Embed Size (px)
Citation preview
Prof.K.H.NOORUL AMEEN’s UnitDr.E.Thirulogachandar
A 20 yr old male admitted with c/o headache-20 days Double vision 7 days Diff in swallowing – 7 days Nasal regugitation-7 days Diff in getting up from bed-1 week
HOPI: Apparently normal 3 weeks before.
H/o headache-20 days bifrontal dull aching continuous not ass. with nausea/vomiting
No h/o feverNo h/o seizures,syncope,trauma h/o double vision 1 week ,binocular more on
lateral gaze and down gaze h/o diff in swallowing both solids and liquids
h/o nasal regurgitationh/o diff. in speakingh/o diff in getting from squatting posture h/o diff in lifting arm above shoulderh/o flail limbs+No h/o diurnal variationNo h/o radicular pain or other sensory
disturbances No h/o autonomic or bladder disturbances
Past history: h/o jaundice 2 yrs before and taken native treatment
no h/o food poisoning,dysentry,recent vaccination
Personal history: nil significant
Family history:nil significant
O/E pt conscious, oriented, afebrile, anaemia+ no
jaundice,cyanosis,clubbing,lymphadenopathy no pedal odema no neurocutaneous markers,no nerve
thickening neck stiffness+Vitals:PR-82/min,BP-120/76mm Hg,RR-16/min
Higher mental functions: conscious oriented to time place and person Rt.handed person speech –lingual and gutteral dysarthria attention-normal calculation-normal behaviour-normal memory-normal
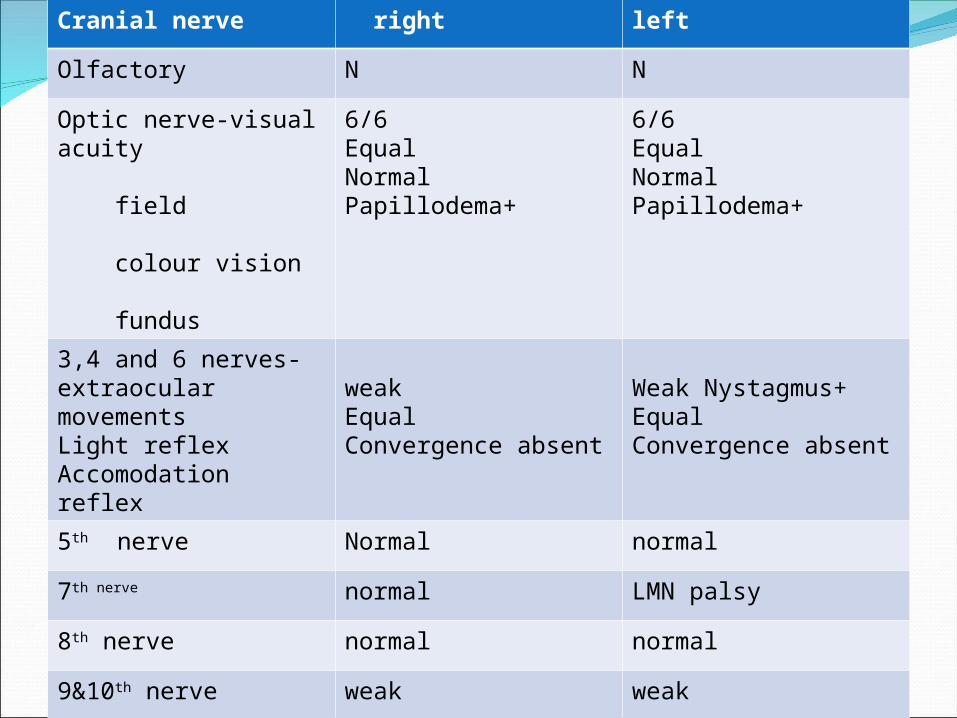
Cranial nerve right left
Olfactory N N
Optic nerve-visual acuity field colour vision fundus
6/6EqualNormalPapillodema+
6/6EqualNormalPapillodema+
3,4 and 6 nerves- extraocular movementsLight reflexAccomodation reflex
weakEqualConvergence absent
Weak Nystagmus+EqualConvergence absent
5th nerve Normal normal
7th nerve normal LMN palsy
8th nerve normal normal
9&10th nerve weak weak
11th nerve weak weak
12th nerve - LMN palsy
Motor system Bulk –equal Tone-hypotonia in UL &LL Power-proximal weakness in UL&LL
(4-/5) DTR-absent plantar-flexor both sides
