATION
The study will be terminated after adequate number of cases are achieved.
4 STUDY VARIABLES
1. Dependent Variable :
Incidence of 3 nerves block
Time of onset of 3 nerves block
Extent of sensory Blockade
Quadriceps and Adductor Muscle Strength
Distance of injection site from inguinal ligament
17
2. Independent Variables:
Age
Sex
BMI
4.1 DATA COLLECTION
Data will be entered into a Data collection Proforma Sheet (Appendix 1) and entered
into Excel (MS Excel 2013). Secondary Data will be collected from patient records.
Privacy and Confidentiality will be maintained throughout. All patient identifiable
numbers and information will be stripped and replaced by anonymous numbers.
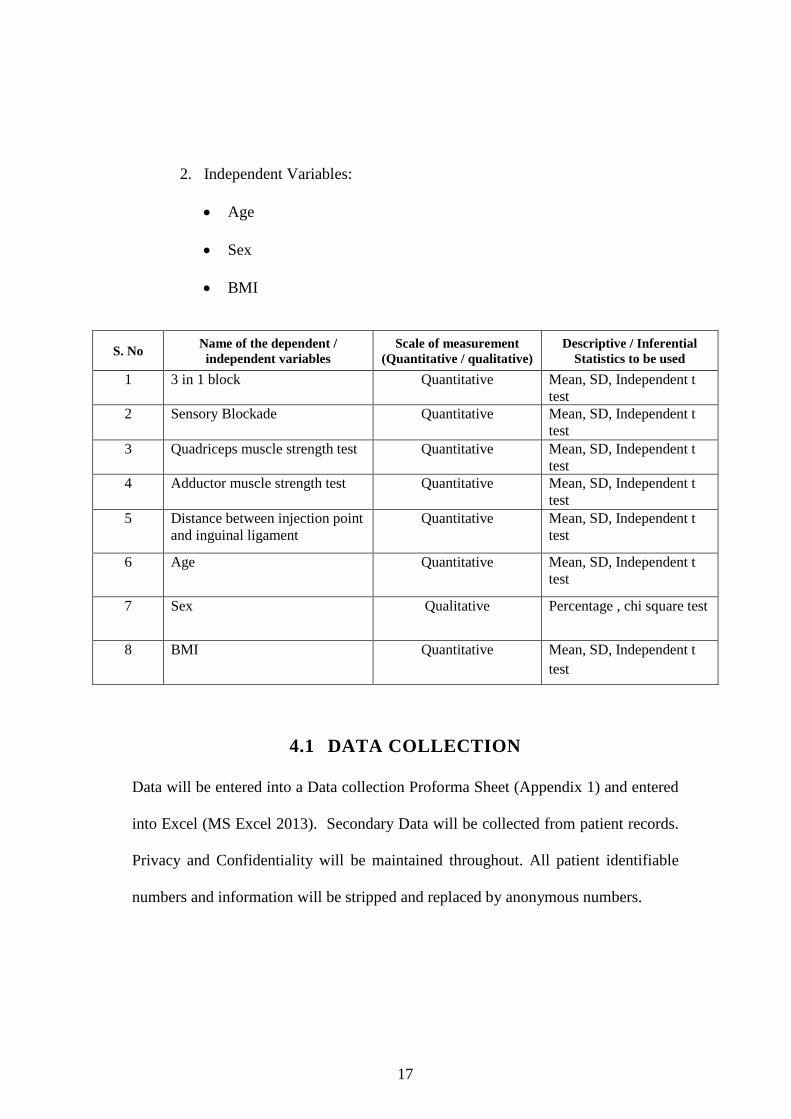
S. No Name of the dependent /
independent variables
Scale of measurement
(Quantitative / qualitative)
Descriptive / Inferential
Statistics to be used
1 3 in 1 block Quantitative Mean, SD, Independent t
test
2 Sensory Blockade Quantitative Mean, SD, Independent t
test
3 Quadriceps muscle strength test Quantitative Mean, SD, Independent t
test
4 Adductor muscle strength test Quantitative Mean, SD, Independent t
test
5 Distance between injection point
and inguinal ligament
Quantitative Mean, SD, Independent t
test
6 Age Quantitative Mean, SD, Independent t
test
7 Sex Qualitative Percentage , chi square test
8 BMI Quantitative Mean, SD, Independent t
test
18
4.2 STATISTICAL METHODS
Parametric data will be analysed using student t test.
