Embed Size (px)
Citation preview
CEPHALOMETRICS
Cephalometrics Definition
‘cephalo’ means head and ‘metric’ means measurement.
Measurement of the shadows of the bony and soft tissue landmark on the radiographic image is known as roentgenographic cephalometry
Types of cephalograms
Lateral cephalogram
Frontal or anteroposterior cephalogram
Oblique cephalogram
Uses of cephalograms orthodontic diagnosis to elucidate the skeletal, dental
and soft tissue relationships of the craniofacial region.
identification and classification of skeletal and dental anomalies.
estimating the facial type.
quantify the changes brought about by the treatment.
Uses of cephalograms distinguish changes produced by natural growth and
orthodonthic treatment.
Assessment of growth of facial skeleton through serial cephalograms.
growth prediction.
plan the skeletal repositioning in surgical orthodonthics
Advantages of cephalogramsFunctional analysis.
tangible records that are relatively permanent
relatively non-destructive and non-invasive producing a high yield of information at relatively low physiologic cost.
easy to store, transport and reproduce.
Limitation and drawbacks Patient is exposed to ionizing radiation which is harmful.
The processes of image acquisition as well as measurement procedures are not well standardized.
The difficulty in locating landmarks and surfaces on the X-ray image as the image lacks hard edges and defined outlines.
The structures being imaged are three dimensional whereas the radiographic image is two dimensional.

Limitation and drawbacks Anatomical structures lying at different planes within the head undergo
projective displacement.
Patient is positioned with the ear rods in the external acoustic meatus. The operator assumes that the meatuses are symmetrical. It need not be so.
Patient is made to bite in maximum intercuspation while taking the cephalogram. There could be a mandibular shift from centric relation.
A cephalometric analysis makes us of means obtained from different population samples. They have only limited relevance when applied to individual patient.
Cephalometric landmarks
Cephalometric landmarks can be broadly classified into
hard tissue soft tissue pointsBilateral points
Hard tissue pointsUnilateral points
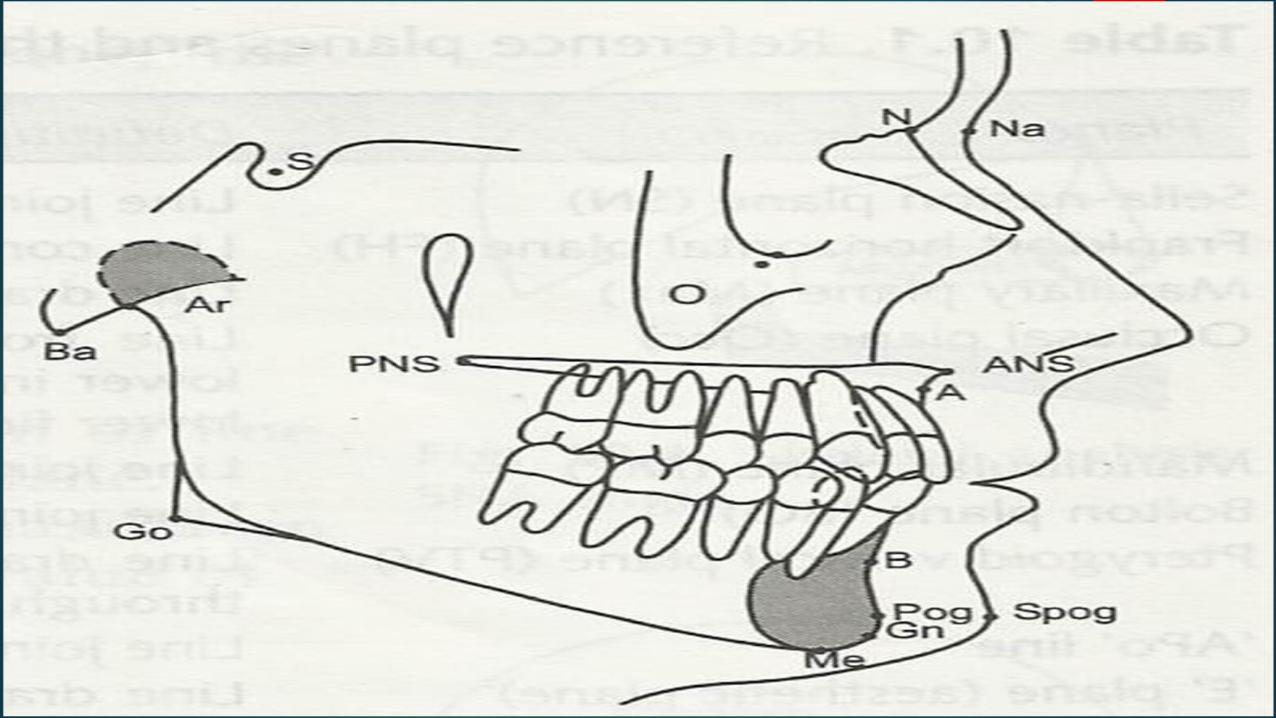
Nasion (N) : point where frontonasal and internasal sutures meet in the midline.