Sensory system –normal
Cerebellum-normalAutonomic nervous system-normalSpine&cranium-normal
Other system: CVS-S1 S2 normally heard no murmur RS- NVBS no added sounds Abdomen-soft; no organomegaly
Problems : insiduous onset over 20 days
1.Headache2.Asymmetrical multiple cranial nerve palsies3.Proximal weakness of UL&LL of LMN type4.Neck stiffness5.Bilateral papillodema
Provisional diagnosis: BASAL MENINGITIS -?TB
Neurogist opinion?Demyelination-/NMJ disorder?Basal meningitis –Tb started on empirical ATT with steroids After imaging and CSF analysis reviewed advised to continue ATT
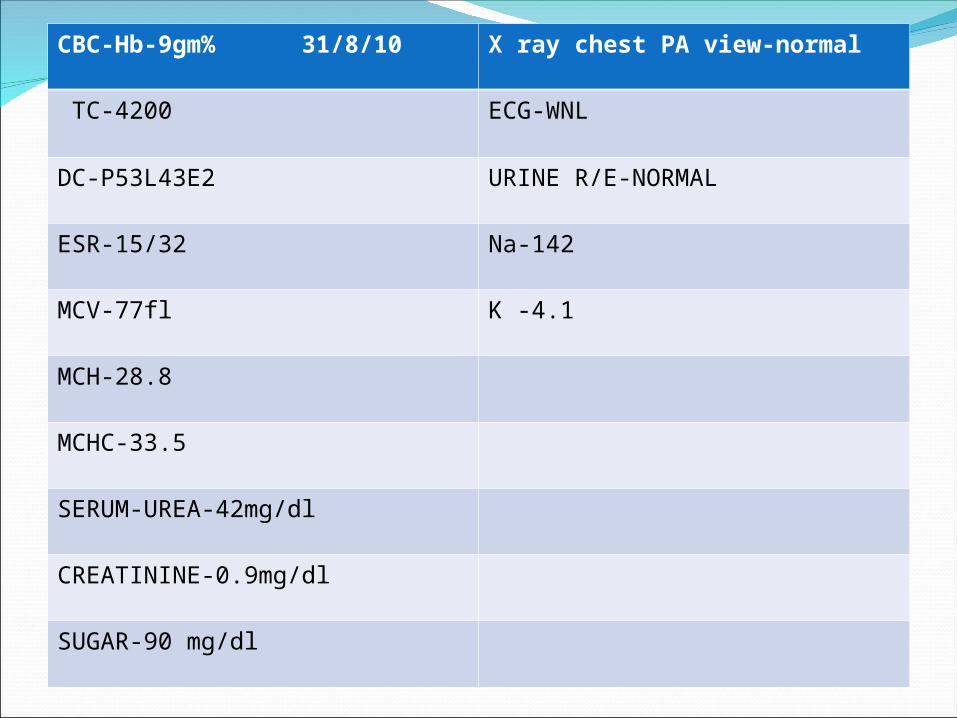
CBC-Hb-9gm% 31/8/10 X ray chest PA view-normal
TC-4200 ECG-WNL
DC-P53L43E2 URINE R/E-NORMAL
ESR-15/32 Na-142
MCV-77fl K -4.1
MCH-28.8
MCHC-33.5
SERUM-UREA-42mg/dl
CREATININE-0.9mg/dl
SUGAR-90 mg/dl
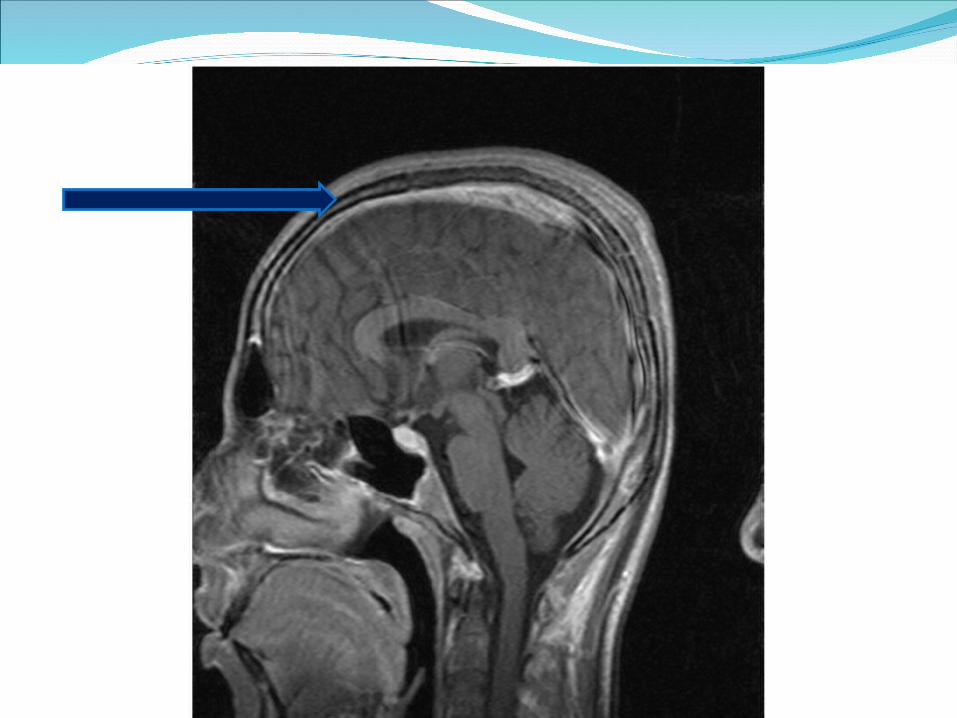
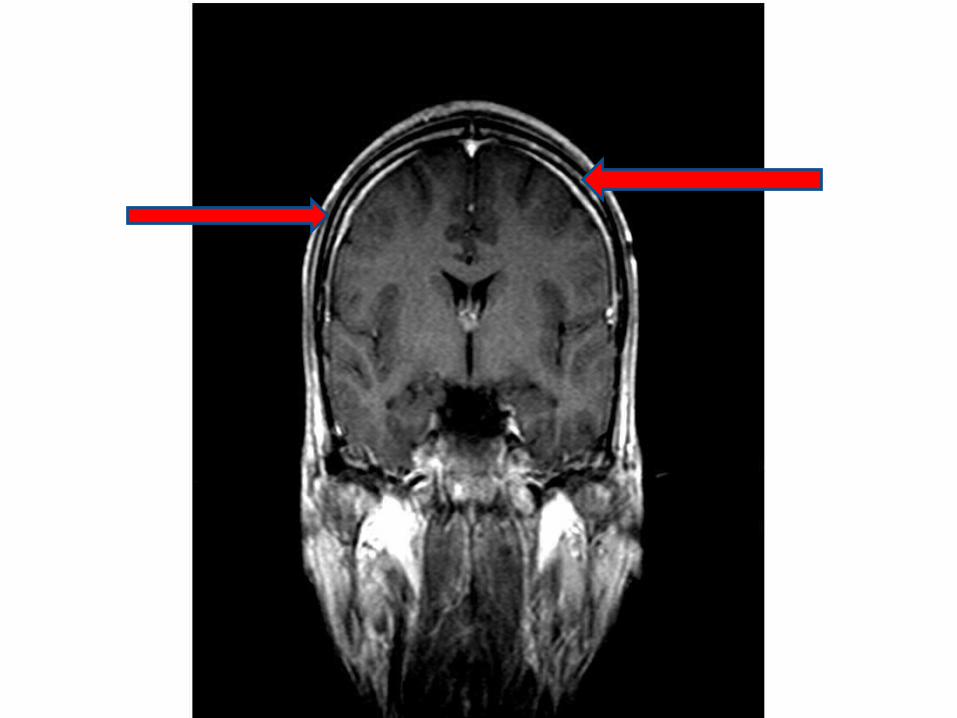
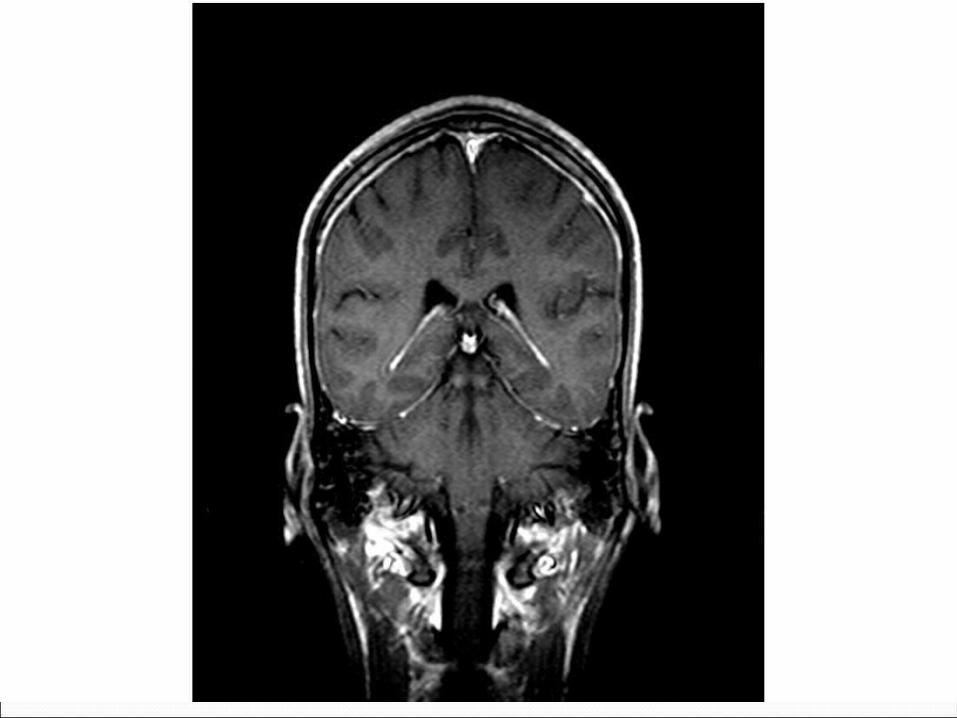
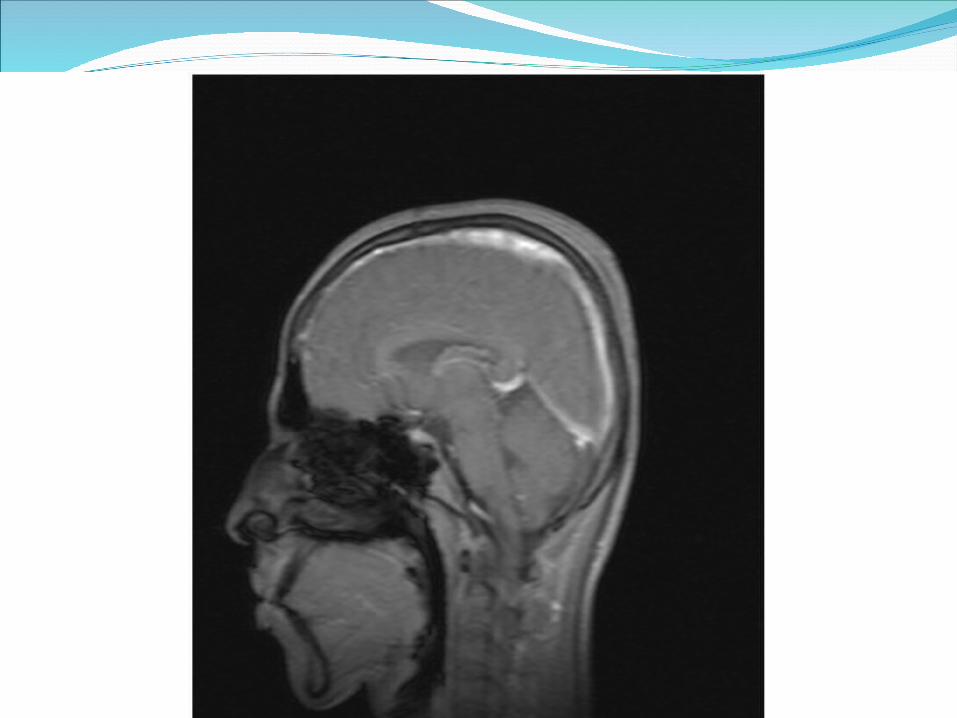