Non-parametric data will be analysed by chi square test.
5 REFERENCES
1) DalensB, Vanneuville G, Tanguy A. Comparison of the fascia iliaca
compartment block with the 3-in-1 block in children. AnesthAnalg 1998;
69,705-713
2) Diwan S. Fascia Iliaca Block- An anatomical and Technical Description.
Journal of Anaesthesia And Critical Care Case Reports.2015; 1(1):27-30.
3) Stevens M, Hrrison G, McGrail M. A modified fascia iliaca compartment
block has significant morphine sparing effects. Anaesth. Int. Care 2007;35:
949-952
4) Kumar K, Pandey RK, Bhalla AP, Kashyap L, Garg R, Darlong V.
Comparison of conventional infra-inguinal versus modified proximal supra-
inguinal approach of Fascia Iliaca Compartment Block in Total Knee
Replacement. ActaAnaesthesiolBelg 2015; 66(3):95-100.
5) X. Capdevila, Biboulet, M. Bouregba, Y. Barthelet, J. RubenovitchF.
d‟Athis.Comparison of the Three-in-One and Fascia lliaca Compartment
Blocks in Adults: Clinical and Radiographic Analysis. AnesthAnalg
1998;86:103944)
6) Swenson JD, Davis JJ, Stream JO, Crim JR, Burks
RT, GreisPE.Localanesthetic injection deep to the fascia iliaca at the level of
19
the inguinal ligament: the pattern of distribution and effects on the obturator
nerve. Ream Act Anaesth 2005; 11: 86-91.
7) Mcnamee DA, Parks L, Milligan KR. Post-operative analgesia following total
knee replacement: an evaluation of the addition of an obturator nerve block to
combined femoral and sciatic nerve block.ActaAnaesthesiol. Scand 2002; 46
(1) :95-9
8) Olivier Cuignet,, Jean Pirson,, Jenna Boughrouph,, and Diane Duville. The
Efficacy of Continuous Fascia Iliaca Compartment Block for Pain
Management in Burn Patients Undergoing Skin Grafting
ProceduresAnesthAnalg2004;98: 1077–81.
6 PRELIMINARY WORK DONE ALREADY
Review of literature, data collection form and consent form.
7 ETHICAL ISSUES
This study aims to identify which of the two techniques causes increases chances of
3 in 1 nerve block in lower limb. The drug to be used is already approved and found
safe for nerve block.
Study involves Humans
20
8 INFORMED CONSENT PROCEDURE
Patient information and informed consent form isattached as APPENDIX 2
9 QUALITY CONTROL
Name: Dr.HemanthKumar.V
Designation: Professor
Department of Anaesthesiology and Critical Care
Telephone No: 9003550553
E-mail:[email protected]
10 SPONSORSHIPS
a. Sponsors for the study: NONE
b. Outside funding: NONE
21
11 INVESTIGATORS DECLARATION
This is to certify that the protocol entitled “Comparative Evaluation Of
Ultrasound Guided Supra- inguinal v/s Infra-inguinal Approach to Fascia Iliaca
Compartment Block – A Randomised Clinical Trial” was reviewed by us for
submission to the SBV Institutional Ethics Committee and certified that this protocol
represents an accurate and complete description of the proposed research. Wehave
read the ICMR guidelines, ICP-GCP guidelines/CPCSEA guidelines/and other
applicable guidelinesand undertake to ensure that the rights and welfare of the study
subjects are protected.
The study will be performed as per the approved protocol only. If any deviation is
warranted, the same will be presented to the ethical committee and permission will
be sought. We assure that the study will be terminated immediately in case of any
unforeseen adverse consequences and we will inform the same to the ethical
committee immediately.
