Embed Size (px)
Citation preview

CLEFT PALATE
Dr.Reza Parker (MD Romania)

Introduction
• Cleft lip and palate are the most common congenital craniofacial anomalies treated by plastic surgeons.
• Cleft care requires that the plastic surgeon be a member of a collaborative multidisciplinary team.
• Successful treatment of these children requires technical skill, in-depth knowledge of the abnormal anatomy, and appreciation of three-dimensional facial aesthetics.

Cleft lip, cleft palate, and the combinationof cleft lip and palate are considered to have a multifactorial cause, including both environmental and genetic elements.

Etiology
• Oral clefts have been linked to genes located on more than several chromosomes including 1, 2, 4, 6, and 19, among others
• maternal smoking (especially more than 20/day) and exposure to passive smoke
• Drugs: Accutane, phenytoin, warfarin ethanol • maternal folic acid deficiency• ingest large quantities of Vit A

EPIDEMIOLOGY • the most common diagnosis is cleft lip and palate 46%,• Isolated cleft palate at 33%• isolated cleft lip at 21%.• Majority of bilateral cleft lips (86%) and unilateral cleft lips
(68%) are associated with a cleft palate.• In the white population, cleft lip with or without cleft
palate occurs in approximately 1 in 1,000 live births.• twice as common in the Asian population• half as common in African Americans• More common in males
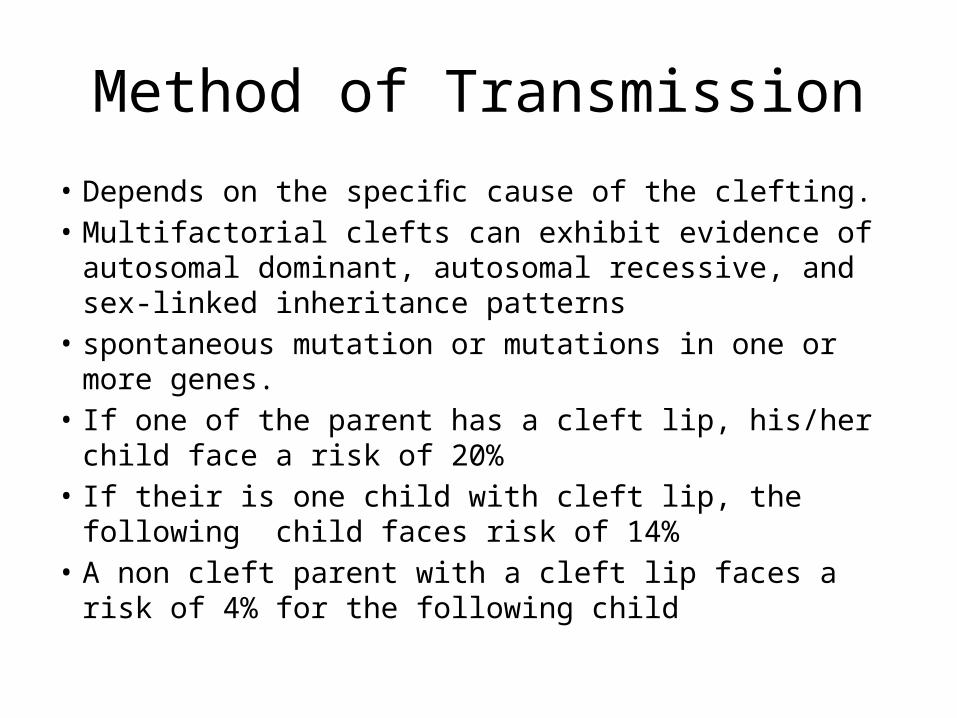
Method of Transmission• Depends on the specific cause of the clefting. • Multifactorial clefts can exhibit evidence of autosomal
dominant, autosomal recessive, and sex-linked inheritance patterns
• spontaneous mutation or mutations in one or more genes.• If one of the parent has a cleft lip, his/her child face a risk of
20%• If their is one child with cleft lip, the following child faces risk
of 14% • A non cleft parent with a cleft lip faces a risk of 4% for the
following child

Pathogenesis
• The face and facial structures are formed out of three plates, each migrating toward a meeting point in the middle area of the face.
• The facial structures of the orbicularis muscle form the lip. They are joined at the philitrum lines.
• join by 4th week of pregnancy

Pathogenesis
• The palate is then formed out of the structure that begins as the tongue and palate.
• Between the fourth and the eighth weeks of gestation, the tongue drops down and the palatal segments then move from the sides and toward the middle, fusing in the center.
• A cleft, therefore, is not something that is formed, so much as it is something that does not form.