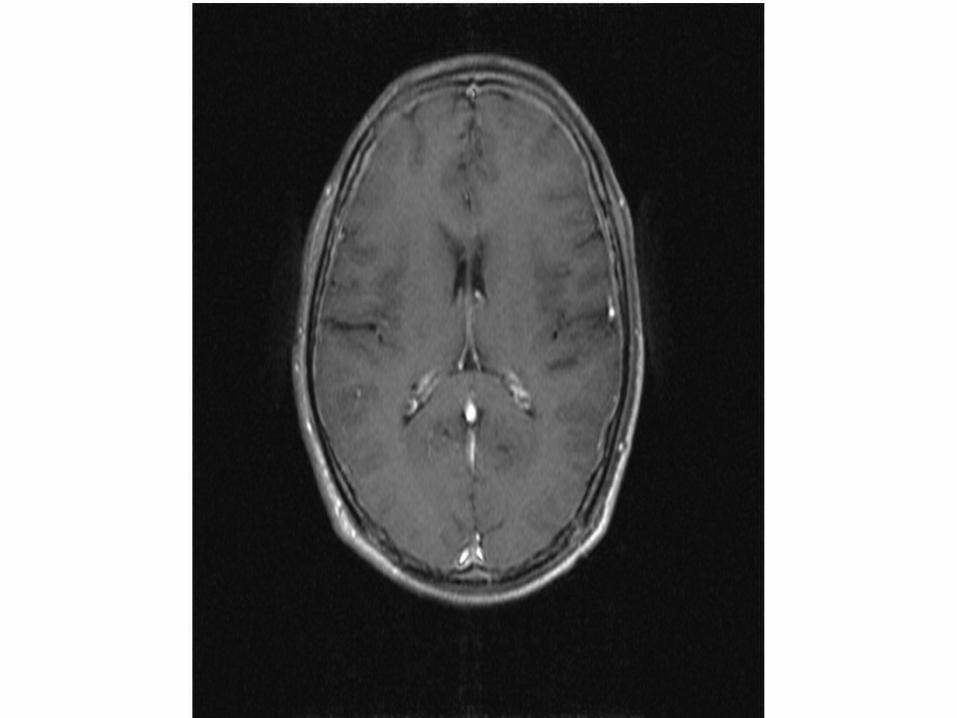
MRI BRAIN T1 weighted image and contrast: Diffuse pachymeningeal enhancement
bilaterally and subarachnoid space in optic nerve sheath appears prominent
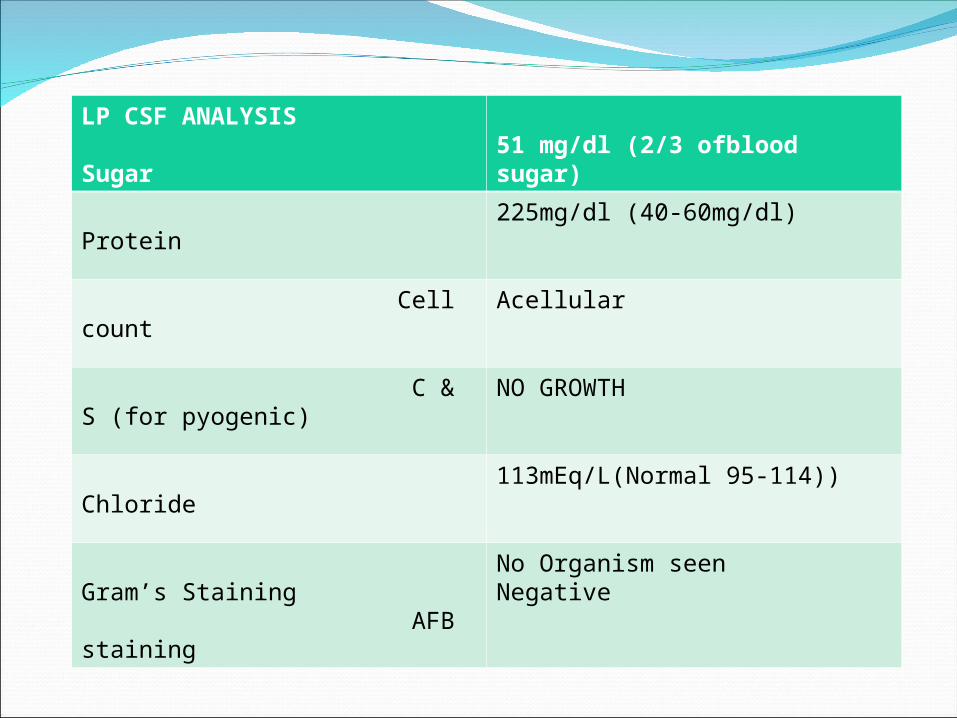
LP CSF ANALYSIS Sugar 51 mg/dl (2/3 ofblood sugar)
Protein 225mg/dl (40-60mg/dl)
Cell count Acellular
C & S (for pyogenic)
NO GROWTH
Chloride 113mEq/L(Normal 95-114))
Gram’s Staining AFB staining
No Organism seenNegative
Pt improved with ATT and steroidsCranial nerve palsies improved except 6th
nervePapillodema-resolving
But he developed clinically severe anamia and had mild splenomegaly over a period of 7 days later it became moderate ,no lymphadenopathy.
DD for diffuse dural enhancement1.Bacterial infections2.Non-infectious-Calavarial metastasis Extensive subdural
haematoma3.Low intracranial pressure states4.Hypertrophic cranial pachymengitis5.Wegner’s granulomatosis6.Multiple sclerosis7.Secondaries –breast/prostate carcinoma
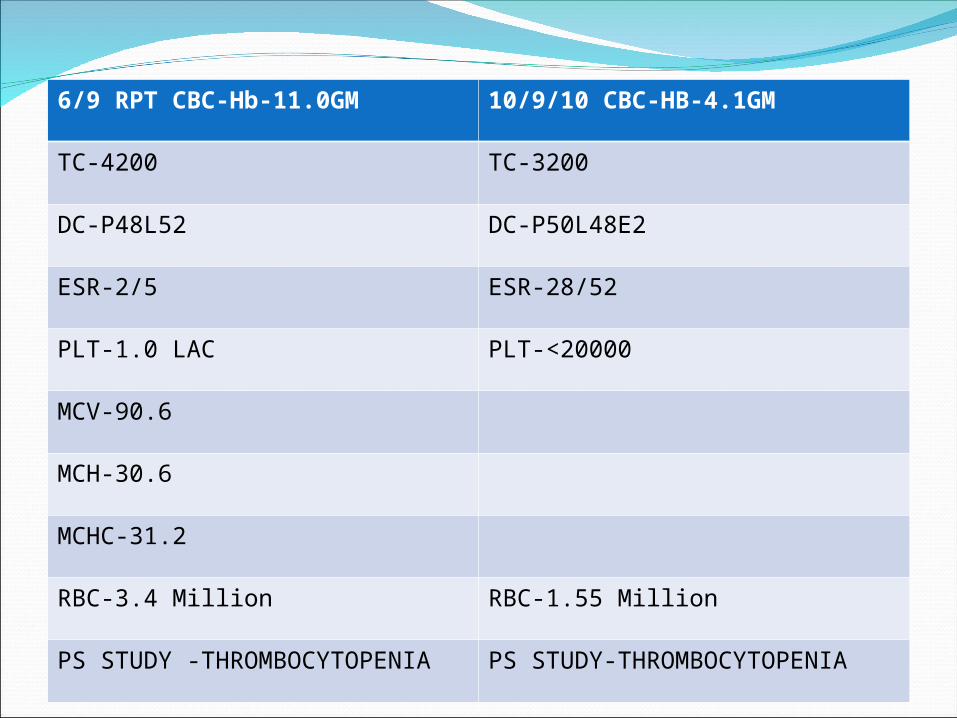
6/9 RPT CBC-Hb-11.0GM 10/9/10 CBC-HB-4.1GM
TC-4200 TC-3200
DC-P48L52 DC-P50L48E2
ESR-2/5 ESR-28/52
PLT-1.0 LAC PLT-<20000
MCV-90.6
MCH-30.6
MCHC-31.2
RBC-3.4 Million RBC-1.55 Million
PS STUDY -THROMBOCYTOPENIA
PS STUDY-THROMBOCYTOPENIA
PS study done outside:RBC-microcytic hypochromic
anisopoikilocytosis Many target cellsWBC-leukopenia+ ,no blast cellsPLT-reduced
USG abd-splenomegalyLFT-normalHIV-negativeSr.LDH-4011U/L
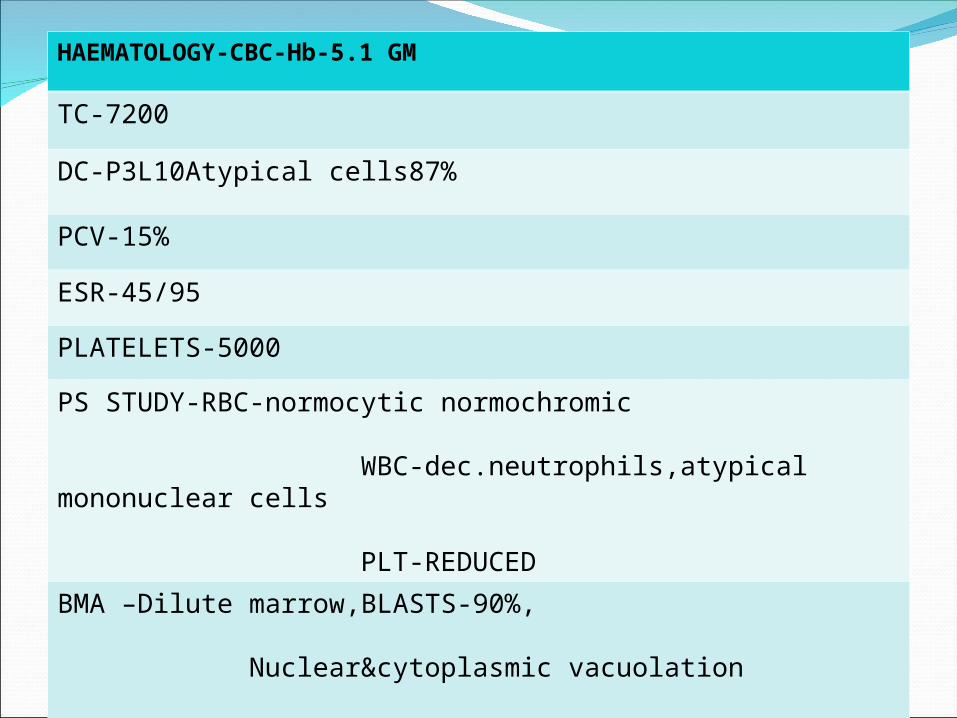
HAEMATOLOGY-CBC-Hb-5.1 GM
TC-7200
DC-P3L10Atypical cells87%
PCV-15%
ESR-45/95
PLATELETS-5000
PS STUDY-RBC-normocytic normochromic
WBC-dec.neutrophils,atypical mononuclear cells
PLT-REDUCED
BMA –Dilute marrow,BLASTS-90%,
Nuclear&cytoplasmic vacuolation
ACUTE LEUKEMIA-ALL –L3
DIAGNOSIS Acute lymphocytic leukemia-L3 with leukemic meningitis CNS 3;
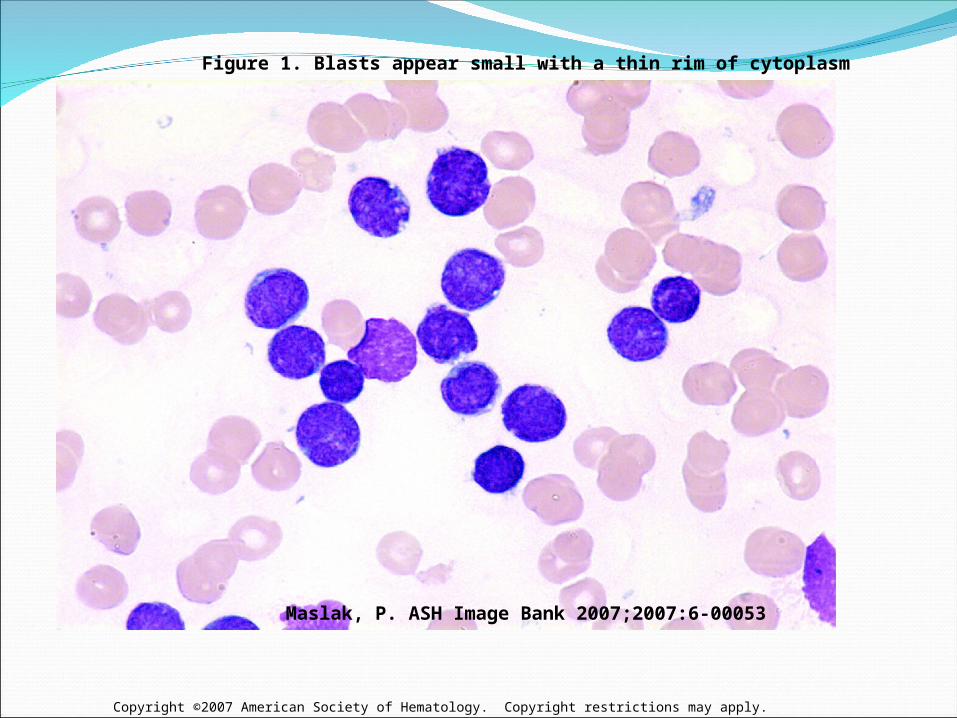
Copyright ©2007 American Society of Hematology. Copyright restrictions may apply.
Maslak, P. ASH Image Bank 2007;2007:6-00053
Figure 1. Blasts appear small with a thin rim of cytoplasm
Acute leukemia presenting with blasts first found in the cerebrospinal fluid but not in the peripheral blood
we report nine patients with acute leukemia, symptoms suggestive of involvement of multiple cranial nerves, the spinal cord, and meningeal involvement. Moreover, we found that all these patients unexpectedly showed the presence of blasts in the cerebrospinal fluid (CSF) but not in the peripheral blood despite repeated examinations. Bone marrow examination confirmed the presence of acute leukemia in these patients. .
Journal of Clinical NeuroscienceVolume 17, Issue 10, October 2010, Pages 1252-1255
Carcinomatous meningitis Occurs in 5 % of all primaries ;Most common –breast, lung ,prostate ,lymphoma and
leukemia ,melanoma ,git,
Mode of spread -1.hematogenous via choroid plexus
2.parenchymal blood vessels –
virchow robin space
3.microscopic vessel involvement
in arachnoid to subarachnoid space
Clinical features Symptoms Signs Headache ,nausea,
vomiting –increased ICT ;
Backpain due to radiculopathy;
Focal or generalised seizures
No fever Higher mental function - mild memory
loss-50% -dementia -30%
Multiple cranial nerve palsies
with asymmetrical limb weakness ( predilection for third nerve-75 % ) seventh – 47 % eighth -40 % second -38 %Papilledma -19 %60%-absent DTR –
polyradiculopathyhydrocepalus
InvestigationsCSF analysis: pressure >160 mm water protein >0.5 g/l glucose < 2.5 mmol /l (< 45 mg /dl) lymphocytes > 5 cells / c.mm CSF for malignant cells – first sample positivity rate 54 % repeat sample positivity 30 % negative -10% MRI BRAIN –T1 weighted images with
gadolinium enhancement will show meningeal enhancement -30 to 70%
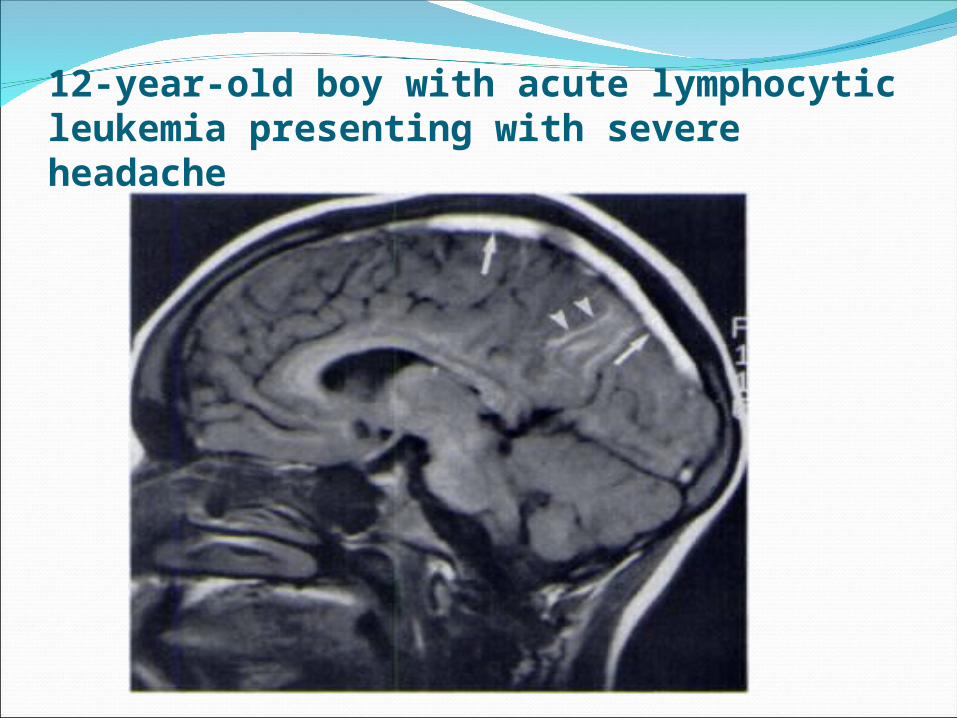
12-year-old boy with acute lymphocyticleukemia presenting with severe headache
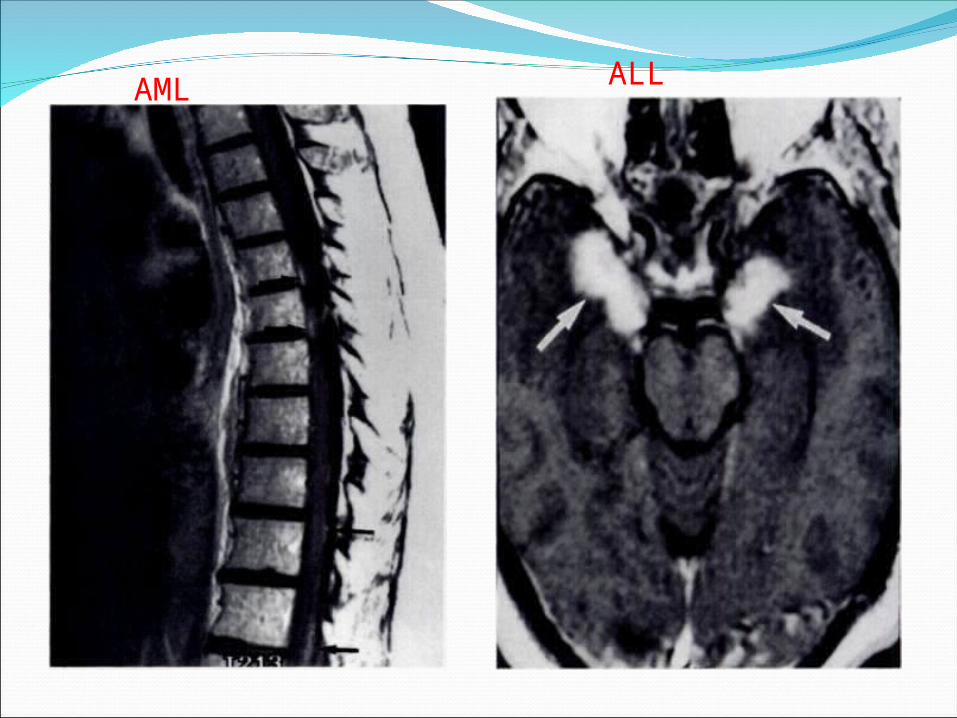
AML ALL
LEUKEMIC MENINGITIS 5 – 15 % of hematological malignancies ALL -40 % AML – 7 % lymphomas -7 -30 %Grading : CNS 1 –no WBC CNS 2 -<5 WBC /Blasts CNS 3 > 5 wbcs/Blast cells or presence of
multiple cranial palsies
Real time PCR analysis of CSF is an excellent
tool to assess occult CNS leukemia involvement
in patients with ALL and can possibly be used to
refine CNS status classification. (J Mol Diagn 2005,
7:127–132)
Survival UNTREATED ALL pts with CNS features -- 4-6
WEEKS
ON TREATMENT – 9 – 24 WEEKS
> 1 YEAR SURVIVAL
RATE – 10 %
.J Clin Oncol 21:184-188. © 2003
CNS2 patients have a good prognosis (EFS 80%) that does not require any intensification of CNS-directed therapy. TLP patients have an inferior prognosis compared with the CNS1 group (73% v 80%)
Treatment Dutch Childhood Oncology Group showed
that prophylactic cranial irradiation can be safely omitted from all children with ALL.202a
CNS disease at the time of leukemia relapse in adults occurs in approximately 10 percent of cases.
intrathecal methotrexate, cytarabine, and hydrocortisone. Systemic high-dose methotrexate and cytarabine add to the CNS therapy.
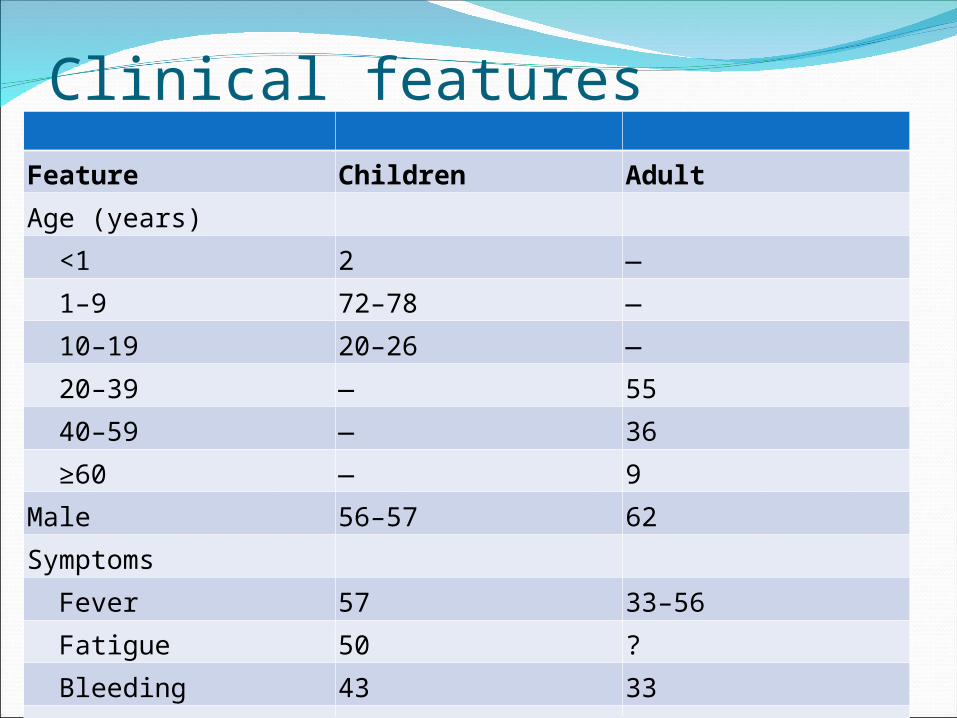
Clinical featuresFeature Children Adult
Age (years)
<1 2 —
1–9 72–78 —
10–19 20–26 —
20–39 — 55
40–59 — 36
≥60 — 9
Male 56–57 62
Symptoms
Fever 57 33–56
Fatigue 50 ?
Bleeding 43 33
Bone or joint pain 25 25
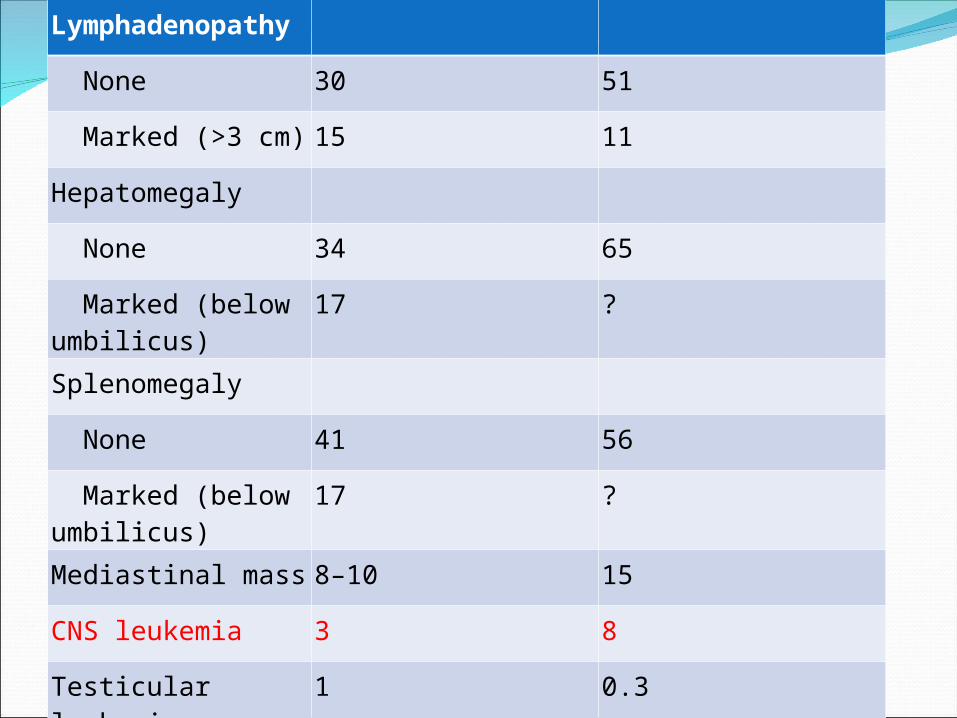
Lymphadenopathy
None 30 51
Marked (>3 cm) 15 11
Hepatomegaly
None 34 65
Marked (below umbilicus)
17 ?
Splenomegaly
None 41 56
Marked (below umbilicus)
17 ?
Mediastinal mass 8–10 15
CNS leukemia 3 8
Testicular leukemia 1 0.3
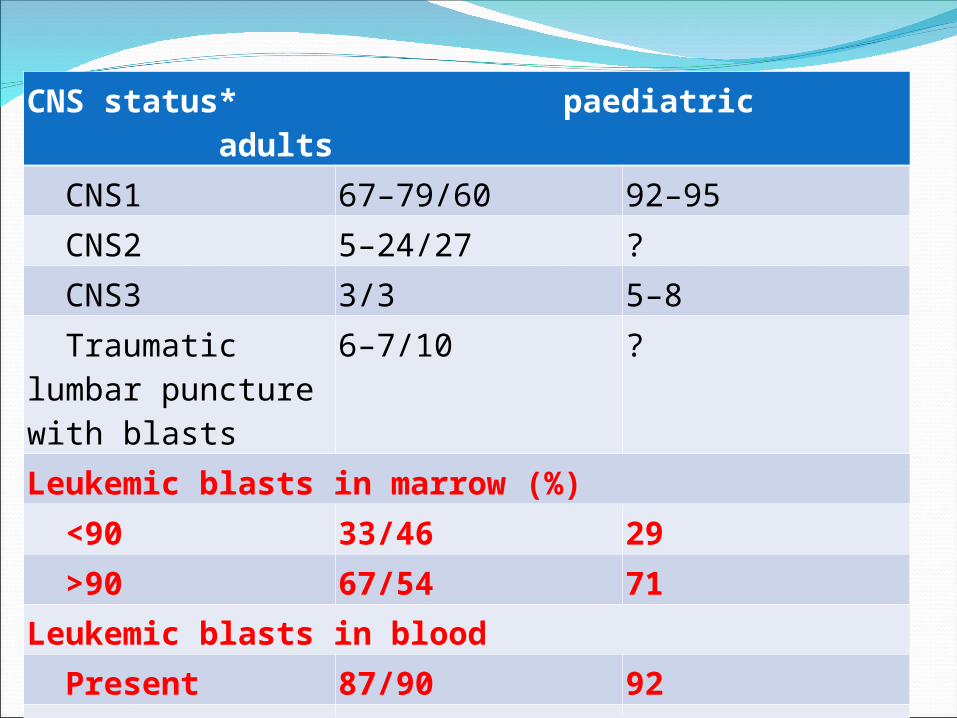
CNS status* paediatric adults
CNS1 67–79/60 92–95
CNS2 5–24/27 ?
CNS3 3/3 5–8
Traumatic lumbar puncture with blasts
6–7/10 ?
Leukemic blasts in marrow (%)
<90 33/46 29
>90 67/54 71
Leukemic blasts in blood
Present 87/90 92
Absent 13/10 8
Neurological manifestations of leukemia
Meningeal disease
1.Infiltration of the meninges by leukemic cells may affect the dura, the leptomeninges, or both and may be diffuse or focal.
2. presents as signs and symptoms of increased intracranial pressure, including headache, nausea and vomiting, irritability, lethargy, and papilledema [5]. Cranial nerve palsies may also be present.
3.Less common symptoms include myelopathy, auditory symptoms vertigo, ataxia, and hallucinations.
4. Diffuse dural infiltration by leukemia, far less common than leptomeningeal involvement
Nonmeningeal DiseaseIntracranial masses may occur in leukemia,
although they are rare. Chloromas (granulocytic sarcoma, myeloblastoma) are masses composed of immature granulocytic cells. These lesions were first described by Burns in 1811 and named for their greenish colon on gross inspection.
Granulocytic sarcoma occurs primarily in patients with acute myelogenous leukemia .
in leukemic patients include hemorrhage (intraaaxial or extraaxial),more in acute promyelocytic leukemia
sinovenous thrombosis, (cns infiltration,leucostasis&L-Asparginase therapy)
cerebral infarctions.CNS and other infections-
Aspergillus,Mucor,Cryptococcus&Listeria
Haematologic and cerebrovascular manifestations
Factors Responsible for Cerebral Infarction
AtherosclerosisNonbacterial thrombotic endocarditisIntravascular coagulationSinovenous occlusionTumor emboliSeptic emboliMiscellaneous (e.g. , compression of artery
by tumor, vasculitis)L-asparaginase therapy (leading to
sinovenous thrombosis
Pecularities of this case
Presenting initially as basal meningitisAsymmetetrical cranial nerve palsies with
polyradiculopathyDural enhancement on MRI in CNS ALL
which is rare.Absence of blast cells in peripheral blood.
Carry home message
Pt presenting with cortex involvement,multiple cranial nerve palsies and polyradiculopathy DD are
1.Tb meningitis when associated with fever2.if no fever suspect carcinomatous
meningitis.
References :American journal of radiology-165
SEPTEMBER-1995Brain ‘s neurologyAdam ‘s neurologyWilliam’s haematology-8th editionMRI IMAGING -SUTTON
THANK YOU





