Dr. T. Sivashanmugam (For HOD)
Professor and Head of
Department of Anaesthesiology 18/11/2016
Dr. Annie Sheeba.J
Assistant Professor of Anaesthesiology
18/11/2016
Dr. Abhimanyusingh
Department of Anaesthesiology
18/11/2016
Dr. Head of Department (For HOD)
Head ofDepartment of Speciality
with Dept. Seal 18/11/2016
22
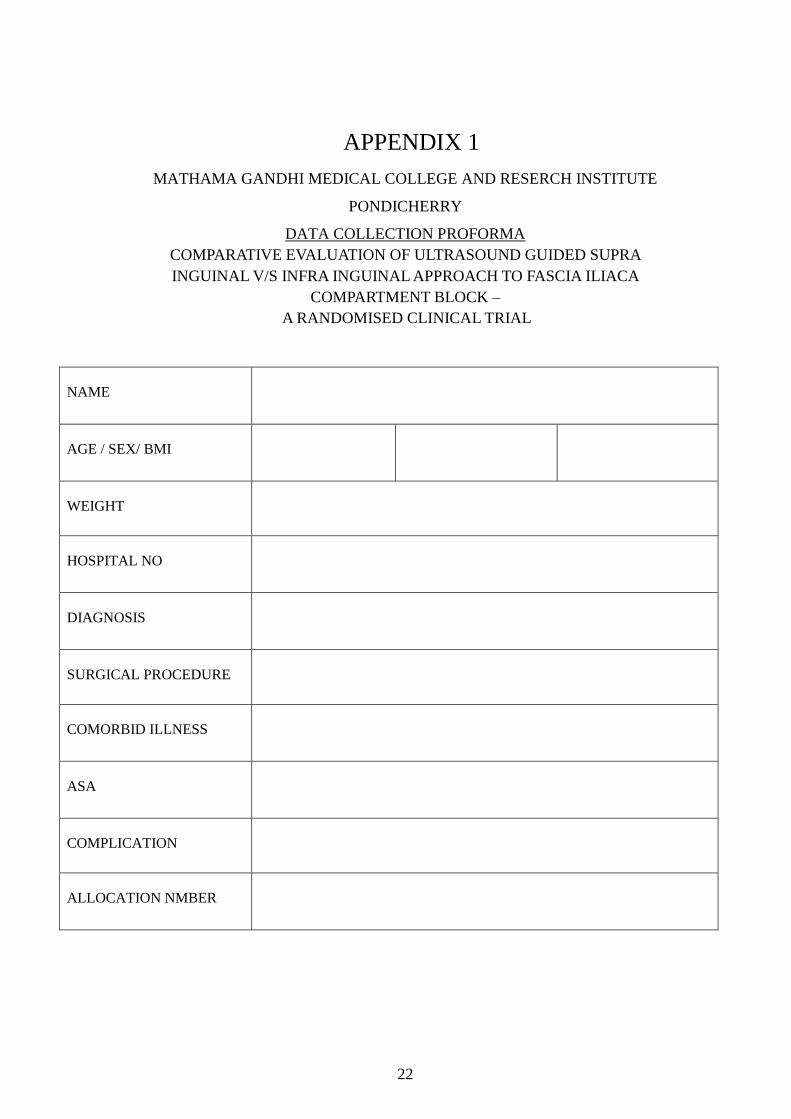
APPENDIX 1
MATHAMA GANDHI MEDICAL COLLEGE AND RESERCH INSTITUTE
PONDICHERRY
DATA COLLECTION PROFORMA
COMPARATIVE EVALUATION OF ULTRASOUND GUIDED SUPRA
INGUINAL V/S INFRA INGUINAL APPROACH TO FASCIA ILIACA
COMPARTMENT BLOCK –
A RANDOMISED CLINICAL TRIAL
NAME
AGE / SEX/ BMI
WEIGHT
HOSPITAL NO
DIAGNOSIS
SURGICAL PROCEDURE
COMORBID ILLNESS
ASA
COMPLICATION
ALLOCATION NMBER
23
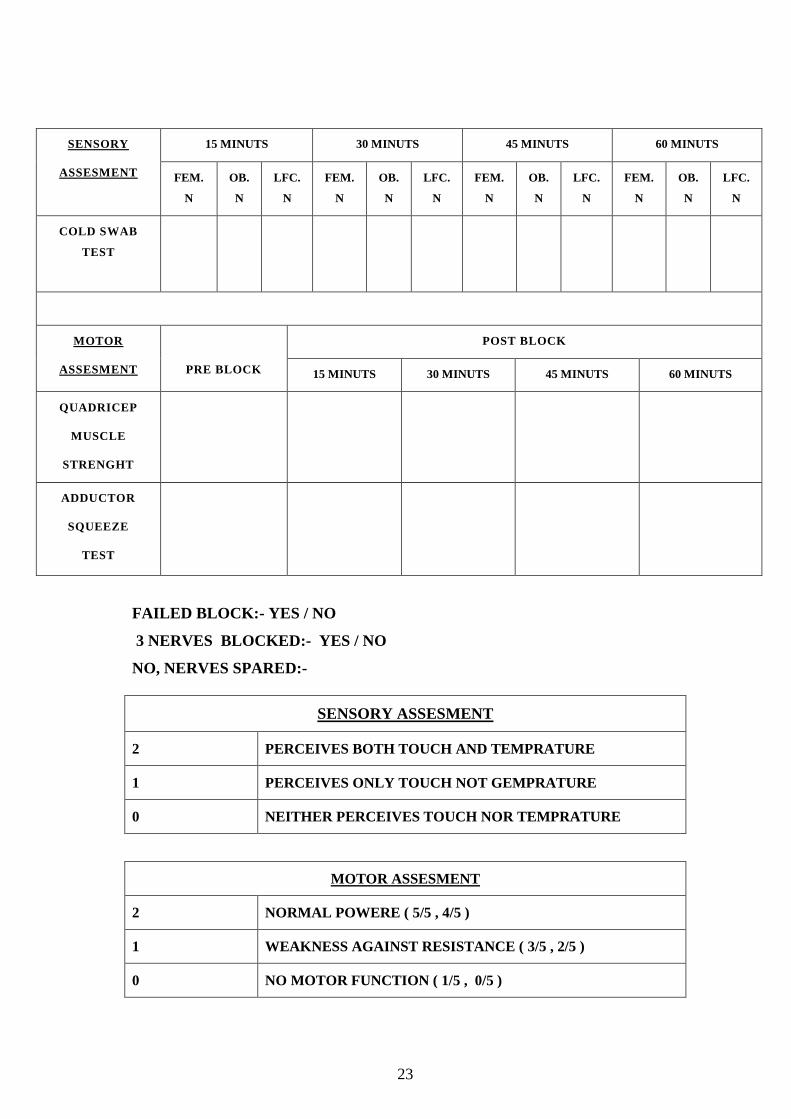
SENSORY
ASSESMENT
15 MINUTS 30 MINUTS 45 MINUTS 60 MINUTS
FEM.
N
OB.
N
LFC.
N
FEM.
N
OB.
N
LFC.
N
FEM.
N
OB.
N
LFC.
N
FEM.
N
OB.
N
LFC.
N
COLD SWAB
TEST
MOTOR
ASSESMENT
PRE BLOCK
POST BLOCK
15 MINUTS 30 MINUTS 45 MINUTS 60 MINUTS
QUADRICEP
MUSCLE
STRENGHT
ADDUCTOR
SQUEEZE
TEST
FAILED BLOCK:- YES / NO
3 NERVES BLOCKED:- YES / NO
NO, NERVES SPARED:-
SENSORY ASSESMENT
2 PERCEIVES BOTH TOUCH AND TEMPRATURE
1 PERCEIVES ONLY TOUCH NOT GEMPRATURE