Anterior nasal spine (ANS) : Most anterior point of maxilla. Used for vertical measurement.
Point A (Subspinale): the deepest point in the curvature between anterior nasal spine (ANS) and inferior most point in the maxillary alveolar process.
Point B (Supramentale): the deepest point in the curvature between pogonion and superior most point in the mandibular alveolar process.
Hard tissue pointsUnilateral points
Pogonion (Pog): Anterior most point in the contour of the lateral shadow of the chin.
Gnathion (Gn): The most anterior and inferior point on the lateral shadow of chin. It is approximately in the midpoint between pogonion and menton.
Menyon (Me): The inferior most point in the contour of the chin.
Basion (Ba): The most posterior and inferior point in the sagittal plane on the anterior rim of foramen magnum.
Sella (S): Centre of the pituitary fossa or sella turcica.
Hard tissue pointsBilateral points
Orbitale (O): The lowest point on the outline of the bony orbit. In the lateral cephalogram, overlapping of the two side is seen. In that situation, lowest point in the averaged outline is used for constructing this point
Gonion (Go): The most posterior and inferior point at the angle of mandible.
Articulare (Ar): Intersection of the inferior surface of the cranial base and the posterior surfaces of the necks of the condyles of mandible.
Porion (Po): Superior most point of the external auditory meatus. Usually only anatomic porion is taken into consideration. The machine porion which is the shadow of the car rods are not considered.
Soft tissue points
• Soft tissue glabella (G’): The most prominent point in the midline of the forehead.
• Soft tissue nasion (Na’): Root of the nose in the midline.
• Soft tissue pogonion (S Pog): Most prominent point in the soft tissue contour of chin.
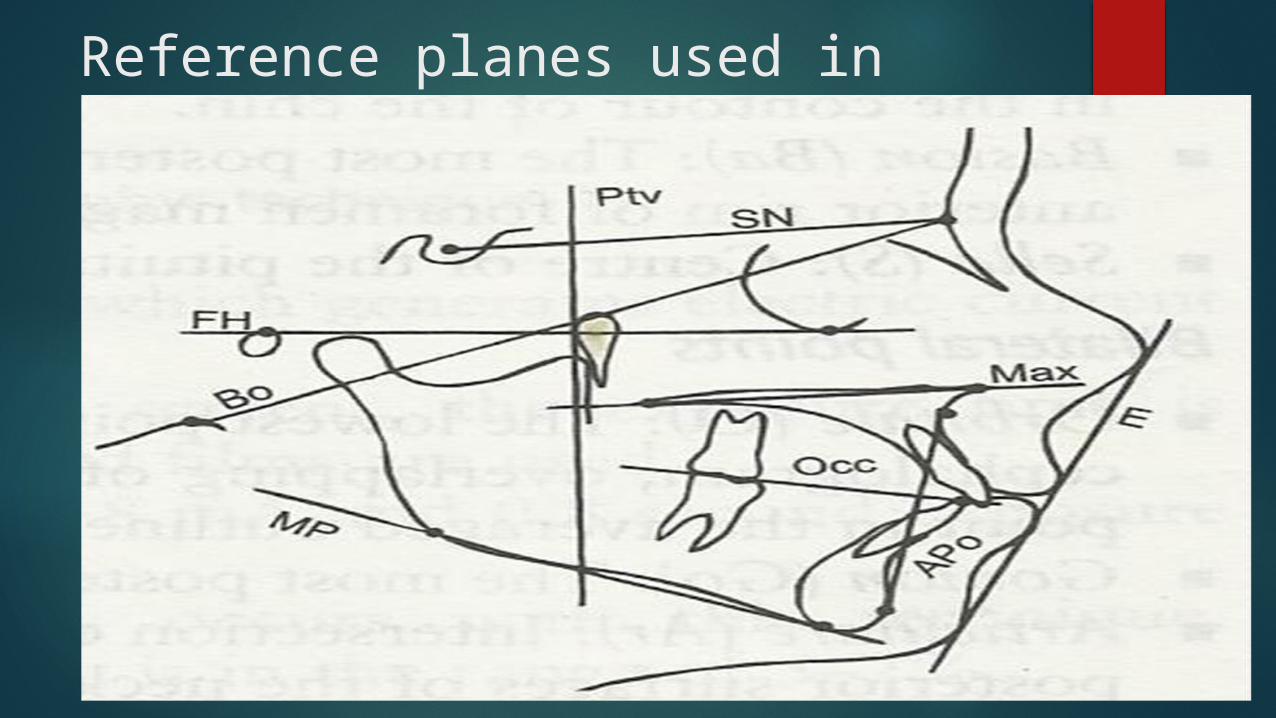
Reference planes used in cephalometry
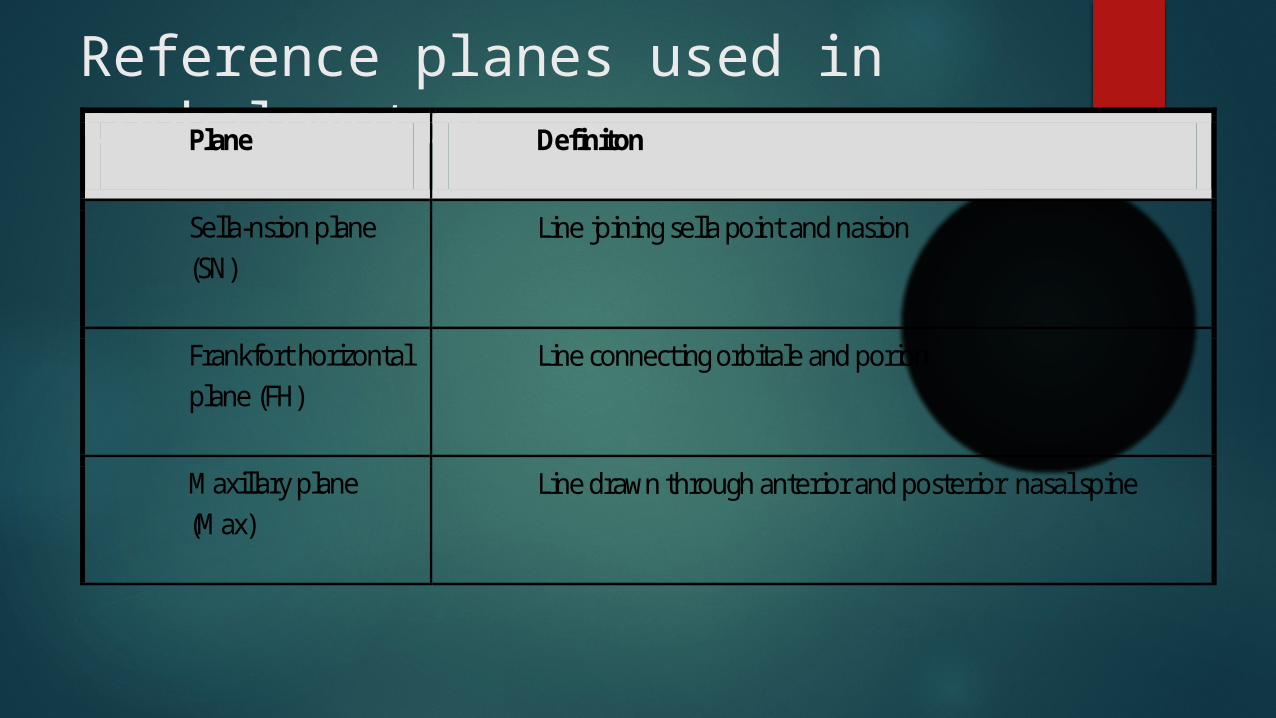
Reference planes used in cephalometryPlane Definiton
