Embed Size (px)
Citation preview

Approach to abdominal wall hernia by : younis zainal khaleel kufa college of medicine .. Medical student .. Stager

Topics of presentation
• 1 . All types of abdominal wall hernia other than inguinal and femoral (previously discussed ).
• 2 . Divarication of the rectus abdominis and incisional hernia .

Those are …
Incisional hernia : at the site of previous incision

According to there incidence

Anterior abdominal wall hernia

Umbilical herniaMany different condition represent
umbilical hernia , they differ by each other in there pathophysiology and age of incidence .
1- Omphalocele & gastrochisis ( at birth)
2-Umbilical hernia of infants and children
3- acquired umbilical hernia (adult and older)
*

omphalocele1.. Omphalocele and gastrochisis.-1: 6000 birthsGastroschisis: It is the congenital anomaly
characterized by a defect in the anterior wall through which the abdominal contents freely fall.
Omphalocele: It is a congenital birth defect that involves the umbilical cord itself, and the organs remain enclosed in the visceral peritoneum.
-There is some debate as to whether gastroschisis represents a separate entity or is simply an Omphalocele with ruptured membranes, but the debate of little importance because the same principles of treatments.

Pathophysiology of omphaloceleAn omphalocele is caused by error in the embryonic development
↓Normal development there are 3 distinct portions formed –
foregut, midgut & hindgut↓
At early fetal life much of midgut is temporarily herniated outside the abdomen at the umbilicus
↓The midgut later re-enters the abdomen and opening of
abdominal wall is closed↓
*Failure for the midgut to return and re-enter the abdomen↓
Omphalocele is formed

• Management of omphalocele• Small defects : may be closed primarily soon after
birth• Large defect : a more substantial problem and four techniques have been described: * non-operative therapy, * skin flap closure, *staged closure and * primary closure.
omphalocele

Umbilical hernia2.. Congenital umbilical hernia

Umbilical hernia

Pathophysiology of congenital umbilical hernia
During development of fetus↓
A small opening is present in the abdominal muscles, so that the umbilical cord can pass through, connecting mother to baby.
↓Usually the abdominal opening closes.
↓(After birth) Sometimes these muscles do not meet- creating a
small opening.↓
A loop of intestine can move into the opening between abdominal muscle and cause and hernia.

age : usually at birth , but may not be noticed until umbilical cord has separated & healed or it stay so small and not noticed until it enlarged months later.Symptoms : usually Symptomless, but mother anxiety is
common , intestinal obstruction is extremely rare.Signs :_ Have a classical conical shape or hemispherical ._ size ( range from 0.5_10cm) .They reduce spontaneously when the child lies down and
become tense when the child cries.Cough impulse:expansile cough impulse is invariably present.Composition : are soft, compressible and easy to reduce,
They usually contain bowel and so may be resonant to percussion
Congenital umbilical hernia

• Natural history :The vast majority of congenital umbilical hernia disappear spontaneously during the first few years of life (up to 2 year), It is difficult to believe that a large defect will close over in an active child, but this is the usual
course of events.
Congenital umbilical hernia

umbilical hernia
Treatment of infantile umbilical herniaConservative treatment indicated ↓ 2 years; Just reassurance of the
parents, as 95% of hernias will disappear spontaneously and rarely strangulate .
Surgical : If persists at 2 years of age or older it is unlikely to resolve and herniorrhaphy is indicated.

UMBILICAL HERNIA IN ADULTS

UMBILICAL HERNIA IN ADULTSA true umbilical hernia comes through the
umbilical scar. It is not common in adults and usually secondary to raised intra-abdominal pressure. but the common causes of an acquired umbilical hernia are pregnancy and ascites. The local physical signs of the hernia are identical to those described for the congenital variety.

Paraumbilical hernia

Paraumbilical hernia

Paraumbilical hernia• is a protrusion through the linea alba,• 1. just above (supraumbilical hernia)• 2. just below the umbilicus (infraumbilical)
hernia)

• M:F 1:5 therefore its common in woman who are *overweight
*ages of 35 and 50 *repeated pregnancy .• Symptoms : The commonest symptoms are
discomfort and a swelling • some time they present complaining of pain or
discomfort around the umbilicus, made worse by prolonged standing or strenuous exercise , and if its large one cause a dragging pain because of its weight .
• Strangulation is common , but the usual contents in this case are extraperitoneal fat or omentum, so even strangulation occur, the bowel is not obstructed.
Paraumbilical hernia

Paraumbilical herniaGeneral examination The patient is quite likely
to be obese and may have other herniae and generalized abdominal wall laxity.
Shape :classically make the umbilicus crescent shape if its so near the umbilicus but not in obese pt and in large one .
Composition The lump is firm as it usually contains omentum. If it contains bowel, it is soft and resonant to percussion.
If the hernia can be reduced, the firm fibrous edge of the defect in the linea alba is easy to feel. It may vary in size from a few millimetres in diameter to a defect big enough to admit your hand.

Management May strangulate so need surgery
Paraumbilical hernia

Which type of hernia here ??

And what's this ??

Epigastric hernia• occurs through the linea alba anywhere between the
xiphoid process and the umbilicus, usually midway between these structures.
• Its usually as a protrusion of extraperitoneal fat that why called (fatty hernia of the linea alba) , The mouth of the hernia is rarely large enough to permit a portion of hollow viscus to enter it; consequently, either the sac is empty or it contains a small portion of greater omentum.