0 NEITHER PERCEIVES TOUCH NOR TEMPRATURE
MOTOR ASSESMENT
2 NORMAL POWERE ( 5/5 , 4/5 )
1 WEAKNESS AGAINST RESISTANCE ( 3/5 , 2/5 )
0 NO MOTOR FUNCTION ( 1/5 , 0/5 )
24
25
APPENDIX 2
INFORMATION SHEET FOR THOSE WHO PLAN TO PARTICIPATE IN
THE RESEARCH PROJECT
NAME OF THE RESEARCH PROJECT:
“COMPARATIVE EVALUATION OF ULTRASOUND GUIDED SUPRA
INGUINAL V/S INFRA INGUINAL APPROACH TO FASCIA ILIACA
COMPARTMENT BLOCK - A RANDOMISED CLINICAL TRIAL”
We welcome you and thank you for having accepted our request to consider whether
you can participate in our study. This sheet contains the details of the study; the
possible risks, discomfort and benefits for the participants are also given. You can
read and understand by yourself; if you wish, we are ready to read and explain the
same to you.If you do not understand anything or if you want any more details we
are ready to provide the details. The purpose of my study is to find out the nerves
getting blocked while giving local anaesthetics drug at the level groin region (region
between the abdomen and the thigh). An injection with local anaesthetic drug at the
level of the groin will block the sensation through the nerves arising from there.
