Embed Size (px)
Citation preview
Whānau and
personalising end-
of-life care:
Translating research
for practice
Hospice New Zealand Conference, Wellington, 29/10/2014
Lesley Batten, Maureen Holdaway, Marian Bland, Jean Clark, Simon Allan, Bridget Marshall, Delwyn Te Oka, Clare Randall Te
Wakahuia Manawatu Trust
Project aims
Over three years to:
A. Investigate if / how the addition of ‘cultural goals’ of care in the Liverpool Care Pathway for the Dying Patient (LCP) guides the delivery of culturally appropriate end-of-life (EOL) care for adult Māori within the MDHB region
B. Explore the experiences and perspectives of EOL care of whānau whose relatives have received care guided by the LCP since the inclusion of the ‘cultural goals’
C. In partnership with Māori communities, stakeholders, and providers, develop and pilot a culturally appropriate New Zealand version of the LCP EOL pathway
Research overview
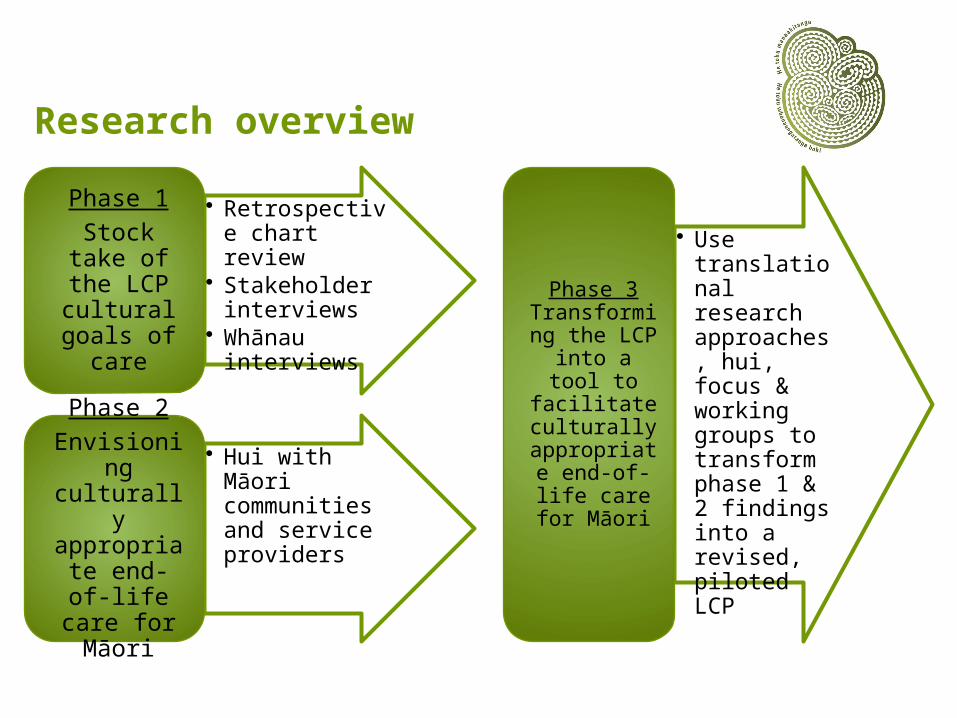
• Retrospective chart review
• Stakeholder interviews
• Whānau interviews
Phase 1Stock take of the LCP
cultural goals of
care
• Hui with Māori communities and service providers
Phase 2Envisioning culturally
appropriate end-of-life care for Māori
• Use translational research approaches, hui, focus & working groups to transform phase 1 & 2 findings into a revised, piloted LCP
Phase 3 Transforming the LCP into
a tool to facilitate culturally
appropriate end-of-life care for Māori
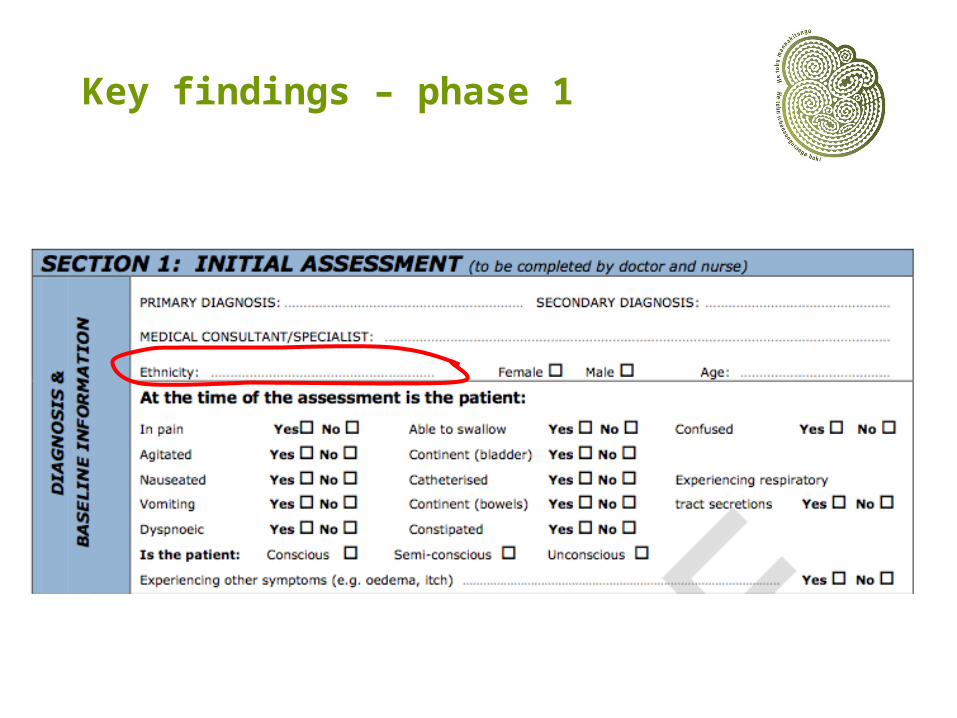
Key findings – phase 1
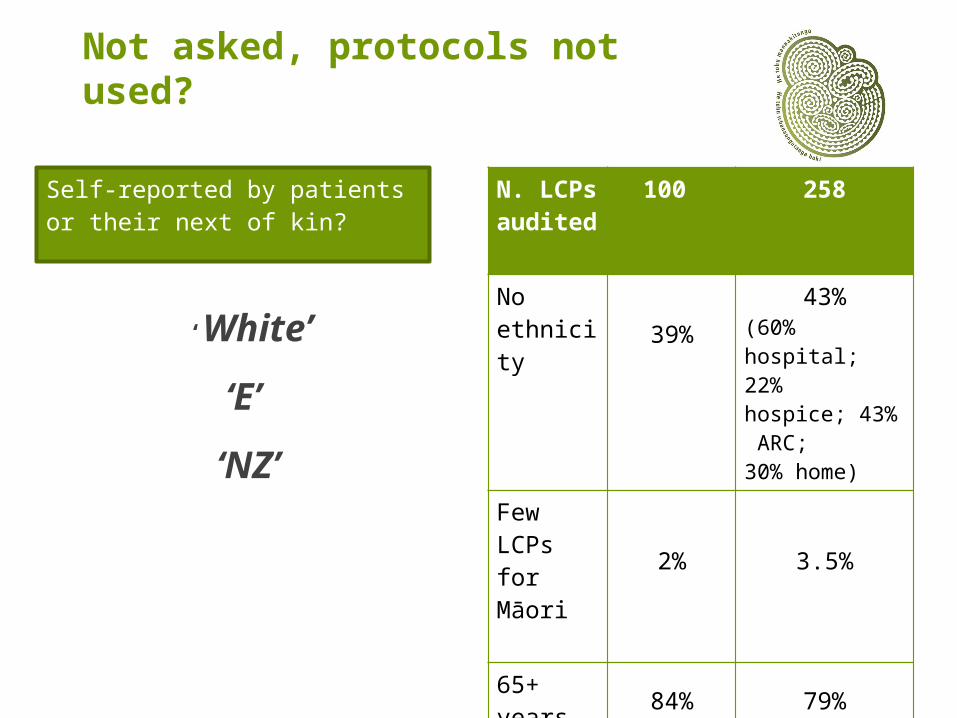
Not asked, protocols not used?