Pathophysiologyit is more likely a result of a weakened linea alba due to abnormal decussation of the fibres of the aponeurosis
That why an epigastric hernia is the direct result of asudden strain tearing of the interlacing fibres of the linea
alba. and the patients are often manual workers between 30 and
45 years of age.
Epigastric hernia

Clinical features• Symptomless• Painful (attacks of local pain, worse on physical
exertion, and tenderness to touch and light clothing)
• Referred pain The pain is often associated with eating, so the patient calls it ‘indigestion’ and makes a self-diagnosis of peptic ulceration.
• A likely explanation for this is Referred pain that the fatty hernia is ‘nipped’ by the linea alba on leaning forward in the sitting position adopted at the dining table.
Epigastric hernia

• On examination_feel firm, don't usually have a cough
impulse _cannot be reduced._sometimes impossible to distinguish
them from lipoma_ only the typical position suggesting
the correct diagnosis
Epigastric hernia

Treatment : indicated when a considerable symptom occur .
Epigastric hernia

Which type of hernia here??

Spigelian hernia• hernia occurring at the level of the arcuate line • The sac, lie beneath the internal oblique muscle, where
it is virtually impalpable it advances through that muscle and spreads out like a mushroom between the internal and external oblique muscles and gives rise to a more evident swelling.

Spigelian herniaClinicallySo rare , usually over 50 years of age, equal in M & F .Typically, a soft, reducible mass will be encountered lateral to the rectus muscle and below the umbilicus Dx : By US , CT . Treatment : need operation

Posterior wall hernia
Superior lumber herniaInferior lumber hernia (more common)

lumber hernialumbar hernias are usually occur secondary to
renal operations, when extensive incisional sacs may be present
Treatment: operation

Pelvic hernia
These are rare types of hernia.1. Obturator 2. Gluteal 3. Sciatic

Obturator herniawhich passes through the obturator canal,women : men 6:1. Most patients are over 60 years of age.The swelling is liable to be overlooked because it is covered
by the pectineus muscle

It seldom causes a definite swelling, but if the limb is flexed, abducted and rotated outwards, the hernia sometimes becomes more apparent.
but can cause intestinal obstruction with nausea & vomiting.
And the presentation usually as a strangulated hernia , In more than 50% of cases of strangulated obturator hernia, pain is referred along the obturator nerve by its geniculate branch to the knee.
On vaginal or rectal examination the hernia can sometimes be felt as a tender swelling in the region of the obturator foramen.
Treatment Operation is indicated
Obturator hernia

Gluteal and sciatic hernias• A gluteal hernia passes through the greater
sciatic foramen• A sciatic hernia passes through the lesser
sciatic foramen.

Presentation : sciatica , local pain , swelling .
Differential diagnosis must be made between these conditions and:
• a lipoma under the gluteus maximus;• a tuberculous abscess;• a gluteal aneurysm.All doubtful swellings in this situation should be explored byoperation.
Gluteal and sciatic hernias

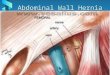
• An abdominal incisional hernia is a hernia through an acquired scar in the abdominal wall, caused by a previous surgical operation or injury.
• Scar tissue stretches progressively if subjected to constant stress.
Incisional hernia

Incisional herniaoccurs most often in•obese individuals•postoperative abdominal distension .•Postoperative infection or haematoma .•operations for peritonitis because, as a rule, the wound becomes infected.• There may be a history of factors likely to weaken
the abdominal musculature, such as chronic cough or steroid therapy.
Weakness Often the event passes unnoticed if the skin wound remains intact after the stitches have been removed.

Clinical presentation may occur through 1. a small portion at the lower end or frequently as a diffuse
bulging Symptoms : The commonest symptoms are a lump and pain.
Intestinal obstruction can occur, causing distension, colic, vomiting, constipation and severe pain in the lump.
Those through a lower abdominal scar, usually increases steadily in size and more and more of its contents become irreducible .
Nevertheless, most cases of incisional hernia are asymptomatic and broad-necked and do not need treatment Therefore they are rarely strangulate.
Incisional hernia

ExaminationThe common findings are a lump with
an expansile cough impulse, beneath an old scar.
Incisional hernia are not unusual irreducible, the defect being plugged withadherent omentum.
Incisional hernia

Incisional herniaTreatment1.Palliative : An abdominal belt is sometimes
satisfactory, especially in cases of a hernia through an upper abdominal incision.
2.OperationPostoperative care* nil by mouth and intravenous fluids until bowels have functioned*Early ambulation and gentle physical exercise to be encouraged.*patient should not resume strenuous exercise for several weeks.Result of operation (recurrence )Without mesh .. 30_50% , With mesh .. 10%

This is separation of the rectus abdominis muscles with extenuation of the linea alba, from xiphisternum to umbilicus and occasionally below.
Divarication of the rectus abdominis

Divarication of the rectus abdominis
① in children may be seen in the first few years.
_The condition usually improves and eventually disappears as the child grows.
The only clinical concern is the cosmetic disfigurement,
as strangulation is impossible.

Divarication of the rectus abdominis
② in adults, in women during and immediately after childbirth. There
may be a wide separation of the muscles, with stretched overlying abdominal skin.
As abdominal tone recovers, the defect closesbut may become permanent after multiple pregnancies.
2 way to examine :1.. Make the recti to relax :the patient lying supine The
examiner may be able to push a hand into the abdominal cavity .
2.. Make the recti fully tense :ask the patient to raise the head and legs together or other way to tense the recti , The thinned-out linea alba then bulges, producing a visible swelling.

• Treatment• An abdominal belt is all that is
required. As there is no risk of strangulated intestinal contents.
Divarication of the rectus abdominis

Important messages ,Review slide ..

Is this hernia ??

Is this hernia ??