There are three nerves giving sensation to the skin over the thigh and the thigh
muscle. By blocking these nerves with drugs, pain relief after surgery will be better.
We intend to identify whether all three nerves get blocked while giving the drug
above or below the groin region. This study is being conducted by me, Dr.
Abhimanyu Singh a Post Graduate medical student belonging to the department of
Anaesthesialogy and Critical Care, under the guidance of Dr. T Shivashanmugam.
Professor and Head of Department of Anaesthesialogy and Critical Care, MGMC &
RI, Pondicherry. You am being considered as one of the participant Because you have
26
been referred to PAC (Department of Anaesthesialogy and Critical Care) for lower limb
surgery and you are fulfilling the criteria of this study. The choice is yours. If you do not
wish to participate you will not be included in this study. Even then, you will continue to get
the proposed medical treatment without any prejudice. After understanding the details of
the study, you should give us your written consent. You have to permit us to utilize your
clinical data and co-operation during procedure. Yes, the study will provide you longer
painless postoperative period and in the management of pain for the public in future .
There are no forcible risk or discomfort involving in the study because the drug has
been approved for use in the nerve blocks and has been proven to be safe.. you will
not be paid for the study. Your confidentiality will be maintained. if you want you can
get the details from us. You can withdraw at any time during the study period.
27
MAHATMA GANDHI MEDICAL COLLEGE AND RESEARCH INSTITUTE PUDUCHERRY
FORM FOR GETTING INFORMED CONSENT FOR THOSE PARTICIPATING IN THE RESEARCH PROJECT
Name of the Research Project:- COMPARATIVE EVALUATION OF ULTRASOUND GUIDED SUPRA
INGUINAL V/S INFRA INGUINAL APPROACH TO FASCIA ILIACA
COMPARTMENT BLOCK – A RANDOMISED CLINICAL TRIAL I _______________________ have been informed about the details of the study in own language. I have understood the details about the study. I know the possible risks and benefits for me, by taking part in the study. I understand that I can withdraw from the study at any point of time and even then, I will continue to get the medical treatment as usual. I understand that I will not get any payment for taking part in this study. I will not object if the results of this study is getting published in any medical journals, provided my personal identity is not reviewed. I know what I am suppose to do by taking part in this study and I assure that I will give my full co-operation for this study. Signature/Thumb impression of the participant (Name/Address) ___________________________________ ___________________________________ ___________________________________ Name & Signature of the investigator ___________________________________ ___________________________________

28
\ïVÝ\VïVÍ] \òÝmkÂï_Ùö \u®D g«VFßE W®kªD
Amß¼Äö.
gF¡ >ïk_
g«VFßEl[ ØÃBì: ¶_â«VÄ¡õâ ¶bzxçÅçB ÃB[Ã|Ý] ïkâç¦ ïz]l[
(¼\_, ÿµ, Ö|©AD, m禥D ¼ÄòD Ö¦D) \ÅÂï »E >|©çà ÃB[Ã|Ým>_
Ãu¤B {ì gF¡.