‘White’
‘E’
‘NZ’
N. LCPs audited
100 258
No ethnicity
39% 43%(60% hospital; 22% hospice; 43% ARC; 30% home)
Few LCPs for Māori
2% 3.5%
65+ years 84% 79%
Self-reported by patients or their next of kin?
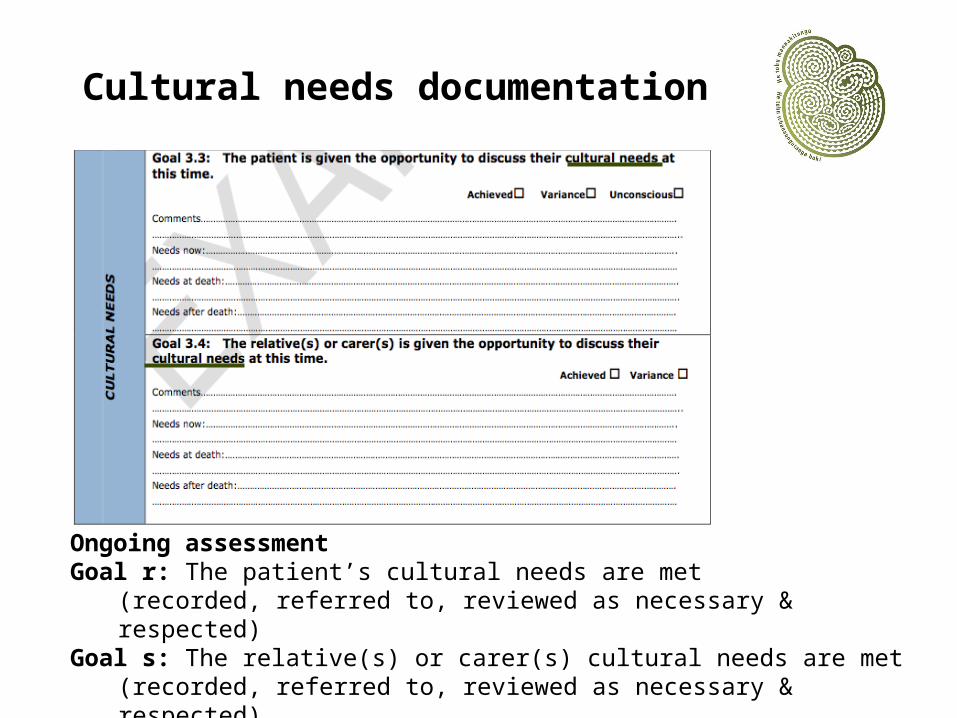
Cultural needs documentation
Ongoing assessmentGoal r: The patient’s cultural needs are met
(recorded, referred to, reviewed as necessary & respected)Goal s: The relative(s) or carer(s) cultural needs are met
(recorded, referred to, reviewed as necessary & respected)
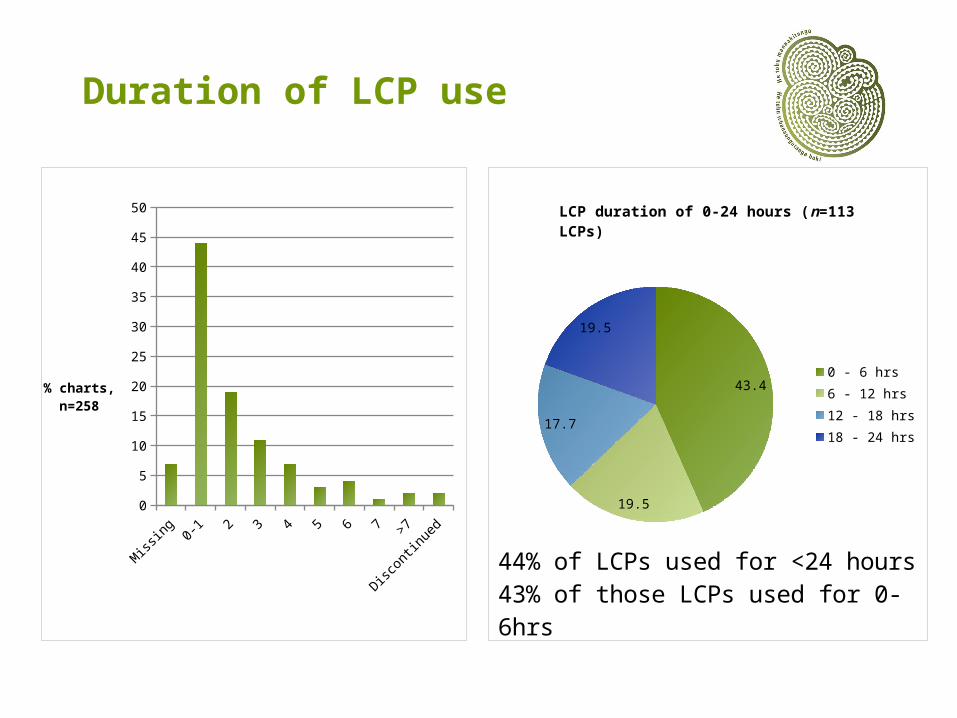
Duration of LCP use
Missin
g0-
1 2 3 4 5 6 7>7
Disco
ntin
ued
0
5
10
15
20
25
30
35
40
45
50
% charts,n=258
43.4
19.5
17.7
19.5
0 - 6 hrs6 - 12 hrs12 - 18 hrs18 - 24 hrs
44% of LCPs used for <24 hours43% of those LCPs used for 0-6hrs
LCP duration of 0-24 hours (n=113 LCPs)
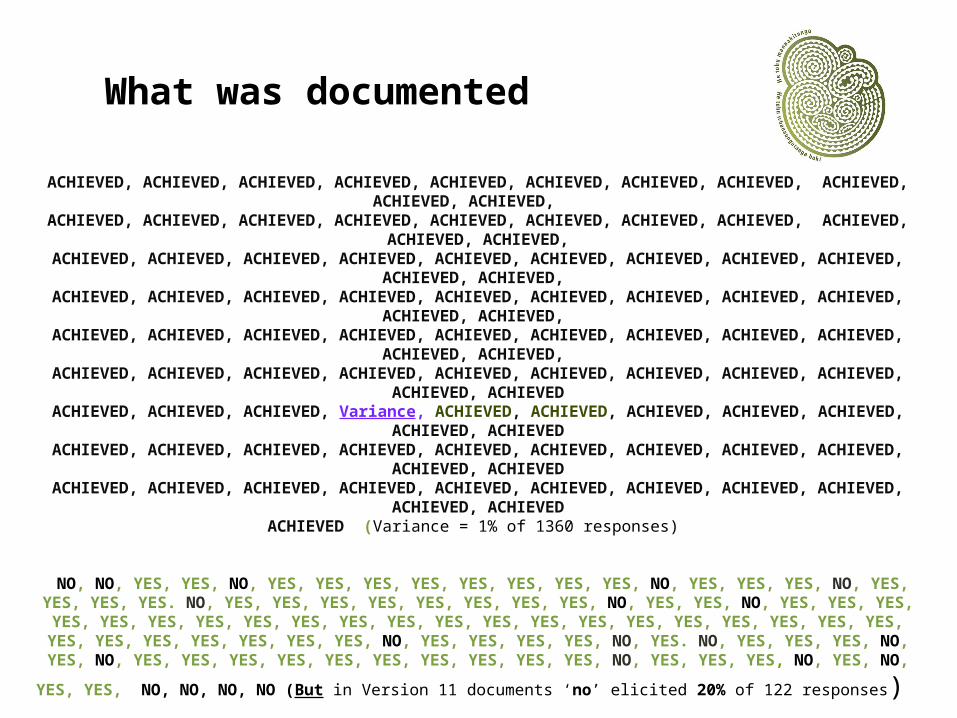
What was documented
ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED,
ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED,
ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED,
ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED,
ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED,
ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED
ACHIEVED, ACHIEVED, ACHIEVED, Variance, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED
ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED
ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED, ACHIEVED
ACHIEVED (Variance = 1% of 1360 responses)
NO, NO, YES, YES, NO, YES, YES, YES, YES, YES, YES, YES, YES, NO, YES, YES, YES, NO, YES, YES, YES, YES. NO, YES, YES, YES, YES, YES, YES, YES, YES, NO, YES, YES, NO, YES, YES, YES, YES, YES,
YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, NO, YES, YES, YES, YES, NO, YES. NO, YES, YES, YES, NO, YES, NO, YES, YES, YES, YES, YES, YES, YES, YES, YES, YES, NO, YES, YES, YES, NO, YES, NO, YES, YES, NO, NO, NO,
NO (But in Version 11 documents ‘no’ elicited 20% of 122 responses)
‘nil identified’, ‘nil identified’ Minimal variance documentation
Relatives’ goals achieved even when not present
Confidence, competence
Looking at the cultural goals and the audits, I do find it really interesting that not much is often written there. And I even see ‘no’, you know, “what are your cultural needs?” “None”. And I find that really interesting.
Interviewer: Why do you think that is?
I just wonder whether the person who’s doing the [cultural needs] assessment doesn't have the confidence to actually ask probing questions to pull it out of the person. (Int. 4)
Blocks to cultural care
Image: With permission – KB Trout Productions
Phase 2: Key findings
Whānau
centred
Communication &
relationships
Integrated, seamless, navigated services
Organisational commitment
Whānau roles
The whānau were being advised and supported from here and from our [rural] local GPs, from our [rural] hospital. They were well in control, they were able to plan, they were able to watch that, with this whānau and their loved one that the tikanga and the wairua was maintained and intact and that the mana of their loved one, and for all of them as a whānau too, was being appropriately attended to and maintained. (FG. 6)
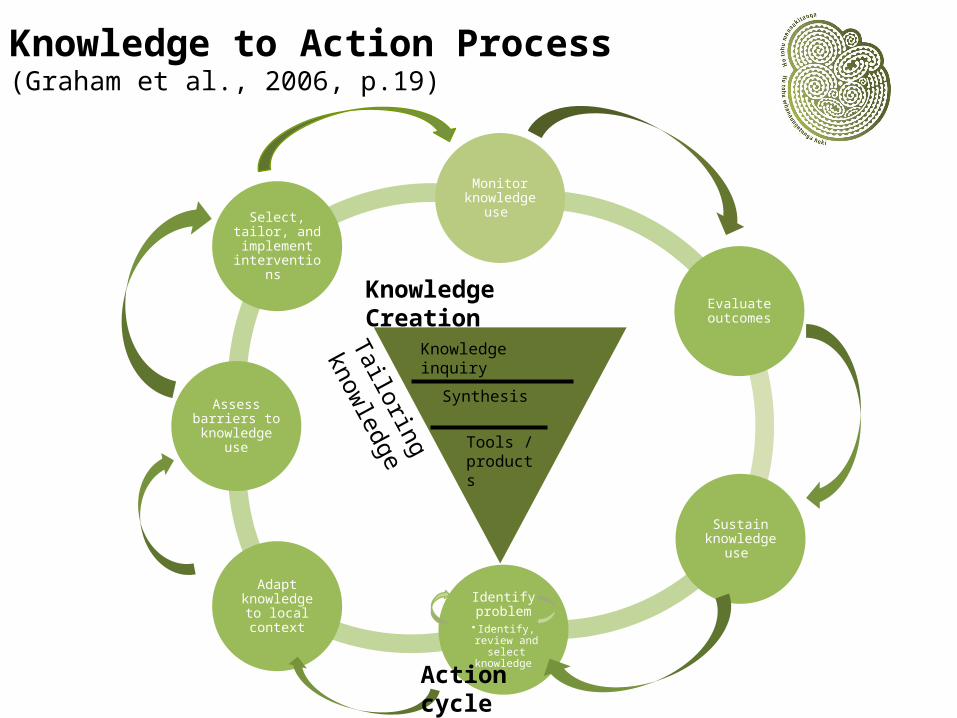
Monitor knowledge
use
Evaluate outcomes
Sustain knowledge
use
Identify problem
• Identify, review and select knowledge
Adapt knowledge
to local context
Assess barriers to knowledge
use
Select, tailor, and
implement interventions