Sella-nsion plane (SN)
Line joining sella point and nasion
Frankfort horizontal plane (FH)
Line connecting orbitale and porion
Maxillary plane (Max)
Line drawn through anterior and posterior nasal spine
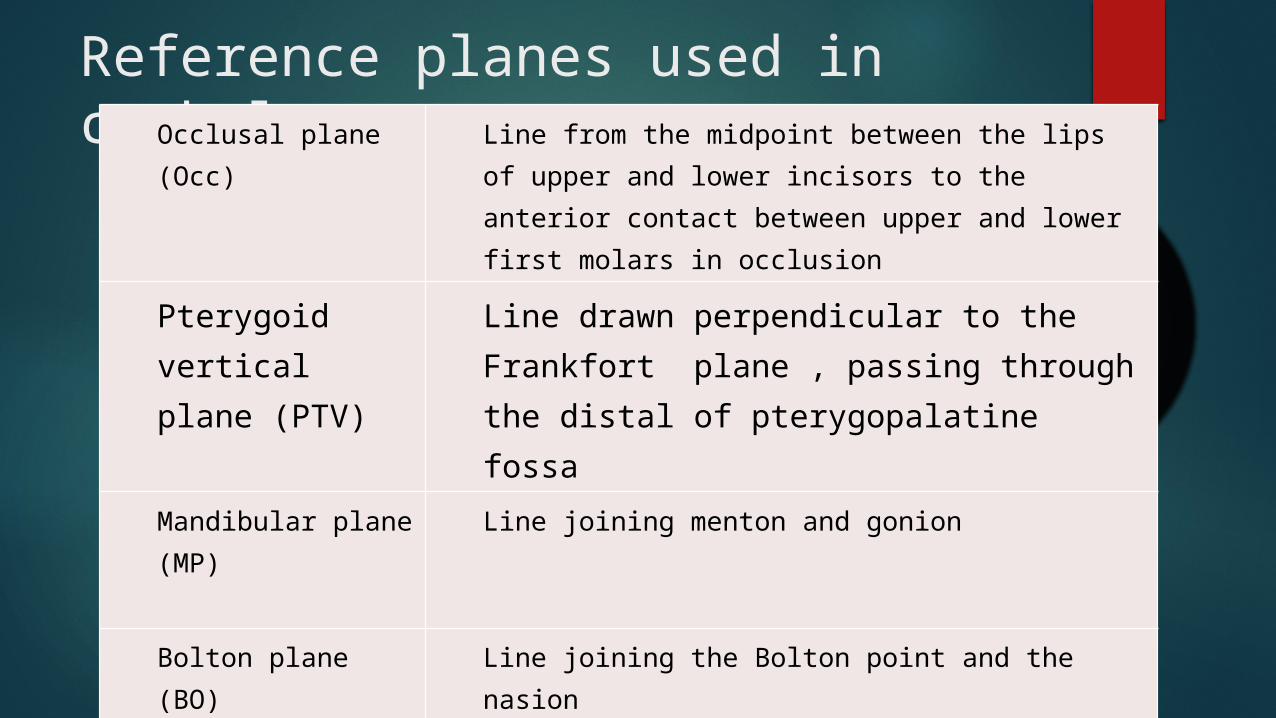
Reference planes used in cephalometryOcclusal plane (Occ)
Line from the midpoint between the lips of upper and lower incisors to the anterior contact between upper and lower first molars in occlusion
Pterygoid vertical plane (PTV)
Line drawn perpendicular to the Frankfort plane , passing through the distal of pterygopalatine fossa
Mandibular plane (MP)
Line joining menton and gonion
Bolton plane (BO) Line joining the Bolton point and the nasion

Reference planes used in cephalometry
‘APo’ line Line joining point A to the pogonion
‘E’ plane (aesthetic plane)
Line drawn from the tip of the nose to the most anterior part of the soft tisue chin.
Steiner’s analysis Steiner’s analysis provides maximum clinical information with
minimum number of measurements.
Steiner’s analysis consists of: Skeletal analysis Soft tissue analysis Dental analysis
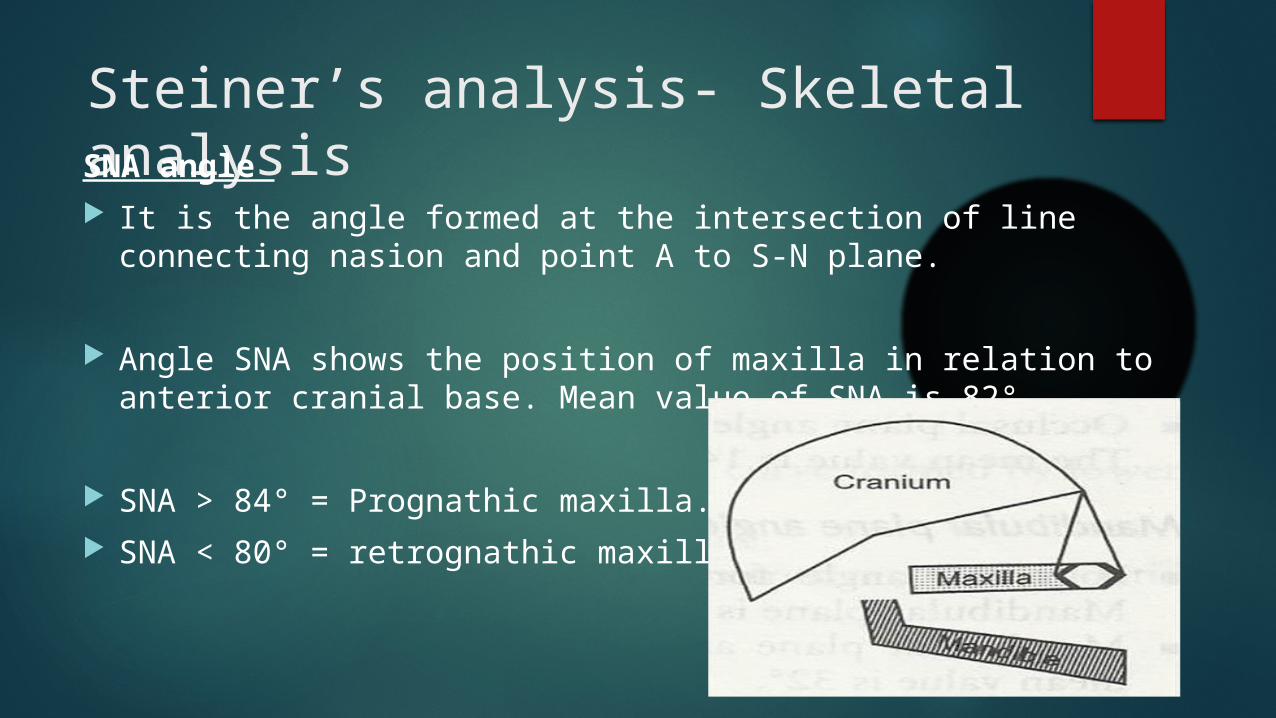
Steiner’s analysis- Skeletal analysisSNA angle It is the angle formed at the intersection of line connecting nasion
and point A to S-N plane.
Angle SNA shows the position of maxilla in relation to anterior cranial base. Mean value of SNA is 82° .
SNA > 84° = Prognathic maxilla. SNA < 80° = retrognathic maxilla
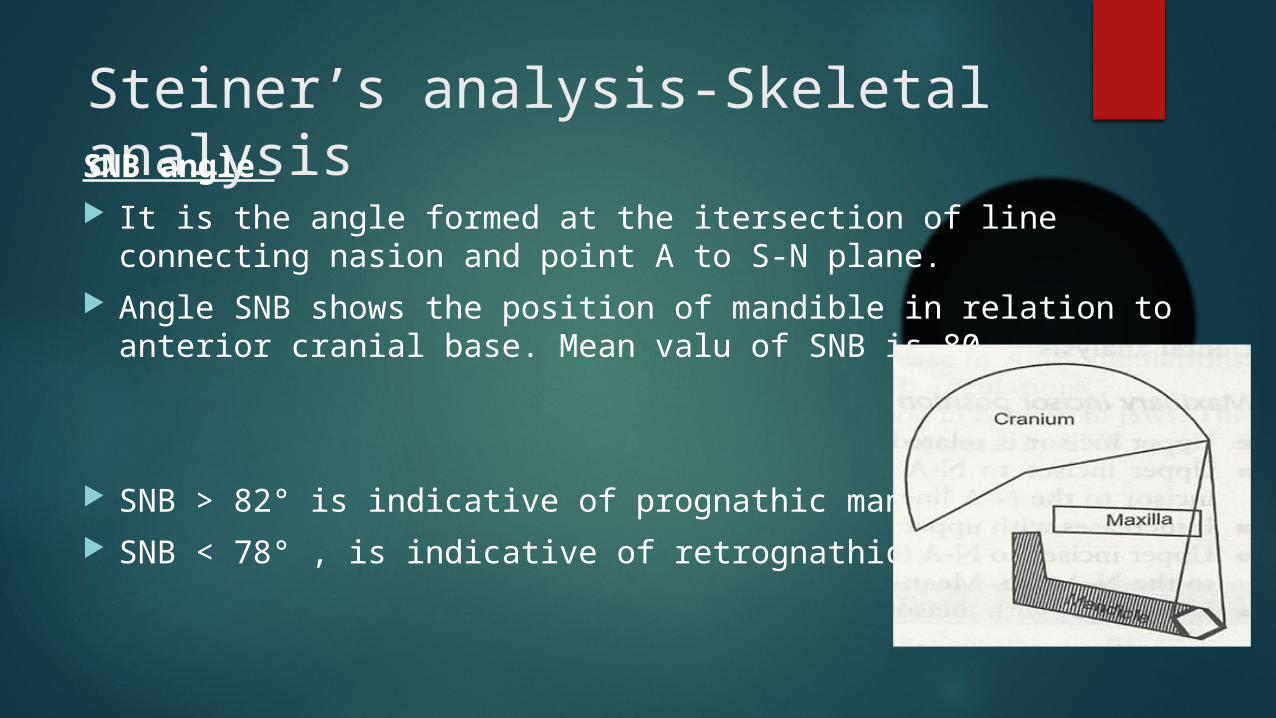
Steiner’s analysis-Skeletal analysisSNB angle It is the angle formed at the itersection of line connecting nasion and
point A to S-N plane. Angle SNB shows the position of mandible in relation to anterior
cranial base. Mean valu of SNB is 80.
SNB > 82° is indicative of prognathic mandible. SNB < 78° , is indicative of retrognathic mandible.
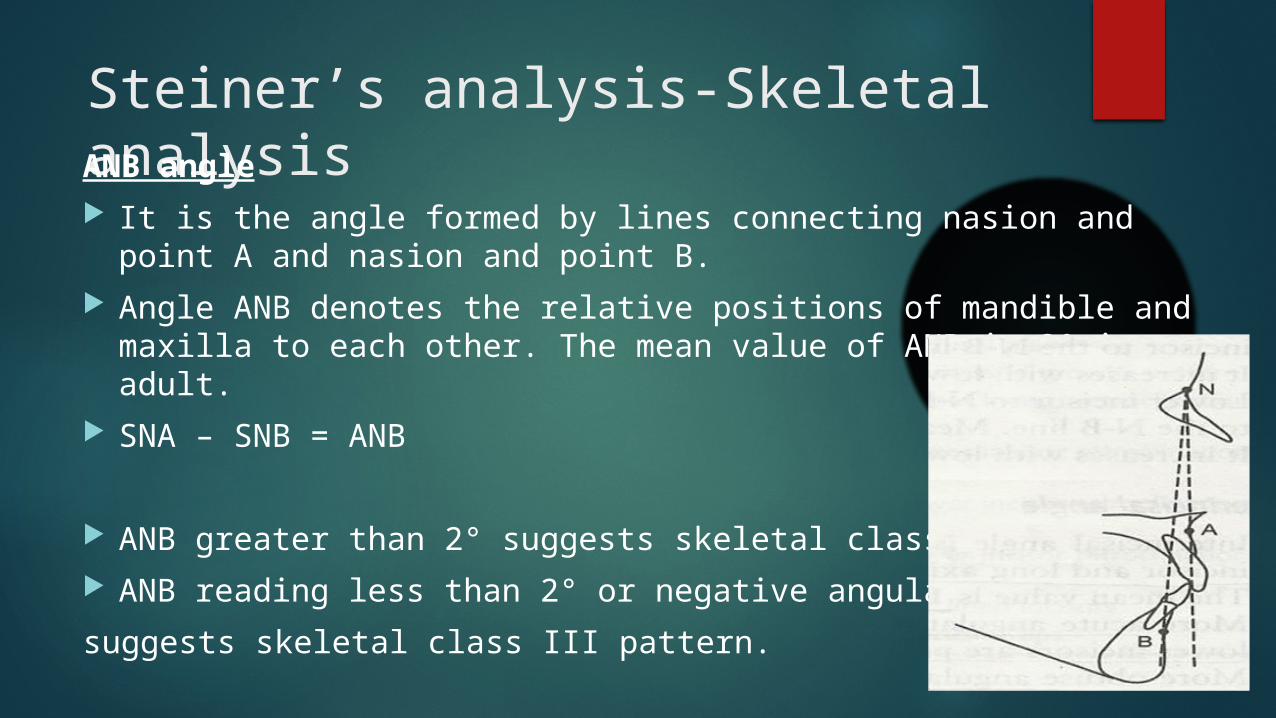
Steiner’s analysis-Skeletal analysisANB angle It is the angle formed by lines connecting nasion and point A and
nasion and point B. Angle ANB denotes the relative positions of mandible and maxilla to
each other. The mean value of ANB is 2° in an adult. SNA – SNB = ANB
ANB greater than 2° suggests skeletal class II patern. ANB reading less than 2° or negative angulations
suggests skeletal class III pattern.
Steiner’s analysis-Skeletal analysisMandibular plane angle
It is the angle formed by the S-N plane and the mandibular plane. Mandibular plane is drawn by a line connecting gonion and gnathion.
Mandibular plane angle denotes the growth pattern of an individual. The mean value is 32°.
High mandibular plane angle is indicative of vertical growth pattern and low mandibular plane angle is indicative of horizontal growth pattern.
Steiner’s analysis-Dental analysisMaxillary Incisor position Upper incisor is related to N-A line for determining its position.
Upper incisor to N-A (linear): the distance between incisal edge of upper incisor to the N-A line. Mean value is 4 mm.
It increases with upper incisor proclination and decreases with retroclination.
Upper incisor to N-A (angular): The angle between long axis of upper incisor to the N-A line. Mean value is 22°.
It increases with incisor proclination
Steiner’s analysis-Dental analysisMandibular incisor position Lower incisor is related to N-B line determining its position.
Lower incisor to N-B (liner): The distance between incisal edges of lower incisor to the N-B line. Mean value is 4mm.
It increases with lower incisor proclination and decreases with retroclination.
Lower incisor to N-B (angular): The angle between long axis of lower incisor to the N-B line. Mean value is 25º.
It increases with lower incisor proclination and decreases with retroclination.
Steiner’s analysis- Soft tissue analysis
Steiner’s line is drawn from the middle of S-shaped curve formed by lower border of nose to the soft tissue contour of the chin.
The lips in well balanced faces should lie along this line.
Lips located anterior to this line are labelled protrusive. Orthodontic treatment may be undertaken to reduce protrusion.
.
Tweed’s analysis / Tweed’s diagnostic triangle
Charles Tweed stated that there is a relation between the inclination of mandibular incisors and mandibular plane angle.
The mandibular incisor’s should be placed upright over basal bone for stability and aesthetics.
Tweed’s analysis
Cephalometric points used
• Porion: Superior most point of the external acoustic meatus.
• Orbitale : Inferior most point along the lower border of orbit.
Planes \ used
1. Frankfort horizontal plane: Obtained by joining porion and orbitale.
2. Long axis of lower incisor: Obtained by drawing a line along the long axis of incisors.
3. Mandibular plane: Obtained by drawing a tangent to lower border of mandible
Tweed’s analysis
Angles formed
1. Frankfort mandibular plan angle (FMA): the angle formed at the intersection of Frankfort horizontal plane and mandibular plane.
1. Value is 25º in well-balanced faces.
2. Incisor mandibular plane angle (IMPA): angle formed at the intersection of mandibular plane and long axis of lower incisor.
2. Value is 90º in well-balanced faces.
3. Frankfort mandibular incisor angle (FMIA): angle formed at the intersection of long axis of lower incisor and Frankfort horizontal plane.
Value is 65ºin well-balanced faces.
Tweed’s analysis
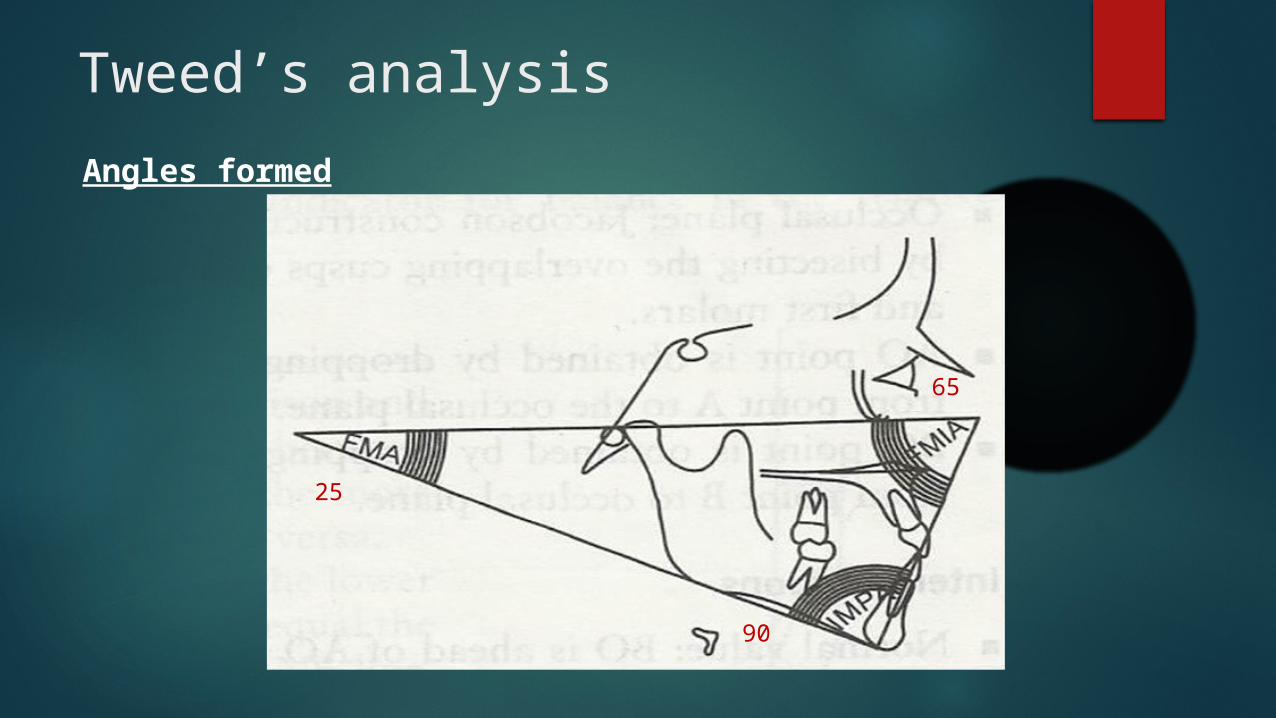
Angles formed
25
65
90
Tweed’s analysis
Interpretations
• FMA > 28º means high angle patient and mandible grows clockwise.
• FMA < 23º means low angle patient and mandible grows counterclockwise.
• IMPA > 110º means proclined lower incisors.
• IMPA < 85º means retroclined lower incisors.
Tweed’s analysis
Clinical applications
• diagnosis, classification, treatment planning and prognosis.
• Tweed advocated extraction of teeth to correct dveolodental prognathism and to position the lower incisors upright over basal bone.

Tweed’s analysis
Clinical applications
• FMA is in the range of 20º to 30º, the prognosis for orthodontic treatment with extractions is excellent to good.
• FMA angle is in the range of 30º to 35º, the prognosis for orthodontic treatment with extractions is good to fair.
• FMA angle is in range of 35º to 40º, the prognosis for orthodontic treatment with extractions is unfavourable.





