ÖÍ> g«VFßEçB Ãu¤B xÂþB\Vª >ïk_ïçáÝ Ø>öÍm ØïVõ| Ö]_
ú¼ïuï cºï^ ÄD\>Ýç> Ø>ösÂz\V® åVºï^ s|Ý> ¼kõ|¼ïVçá
°u®ÂØïVõ¦ç\Âz å[¤. ÖÍ> g«VBßE ÄD\Í>\Vï >ïk_ï^, Ö]_ úz Øîk]ªV_
cºïÓÂz °uæÂí½B ¶ØÄáïöBºï^, ÃV]©Aï^ \uÅD å[ç\ï^ ¶çªÝmD
֩ýkÝ]_ ØïV|Âï©Ãâ½òÂþ[Ū. Öç> ÀºïáVï¼k ýÝm Ø>öÍm
ØïV^áéVD ¶_ém Àºï^ sò©Ã©Ãâ¦V_, åVºï^ Öç> cºïÓÂz ýÝmÂïVâ½
Aö¥Dý ØÄV_k>uzÝ>BV«Vï ÖòÂþ¼ÅVD. cºïÓÂz °¼>ÐD AöBs_çé
¨[ÅVKD ¶_ém í|>_ >ïk_ï^ °¼>ÐD ¼>çk ¨[ÅVKD åVºï^ cºïÓÂz c>k
>BV«Vï ÖòÂþ¼ÅVD.
g«VFßEl_ úzØÃÅsòAkìïÓÂïVª >ïk_:
ÖÍ>g«VFßEl[ ¼åVÂïD ¶®çk EþßçÄl[ ¼ÃVmD ¶®çk EþßçÄÂz
¸ÅzD c^á koçB ÀÂïk_é (¼\_, ÿµ, Ö|©AD, m禥D ¼ÄòD Ö¦D) \ÅÂï
»E >|©çà ÃB[Ã|Ým>¼é gzD.
29
ÖÍ> g«VFßE \ïVÝ\V ïVÍ] \òÝmk\çªl_\BÂï \òÝmkmçÅl_ Ãâ¦
¼\uý©A ýÂzD \òÝmkì. ¶¸\[R Eº \òÝmkì. ½. EkÄ[xïD
\BÂï \òÍm mçÅl[ ¼Ã«VEöBì ïõïÃ詸_ ÖÍ> g«VFßEçB ØÄFþÅVì.
ÖÍ> g«VFßEl_ úz Øîk>uz cºïçá ¼>ìÍØ>|Âï åVºï^ sò©ÃÃ|k>[
ïV«ðD ¶®çk EþßçÄl[ ¼ÃVmD ¶>uz ¸Åz c^á ïVéÝ]KD >ºï¹[ koçB ÀÂï
ÖÍ> (¼\_, ÿµ, Ö|©AD, m禥D ¼ÄòD Ö¦D) \ÅÂï ØÄF¥D xçÅ ØÃömD
c>¡D.
ÖÍ> g«VFßEl_ úzØîkm cºï^ sò©ÃÝç> \â|¼\ ØÃVòÝ>m Àºï^
sòDà s_çéØBM_ cºïçá, ÖÍ> g«VFßEl_ ~|Ã|Ý> \Vâ¦Vìï^. Àºï^ ÖÍ>
g«VFßEl_ úzØÃÅVsâ¦VKD cºïÓÂz þç¦Âï¼kõ½B \òÝmk c>s ¨Í>
ÃV«ÃâÄxD Ö_éV\_ Ø>V¦ìÍm þç¦ÂzD.
ÖÍ> g«VFßEl_ Àºï^ ú¼ïuï ¼kõ|\VªV_, Àºï^ ¨|Ým ØïV^á
¼kõ½B ØÃV®©Aï^: 1)
EþßçÄl[ ¼ÃVm
ÖÍ> g«VFßEB_ úz Øîk]ªV_ cºïÓÂzD, Äx>VBÝ]uzD å[ç\ï^
cõ|. ¶®çk EþßçÄl[ ¼ÃVmD ¶>[ ÃÅz c^á ïVéÝ]KD >ºï¹[ koloòÍm
EÅÍ> WkV«ªD þç¦ÂzD.
30
ÖÍ> g«VFßE úz Øîk]ªV_ cºïÓÂz ÃV]©Aï^ °mD °uæ kVF¸_çé.
\BÂï \òÍm >|©¸uz cB¼BVï©Ã|ÝmD \òÍm ¶ºþïöÂï©Ãâ¦m. ¨Í> s> ÃV]©AD
°uæVm ¨[Ã>uz ¶ºþÃöÂï©Ãâ¦m.
ÖÍ> g«VFßEl_ úz Øîk>uïVï cºïÓÂz Ä[\VªD °mD kwºï©Ã¦
\Vâ¦Vm.