Knowledge inquiry
Synthesis
Tools /products
Knowledge Creation
Tailoring
knowledge
Action cycle (application)
Knowledge to Action Process (Graham et al., 2006, p.19)
Objectives developed from phases 1 & 2 – clinical services
The importance of the cultural component of personalised care is recognised
Personalised goals of care are assessed
Appropriate responses to assessed personalised goals are actioned (and evaluated)
The person receiving are feels safe
The family or whānau feel safe
The clinical staff providing care feel safe in the provision of that care
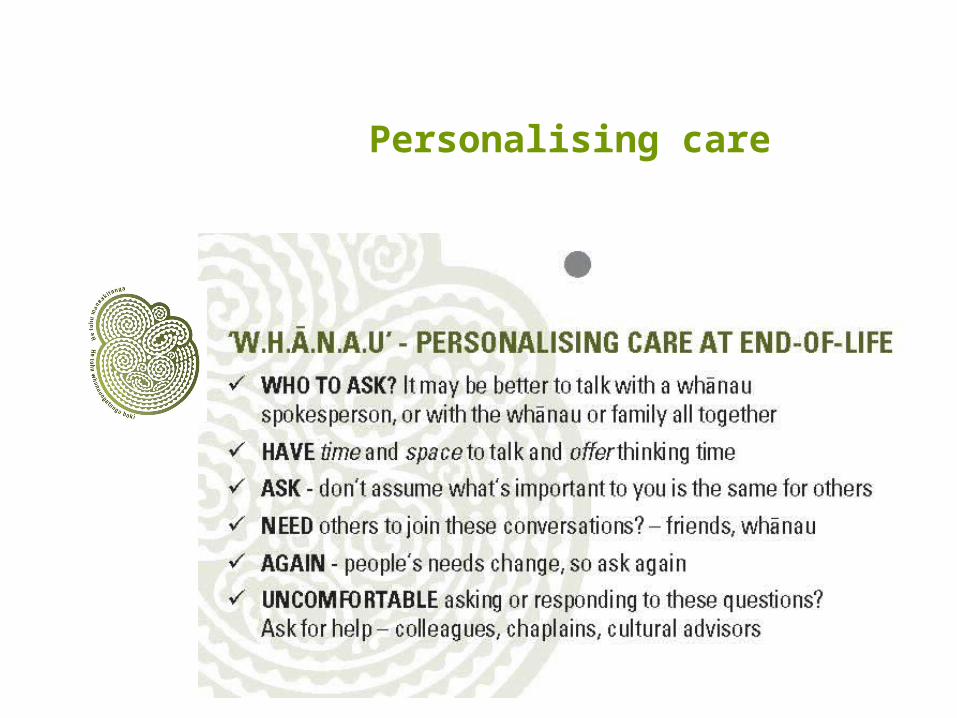
Personalising care
Conversation starter

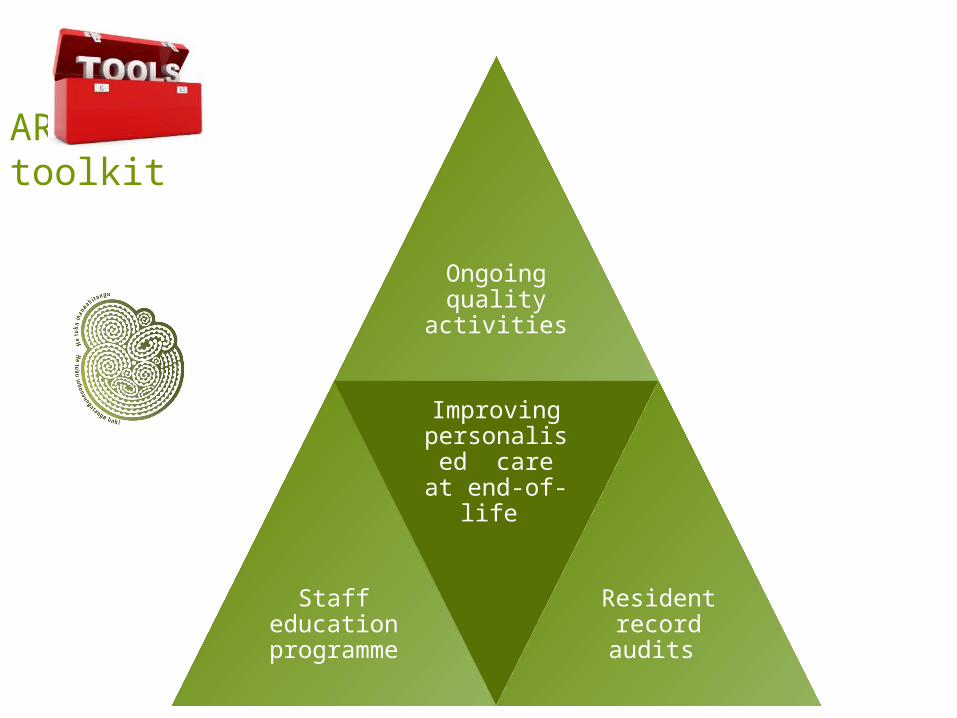
ARC toolkit
Pilot 1
Undergraduate nurses’ workshop
Pilot 2
Revised LCP
Pilot 3
ARC toolkit
Ongoing quality
activities
Staff education
programme
Improving personalised care at end-of-life
Resident record audits

Staff feedback
“An eye opening to ways of discussing end-of-life care”
“Exposing parts of my practice I had become complacent in. Learning the perspective of others and that I’m not always right!”

Workshop for undergraduate nurses
LCP revisions piloted
Standardised ethnicity documentation
Family and whānau involvement in care
Whānau spokesperson
Personalised care needs
Cultural and spiritual advisors
Combined spiritual and cultural care goals – personalising care
Images
⨷ Variance reporting style
Ma te rongo, ka mohio
Ma te mohio, ka marama
Ma te marama, ka matau
Ma te matau, ka ora
Through listening comes awareness, through awareness comes understanding, through understanding, comes knowledge, through knowledge comes life and wellbeing
![Electrical Physical Layer Application Notes - svn.ipd.kit.eduE2%84%A2%20... · [EMC10] FlexRay Communication System – Electrical Physical Layer EMC measurement specification, Version](https://img.pdfslide.us/doc/110x75/5a79c96a7f8b9ab05f8c6047/electrical-physical-layer-application-notes-svnipdkitedu-e284a220emc10.jpg)


















![Applied Information and Communication Technology Assessment Unit A2 7 · 2020-01-23 · Assessment Unit A2 7 assessing Unit 7: Investigating Systems [A6J11] THURSDAY 23 MAY, MORNING](https://img.pdfslide.us/doc/110x75/5f58a24eb99f99342e59ddc9/applied-information-and-communication-technology-assessment-unit-a2-7-2020-01-23.jpg)