Normal Process
• 6 Weeks– Maxillary process– Lateral nasal process– Median nasal process
• These three processes join and fuse to form the primary palate
• 7 Weeks– Median nasal process and maxillary process have fused
creating upper lip and anterior maxillary alveolus

Normal Process
• 8 Weeks– Complex totally fused and mesodermal migration
completed Tongue, which has been postured superiorly between lateral palatal shelves of maxilla, moves inferiorly allowing palatal processes to grow toward midline and fuse, form nasopalatine foramen to uvula
• 11wks– Total palatal closure

Classification
• The Veau Classification system • The Striped-Y Classification system

The Veau Classification system

The Striped-Y Classification system

Cleft Palate

Left-sided unilateral complete cleft lip and palate

Bilateral-right incomplete, left complete cleft lip and primary palate

Bilateral cleft of lip & palate

cleft of the hard & soft palates

Unilateral cleft of lip
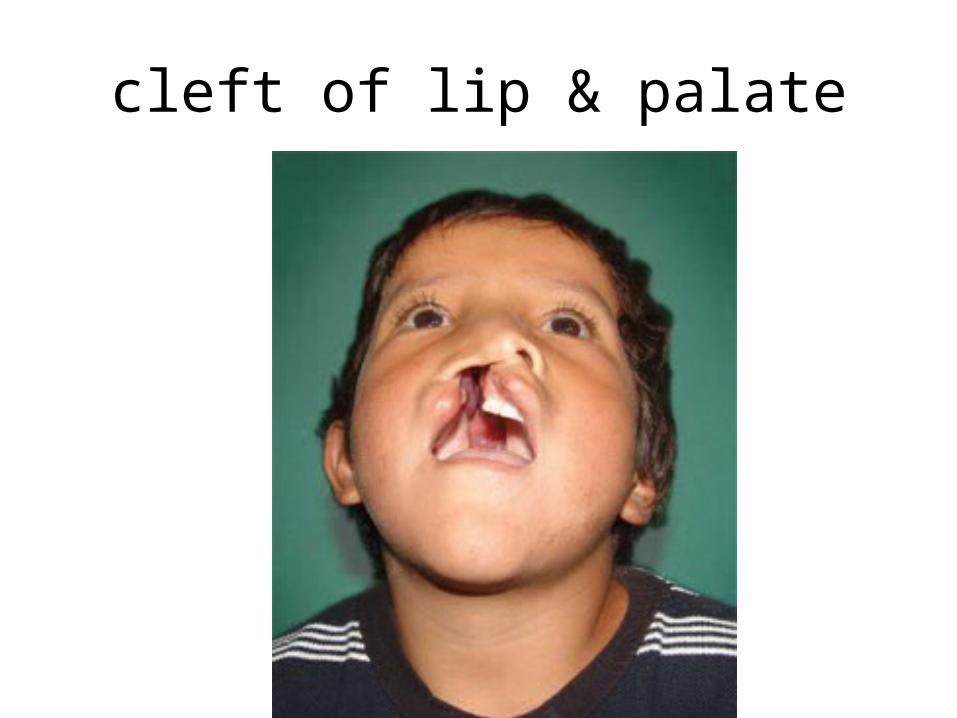
cleft of lip & palate

Bifid uvula

Prenatal Diagnosis
• Cleft lip can be easily diagnosed by performing ultrasonography in the second trimester
• Diagnosing a cleft palate with ultrasonography is very difficult
• Three-dimensional imaging has been introduced to prenatal ultrasonography diagnostics of cleft anomalies

Diagnosis• Advantages of Prenatal
Diagnosis:1. Time for parental education2. Time for parental psychological
preparation3. Opportunity to investigate other
associated anomalies4. Gives parents the choice of
continuing the pregnancy5. Opportunity for fetal surgery

Problems Associated With Cleft Lip and Palate
– Feeding–Dental problems–Nasal Deformity and Esthetic Problems– Ear Problems– Speech Difficulties–Associated Anomalies

Feeding Difficulties
• Cleft lip= makes it more difficult for an infant to suck on a nipple
• Cleft Palate= may cause formula or breast milk to be accidently taken up into the nasal cavity
• Inability to create negative pressure inside oral cavity• Frequent regurgitations• Upper respiratory tract infections
Dental Problems• Local Dental Problems:
– Congenitally Missing teeth, Hypodontia, Hyperdontia, Oligodontia– Presence of natal and neonatal teeth– Anamalies of tooth morphology like microdontia, macrodontia etc– Fused teeth– Enamel Hypoplasia– Poor periodontal support, early loss of teeth– Gemination, Dilacerations
• Orthodontics Problems:– Class III tendency– Anterior and Posterior Cross bite– Spacing and crowding

Nasal Deformity and Esthetic Problems• Facial Disfigurements• Poor nasal shape• Scar marks of surgeries• Poor lip function during speech• Poor dental alignment and smile

Ear Problems
• Middle ear disease - 22% to 88% • Conductive hearing loss and chronic suppurative otitis media
may result • Repeated tympanostomy tube placement

Why do cleft kids have eustachian tube dysfunction?
• Abnormal curvature of the eustachian tube lumen
• Cephalometric data - width and angulation of the skull base with respect to the eustachian tube are different
• Abnormal insertions of the tensor and levator veli palatini muscles into the cartilages and skull base
• Palatal muscle dysfunction

Speech Problems:
• Hearing loss hampers proper development of speech• Velopharyngeal Insufficiency (VPI)• Abnormal air• Poor pronunciation of – Bilabial, – Labiodental, – Linguoalveolar sounds

Schedule of TreatmentBirth:
Initial AssessmentPre-surgical assessment
3 Month:Primary Lip repair
9-18 month:Palate Repair
2 Year: Speech assessment
3-5 Year: Lip Revision Surgery
8-9 Year: Initial interventional
OrthodonticsPreparation for alveolar bone
grafting
10 Year:Alveolar Bone Grafts
12-14 Year:Definite Orthodontics
16 Year:Nasal Revision Surgery
17-20 Year:Orthognathic Surgery

Feeding• Cleft lip = makes it more difficult for an infant to suck
on a nipple– use special nipples to allow the baby to latch
properly (either pump or use formula)
• Cleft Palate = may cause formula or breast milk to be accidentally taken up into the nasal cavity– don’t feed baby without palatal obturator
(prosthetic palate)– feed in an upright position to keep milk from
coming out of the nose


Presurgical Orthopeadics:1. Reduces the size of cleft; Aids in Surgery2. Partial obturation aids in feeding3. Parental Reassurance at a crucial time
• Maxillary Strapping• Nasoalveolar Moulding Appliances (NAM)

Require orthopedic repositioning of the nasal cartilages, columella, nasal tip, and lateral wall of the vestibule
Presurgical infant nasal remodelling nasal molding
Nasal molding by post surgical nasal stenting
Facial taping 2 to 3 months

BILATERAL CLEFT LIPThe most challenging condition1. The premaxilla is extremely
protrusive
2. The premaxilla and prolabium can be of variable size
3. The columella is deficient/almost nonexistent
4. The palatal shelves are collapsed

• Protrusive maxilla imperative to be repositioned
• Premaxillary orthopedics with inraoral aplliance
• Denture adhesive
• Elastic strap


• Latham Appliance

Rule of Ten Primary repair- repaired at approximately 10 weeks • The surgeon usually uses the “Rule of Ten”• The child weighs 10 pounds • The child has a hemoglobin of at least 10 grams • The child has a white count of no higher than 10,000 • The child is at least 10 weeks of age


Definitnion
• Vague term used to describe a number of different abnormalities in the shape of the foot
• Now it has come to be synonymous with the commonest congenital foot abnormality

FOREFOOT
MIDFOOT
HINDFOOT

DefinitionsPlanus: flatfoot
Cavus: highly arched foot
Varus: heel going towards the midlineValgus: heel going away from the midlineAdduction: forefoot going towards the midlineAbduction: forefoot going away From the midline

CLUB FOOT
Talipes: Talus = ankle Pes = footEquinus: (Latin = horse) Foot that is in a position of planter flexion at the ankle,
looks like that of the horse. Calcaneus: Full dorsiflexion at the ankle


CLINICAL FEATURES
• COMMON PRESENTATIONS– Detected at birth – Infancy and early child hood – Late childhood

Clinical Features
• Short Achilles tendon• High and small heel • No creases behind Heel• Abnormal crease in middle of the foot• Foot is smaller in unilateral affection• Callosities at abnormal pressure areas• Internal torsion of the leg• Calf muscles wasting• Deformities don’t prevent walking
CLINICAL FEATURES
• Seek a detailed family history of clubfoot or neuromuscular disorders, and perform a general examination to identify any other abnormalities.
• Similar deformities are seen with myelomeningocele and arthrogryposis. Therefore, always examine for these associated conditions.

CLINICAL FEATURES• DORSIFLEXION TEST : • PLUMBLINE TEST : tibial torsion
• child is made to sit on a table with both LL hanging from the edge.• Line drawn from the centre of the patella to the tibial tubercle
when extended down should cut the foot at 1st or 2nd intermetatarsal space normally.- PLUMBLINE
• In CTEV , with medial rotation of tibia it cuts through 4th or 5th space
• SCRATCH TEST – INFANTS – MEDIAL SCRACTH TEST : FOOT EVERTS - PERONEALS– LATERAL SCRACTH TEST: FOOT INVERTS - INVERTORS

INVESTIGATIONS• RADIOGRAPHY– AP VIEW :angle formed b/w
• talus and calcaneum ( NORMAL 30-35) REDUCED• Talus and metatarsals ( NORMAL 5 -15 ) -VE
Helps to asses angle of varus and forefoot adduction

RADIOGRAPHY– LATERAL VIEW - ANGLE FORMED B/W • TIBIA AND CALCANEUM ( NORMAL 5- 15 ) -VE• TALUS AND CALCANEUM ( NORMAL 20- 50)
TO KNOW THE EXTENT OF EQINUS AND VARUS DEFORMITY
• CT , MRI , ARTHROGRAPHY

MANAGEMENT
The goal of treatment for clubfoot is to obtain a plantigrade foot that is functional, painless, and
stable
A cosmetically pleasing appearance is also an important goal
• CONSERVATIVE• SURGICAL• EXTERNAL FIXATORS
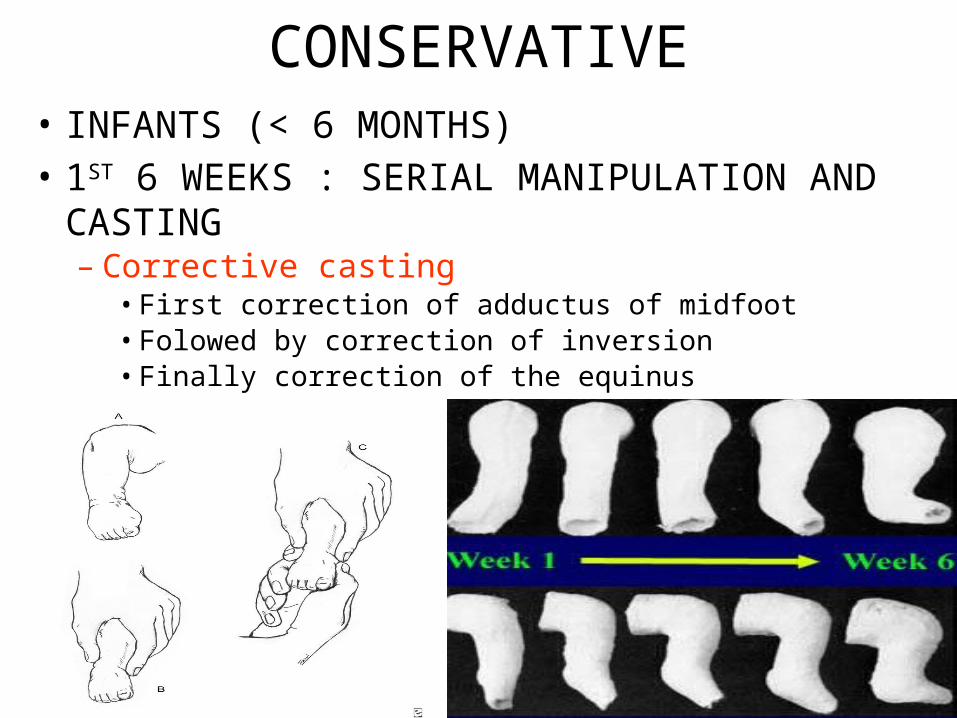
CONSERVATIVE• INFANTS (< 6 MONTHS) • 1ST 6 WEEKS : SERIAL MANIPULATION AND CASTING– Corrective casting
• First correction of adductus of midfoot • Folowed by correction of inversion• Finally correction of the equinus
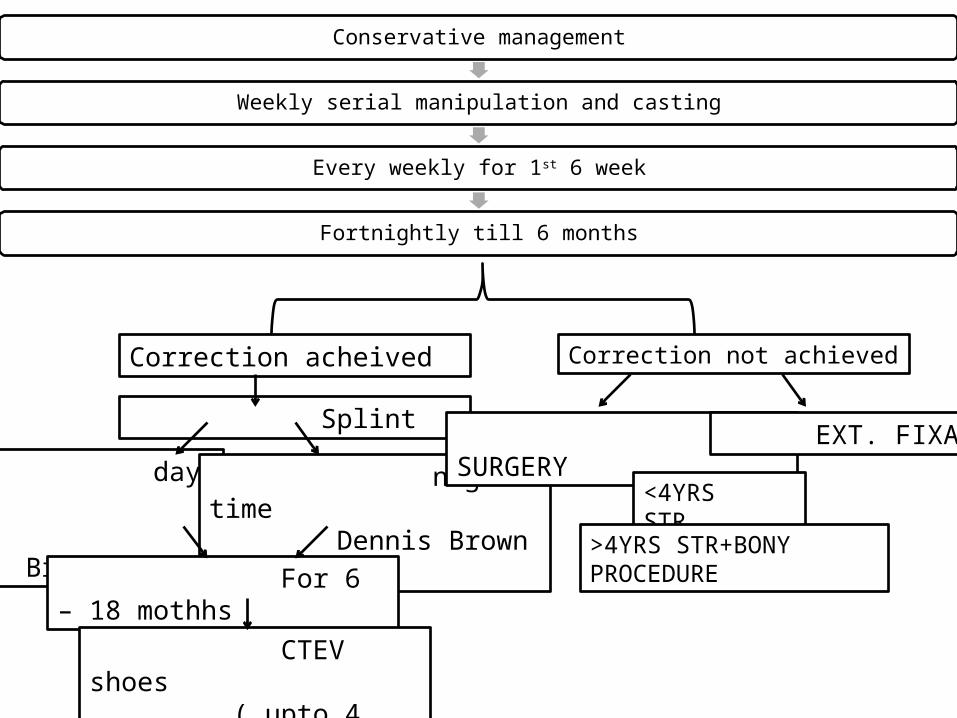
Conservative management
Weekly serial manipulation and casting
Every weekly for 1st 6 week
Fortnightly till 6 months
Correction acheived Correction not achieved
Splint
day time Phelp’s Brace
night time Dennis Brown Splint
For 6 – 18 mothhs
CTEV shoes ( upto 4 years )
SURGERY EXT. FIXATOR
<4YRS STR
>4YRS STR+BONY PROCEDURE

Surgical TratamentIndications• Late presentation, after 6 months of age • Complementary to conservative treatment• Failure of conservative treatment• Residual deformities after conservative treatment• Recurrence after conservative treatment

SURGICAL TREATMENT• Soft tissue operations– Release of contractures– Tendon elongation– Tendon transfer– Restoration of normal bony relationship
• Bony operationsUsually accompanied with soft tissue operation
Types:– - Osteotomy, to correct foot deformity or int. tibial torsion– - Wedge excision– - Arthrodesis (usually after bone maturity)– one or several joints– - Salvage operation to restore shape

EXTERNAL FIXATORS
• ILIZAROV’S EXTERNAL FIXATOR FRAME• JOSHI’S EXTERNAL FIXATOR FRAME• Allows gradual distraction
• Transfixing wires through– Tibia, calcaneum ad metatarsals
• Distractors positioned– Posteriorly, medially and laterally
• Frame completed by interconnecting the components

RETENSION OF CTEV CORRECTION
• DENIS BROWN SPLINT• PHELP’S BRACE• BELOW KNEE WALKING CALIPERS• CTEV SHOES