ÖÍ> g«VFßEB_ cºïám ú¼ïuAD >ºïçá© Ãu¤B >ïk_ïÓD «ïEB\Vï
çkÂï©Ã|D.
ÖÍ> g«VFßEl[ x½¡ïçá Àºï^ sòD¸ªV_, ¨ºï¹¦tòÍm ØÃu®ÂØïV^áéVD.
ÖÍ> g«VFßEloòÍm, cºï^ sò©ÃÝ]u¼ïuà ¨Í¼å«xD séþÂØïV^áéVD.
ÖÍ> g«VFßEl_ Àºï^ ú¼ïuï ¼kõ|D ¨ª ¼ïVòþ¼ÅVD. Àºï^ ÖÍ>
¼kõ|¼ïVÓÂz ÄD\>D ¶¹Âï \®ÂïéVD. ¶ËkV® \®Ý>VKD zçÅÃV| °mD
Ö_éV\_ cºïÓÂz EÅÍ> \òÝmkßEþßçÄ Ø>V¦ìÍm ¶¹Âï©Ã|D. ÖÍ> g«VFßE
z¤Ým cºïÓÂz Äͼ>ïD °mD ÖòÍ>V_ Öm z¤Ým x>[ç\ g«VFßEBVáö¦D
¼ïâ| ¶¤ÍmØïV^áéVD.
\òÝmkì. ¶¸\[R Eº (¶çé¼ÃE ¨õ 9999636613)
g«VFßE kaïVâ½
\òÝmkì. \òÝmkì ½. EkÄõxïD (¶çé¼ÃE ¨õ 9442505567)
\òÝmkì. ¶M ´ÃV. ØÛ (¶çé¼ÃE ¨õ 9655035791)
31
\ïVÝ\V ïVÍ] \òÝmkÂï_Ùö \u®D g«VFßE W®kªD Amß¼Äö.
gF¡ ΩA>_ ýkD
g«VFßEl[ ØÃBì: ¶_â«VÄ¡õâ ¶bzxçÅçB ÃB[Ã|Ý] ïkâç¦ ïz]l[
(¼\_, ÿµ, Ö|©AD, m禥D ¼ÄòD Ö¦D) \ÅÂï »E >|©çà ÃB[Ã|Ým>_
Ãu¤B {ì gF¡.
ÖÍ> gF¡ Ãu¤Bsk«ºï^ ¨ªÂz Ø>ösÂïÃ⦪. Ömz¤Ým ¨[Ðç¦B ØÄVÍ>
Ø\Val¼é¼B ¨ªÂzsköÂï©Ãâ¦m. Ömz¤Ým Äͼ>ïºïáoòÍm Ø>¹¡
Øîk>uïVª kVF©AD ¨ªÂz ¶¹Âï©Ãâ¦m. \òÝmkgF¡ïÓÂz© ¸[A cöBEþßçÄ
¶¹Âï©Ã|D ¨[Ã>çª ¶¤¼k[. ¨[Ðç¦BEþßçÄÂz© ÃV>ïD °mDÖ_éV\_,
ÖÍ>g«VFßEÂïVª ÄD\>Ýç> \®©Ã>uzD ¨ªÂzcöç\¥õ| ¨[Ã>çª åV[ ¶¤¼k[.
ÖÍ>g«VFßEl[ sk«ºï^ \u®D x½¡ï^ \òÝmk ¶¤sB_ ¼åVÂïÝ]uïVï \â|¼\
ÃB[Ã|Ý>©Ã|D ¨[Ã>uzcâÃâ|, ¶Ý>çïBsk«ºï^ \u®D x½¡ïáÂzÝ >禼BmD
ØÄFB \V⼦[ ¨ª c¦[Ã|þ¼Å[.
---------------------------------- gþBåV[ ÖÍ> g«VFßEl_ ú¼ïuÃ>uzß ÄD\>D
¶¹Âþ¼Å[.
ú¼ïuÃkì ÄVâEBVáì
çïØBV©ÃD/ ØÃòs«_ ¼«çï:
ØÃBì/ xïkö:
g«VFßEBVáö[ çïØBV©ÃD:
xïkö:
¼>]: