Embed Size (px)
Citation preview

MULTTTOCAL MoTOR NtUuOpArHy (MMN)
Description . A progressing disorder affecting motor nerves, rcstrltirrl.l irr wr,,rhrr,..,..
. The disorder is autoimmune, and as such, often resp<tnds lo tnurrrrrrrmodulating therapy.
Pathophysiology . MMN is an autoimmune disorder, although the cause of the irrrnrrrrr,.attack is not known. Canglioside antibodies have been implicatctl rrr
some cases.
. Demyelinating changes predominate in the motor nerves, althouglrthere is some axonal drop-out. Conduction block is an importantdifferentiating feature of MMN.
Clinical findings . MMN presents with progressive weakness, often with cramping thalaffects peripheral nerve distributions in a patchy and asymmetricfashion, e.g., radial distribution producing wrist drop and peronealdistribution producing foot drop.
. Sensory symptoms are absent.
. Fasciculations can be seen along with the cramps.
. Re{lexes are normal or slightly reduced initially, but become absentwith progressive disease.
Laboratory studies . Routine labs are normal.
. CMI ganglioside antibodies are seen in about half of patients, and arrsupportive of the diagnosis but not required.
. lmaging is normal and often not needed.
. NCS and EMC show conduction block-where there is attenuation ofconduction of the motor nerves through selected nerve segments.Sensory conduction through the same regions is normal.Fasciculations may be seen, but denervation is not prominent.
Diagnosis MMN is suspected when a patient presents with progressiveasymmetric weakness without sensory abnormalities. ALS is usuallythe first thought in the clinician's mind, but exam does not showcorticospinal tract signs (hyperactive tendon reflexes and up-goingplantar responses), and NCS and EMG show conduction block ratherthan extensive denervation.
CMI antibodies are supportive of the diagnosis, but not diagnosticand not required for diagnosis.
Differentialdiagnosis
Amyotrophic loterol sclerosis. The main differential diagnosispresents with progressive asymmetric weakness, but there are signs ofcorticospinal tract dysfunction, and NCS and EMG show widespreaddenervation without significant conduction abnormalities.
Mononeuropothy multiplex. From many causes, can present withasymmetric weakness.
Management . lVlC is first-line therapy for most patients.
. Cyclophosphamide is used when patients cannot take lVlC or do notrespond.
. Corticosteroids are not effective and are not used.
Clinical course Patients can have substantial improvement with lVlC treatment, so it isimportant to differentiate this from ALS, which essentially is untreatable.
Mttlltlr)( (rl N4olot Ncut()l)(ll lty
tlrr
( ('rvr((rl l((l(lir rrloprrllty
lll)lloli
,l,llysiolt>8y
('r.l{vlcAt. I{AD!-CU!
Cervical nerve root damage can result in any combination or sensoryloss, pain, or motor loss confined to a single nerve root distribution.
Causes of cervical radiculopathy are multiple, and include:
Disc disease
Osteophyte formation
Tumor
lnfection
Diabetes
The common pathophysiology is nerve root impingement orinfiltration with resultant damage to the myelin and axons.
,rl findings Clinical findings depend on the level of the lesion. Most patientshave neck pain that radiates down the arm in the dermatomaldistribution. Weakness may be present, but is not invariable.
Rash over a portion of the involved dermatome suggests herpeszoster. This usually has a characteristic vesicular appearance.
lndividual nerve root symptoms and signs are as follows:
C5 rodiculopothy produces sensory deficit in the radial forearm.Motor loss is in the deltoid and biceps. Biceps reflex isdecreased.
C6 rodiculopothy produces sensory deficit in digits t and 2 ofthe hand. Motor deficit is in the biceps and brachioradialis.Biceps reflex often is decreased, and brachioradialis reflexes maybe as well.
C7 rodiculopothy produces sensory deficit on digits 3 and 4 ofthe hand. Motor deficit is in the wrist extensors and triceps.Triceps reflex may be depressed.
C8 rodiculopothy produces sensory deficit on digit 5 of the hand.Motor deficit is in the intrinsic hand muscles-both median andulnar innervated. Reflexes are normal.
rratory studies Routine labs are normal.
lmaging with MRI can show nerve root impingement orinflammation.
NCS is normal. EMC may show denervation in the distribution ofthe nerve root, but is not always present.
LP can be performed for neoplastic meningitis, but is of extremelylow yield in patients without known cancer.
lnosrs Cervical radiculopathy is suspected when a patient presents withpain and/or sensory loss in the arm with neck pain.
lmaging can show a structural cause in many patients. ln others,diabetes and herpes zoster have to be considered.
Zoster is supported by the development of the rash, which may beminimal and may occur days after the onset of symptoms.
Diabetic radiculoneuropathy is suggested by the diagnosis ofdiabetes and the absence of a structural cause seen on studies.
540 DISORDERS-NEUROMUSCULAR DISORDERS NEUROI\4USCULAR 54I

Differential diagnosis
Management
( t't'vit rtl l(trrlit rtlolrrrtlry tt,ru*t\t
CERVIC.AL RADICUTOT,ATHY.-<onI,d
Brachial plexopothy. Can produce motor and sensory [irrtlirrgs rrr
one or both arms. However, the symptoms span dermatonr,rldistribution.
Peripherol mononeuropothy Especially the radial nerve, periplrt'r,rlmononeuropathy can mimic cervical radiculopathy, e.9., C7 lesionHowever, examination of proximal and distal musculature helps todifferentiate a peripheral from a nerve root lesion. Also, mostperipheral nerve lesions span root distributions.
Nerve root compression from disc or bony element usually canusually be treated conservatively. Treatment options include:
Physicol therapy is extremely helpful for reducing pain andrestoring function. This should be offered to almost all patienls
Muscle reloxonfs are used if there is paraspinal muscle spasnrthat contributes to the pain.
Anti-inflommotory agents are given to most patients and canreduce pain.
Epidurol corticosteroid injections are considered if conservativt.measures are not helpful.
Surgicol decompression is considered especially if there isweakness or refractory pain.
Herpes zoster is treated with analgesics and antiviral medications.Anticonvulsants often are often used as an adjunct for control of tht,neuropathic pain.
Tumor infiltrotion is treated with local or neuraxis radiation.lntrathecal and systemic chemotherapy also often are given.Corticosteroids also are helpful for the pain of tumor infiltration.
Diobetic rodiculoneuropothy produces neuropathic pain, which canbe treated not only with analgesics but also by anticonvulsants suclras gabapentin. These agents are less helpful for the mechanical pairrthan the neuropathic pain.
Most patients improve with treatment, although not all. lf the cause ncompressive, there is a high remission rate with medications andtherapy, although there is the possibility of recurrence of the pain at ,r
later time.
542 DISORDERS-NEUROMUSCULAR DISORDERS-NEUROMUSCULAR 54I
( r,tvit rrl l{rrrli< trloprrllry
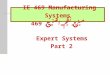
l)t.rrtt.rlorrrr.s art<l Myololncs of Uppcr Limb,,t,.',, lr.It,rtt, rlcrrr,rrr,rlrorr (,1 tl(,illl,tlr)[t(.\,,,,,rrlrrrri lo [r,r,r].rrr.ur(l (;,rt('ll) sltorln.ts distinctrlr ri,rrt,, I lrlt rs ,rr lrr,rill,r onsirk'r.rltle ovcrlaptr1r,r,rr ,rlj,rr cnl (l('ll.ll()ntcs. An alternativerr,rt()rr( nr,r1r is Ih,rl providcd by Foerster.
( .l lo I I Scnsory Representation Anterior view
Posterior view
au\
{, *t l-dfficz,-nl, -:]t *+*
t' \. -. ,tc4 '.l.t**-,r
C5
C5
IC8
.,'
i
C6\r;,-n qr-:-r'.'-
' ".-ca lr,-';: '
I Motor lmpairment Related to Level of Cervical Root Lesion
Hcrniated disccomprcssingnerve root

I ltotrtt it l(rt<lilttloprtllty
THORACIC RADICUT.OPATHY
Description Thoracic nerve root damage can result in pain, predornirr.rrrlly rrr llrr.chest.
Pathophysiology . All of the pathologies that can affect the cervical spine can alfcr I
the thoracic spine. ln general, disc disease and osteophyteformation are less common than they are in the cervical andlumbar spine.
. Herpes zoster and diabetic radiculoneuropathy are more imporl,rrcauses.
Clinical findings . Thoracic radiculopathy commonly produces unilateral chest wallpain, which begins near the spine and radiates toward the front,following the dermatome.
. Rash in the distribution suggests herpes zoster, especially whenvesicular.
. Motor deficit is not expected with thoracic radiculopathy.
. Reflex abnormalities are not expected, unless there are myelopatlfindings due to the cause of thoracic radiculopathy, e.g., disc ortumor with nerve and spinal cord compression.
Laboratory studies . Routine Iabs are normal.
. lmaging with MRI shows a structural cause in most patients. Wherimaging is normal, diabetes and herpes zoster have to beconsidered.
. NCS and EMC are of little value in diagnosis of thoracicradiculopathy and are not routinely performed.
Diagnosis Thoracic radiculopathy is suspected when a patient presents withsensory loss and/or pain in the chest. Careful exam confirms thedistribution of the symptoms within one nerve or dermatomedistribution.
MRI can show a structural lesion. lf this is normal, diabetes andherpes zoster have to be considered.
LP can be performed to look for neoplastic meningitis, but is ofextremely low yield in patients without known cancer.
Differential diagnosis . Lung disorders. Can produce pain that may be mistaken for thorarradiculopathy, especially pleural-based lesions, e.g., mesotheliomaand other tumors, infections, or inflammation.
. Cordiac poin. Rarely confused with thoracic radiculopathy.
Management Treatment of thoracic radiculopathy does not greatly differ fromtreatment of cervical radiculopathy.
Thoracic radiculopathy is not associated with perceptible motordeficit, and, therefore, pain is the main symptom to be addressed.
Clinical course Most patients improve with time, regardless of cause. Long-term useof agents for neuropathic pain occasionally is needed.
544 DISORDERS-NEURON/USCULAR DISORDERS-NEUROMUSCULAR 545
Iltotrtr it l(rrrlit trloprrllry
Spirr.rl Norvr' ()rigin: Cross Scction
'r'r liorr lhrorrth lhor.rcic vertebra
lt o| Ilrlr'lrr,r
I Lt,pt, ,me n inges
Fat in epirJur.r l sp.rcc:
Sympathotic 5;anglion
Ventral ro()1
Whito .rnd grav ranricotnrl u n ic;t ntt:s
Spinal nervt:
Ventral r.rmus(intorcost.rl nervei
Dorsal ranrus
Spinal sensory(dorsal root) ganglion
Dorsa I rool
I ;:lerr l horn ofgray m.rttcr oI spinal corcl
lnternal vertebral(epidural) venous plcxus

LUMBOSACRAL RADICULOPATHY
Description Damageto the lumbar or sacral nerves can producc s('nsory ()r nrrldeficit affecting the lower back, pelvis, and legs.
Pathophysiology The same causes of cervical radiculopathy can affect thelumbosacral nerve roots.
Disc disease and osteophyte formation are the most commonTumor and infection are less likely.
Clinical findings Lumbosacral radiculopathy causes pain in the back that can radi,rlr.down the hip and legs in a dermatomal distribution. Weakness c,rrrbe present, and of great localizing value.
Findings with individual nerve roots are as follows:
L2 rodiculopothy-sensory deficit on the lateral and anteriorupper thi8h. Motor deficit in the psoas and quadriceps. No rt'llabnormality.
L3 rodiculopothy-sensory deficit on the lower medial thigh.Motor deficit in the psoas and quadriceps. Knee reflex is
-
reduced.
L1 lodigulgpothy-sensory deficit on the medial lower leg. Morrdeficit in the tibialis anterior and quadriceps. Knee refleiisdecreased.
L5 rodiculopothy-sensory deficit on the lateral lower leg. Mot<rloss of the peroneus longus, tibialis anterior. No reflex -abnormality.
S.l rodiculopothy-sensory deficit on the lateral foot involvingdigits + and 5. Motor deficit involving the gastrocnemius. Anllereflex is decreased.
The unlisted roots-LI and S2-S4-can be involved, but much lesscommonly than the ones listed.
Laboratory studies . Routine labs are normal.
. MRI shows a structural cause in most patients. lf this is negative,diabetes, herpes zoster, and tumor are considered.
. CT of the lumbar spine is less sensitive than MRl, but has to beperformed when MRI cannot be done (e.g., pacemaker). lntratheccontrast dye improves the diagnostic sensitivity of the CT.
. NCS is normal. EMG may show denervation in the appropriatenerve root distribution if there has been significant involvement ofthe motor nerves.
. Lumbar puncture (LP) can be done to look for neoplasticmeningitis, especially with polyradiculopathy, but is of low yield inthe absence of known cancer.
l.tttttl rr ).\(t( I ( tl l(r rrlir rrlr )l )( rl lly
lr',
I rrrrrlrr)s(l( r(rl l{rtrlir ttlolrrrtlry
l.U M ROSACRAI. RADICULOPATHY--cont'd
Lumbosacral radiculopathy is suspected when a patient presentswith sensory and/or motor symptoms in the leg. The presence ofback pain is supportive, especially of structural causes.
MRI shows a structural lesion in most cases. lf this is normal,diabetes, herpes zoster, and tumor are considered.
A vesicular rash in a dermatomal distribution suggests herpeszoster.
Laboratory signs of diabetes support the diagnosis of diabeticradiculoneuropathy, although this does not mean that some othercause is not present.
NCS and EMG can support the diagnosis of radiculopathy if there is
Iocalized denervation.
t l,'rential diagnosis Lumbosocrol plexopothy. Can produce pain in the leg, which canalso involve the hip and back. Weakness is common. This disorderaffects muscles of more than one dermatome, however.Examination and EMG can make this distinction.
Peripherol mononeuropothy. Can mimic radiculopathy, e.g.,peroneal neuropathy and L5 radiculopathy can both produce footdrop without reflex changes. Differentiation is by examination andEMG.
Management of lumbosacral radiculopathy does not differ from thatof cervical radiculopathy.
Most patients improve. At least -l5o/o oI patients with lumbosacralradiculopathy improve with conservative care, although some willeventually still come to surgery.
546 DISORDERS-NEUROMUSCULAR DI\OIiI )I IIS NI IJI{OM(J\CUIAR '47

l.tt tttI rosrrr't rrI l{rtrlit trloIrtrI Iry,,\tt,,t,,t
l)ain l).tllcrns in Lurnlr.rr l)ist.ase
Radicular pain due to nerve root compression
Nervt,rootcomprcssed byenlarged iac:ct
Rad i cu lar
{ 1,.rin.p.rrterns(\rnBlL'seqmr.nt
dislributirin)
L-omprc,ssion oi specific nervc roo[results in p.lin scns.ttion in radicularpJlleilr .l)c( iii, trr di.lril,utiorr ilrthat particular ncrve ro()t
"f
r )r'.,( lll)lton
t,rtlrophysiology
rlrrrical findings
lltrtr ltirtl l'lcxr)lxrtlly
IIIIACHIAL PLEXOI'ATNY
Damage to the brachial plexus can produce pain, sensory loss, and/otweakness in one arm. Some plexopathies can be bilateral
\, ,,, ,
t*l'.iu#. \ ir',\,,\t
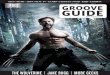
. The brachial plexus is formed from the individual cervical andupper thoracic nerve roots. The nerves diverge and reconnect toform the nerves of the arm. especially median, ulnar, radial, andmusculocutaneous. There also are other minor nerves supplyingshoulder muscles, and these are shown in the diagram.
. Causes of brachial plexopathy include: trauma, plexitis, tumolradiation, and bleeding.
Clinicat findings depend on the cause of the lesion and the preciselocation. Cenerally, there is pain and/or sensory loss in the arm.Weakness can develop in muscles innervated by the involved portionof the plexus.
Upper plexus /esions produce sensory andlor motor deficitsaffecting the distributions of the C5 and C6 nerve roots. Deltoidand biceps are especially affected, with sensory change thatextends below the elbow to the hand.
Lower plexus /esions produce sensory and/or motor deficitsaffecting especially the C8 and Tl nerve roots. Median andulnar-innervated muscles are affected, with hand weakness, andsensory symptoms involve much of the palmar hand, ulnaraspect of the dorsal hand.
Specific findings with individual causes include:
Troumo produces variable damage to the plexus. Stab woundscan affect almost any portion, but the upper plexus is moreexposed. Weakness is prominent early, soon followed byneuropathic pain. Upward traction of the shoulder can stretchthe lower plexus. Downward traction of the shoulder can stretchthe upper plexus.
Brochiol plexitis presents with pain in the shoulder and arm thateventually improves. During this phase, weakness develops,which has slower improvement. Upper plexus is mostly affected.
. Tumor can be compressive from the lung or infiltrating fromcervical lymph nodes. Tumor presents with severe pain, oftenweakness, and Horner's syndrome. Lower plexus is mainlyaffected.
Rodiotion theropy to the neck and chest produces dysesthesiasthat are uncomfortable, but not really painful. Weakness candevelop. The upper plexus is predominantly involved due tothinness of the tissues in the region of the upper plexus.
Bleeding into the neck and plexus from trauma and frombleeding disorder presents with weakness and motor loss in thearm, often with a palpable hematoma in the supraclaviculararea. Pain may be present, but is less prominent than withtumor or plexitis.
548 DISORDERS-NEUROMUSCI]I AR DISORDERS NEUROMUSCULAR'49

Itl(t( lll(tl I'lr,xollrtllty , t,nunuttt
BRACHIAL PLTXOPATHY*cont'd
Laboratory studies . Routine labs are normal. There are no reliable markcrs lor lrr.rr lrr,rlplexitis, although antinuclear antibodies (ANA) and ESR ottt'rr ,rrcchecked.
. MRI is able to show structural cause in a minority of patients,chiefly tumor or signs of trauma. Brachial plexitis and radiationplexopathy are not associated with reproducible findings on studit',,
. NCS usually is normal, although the sensory and motor actionpotential can become reduced in amplitude after t-2 weeks. EMGcan show signs of denervation after 3-4 weeks.
Diagnosis . Troumo as a cause for brachial plexopathy is evident from theinciting event. EMG can help to localize the lesion. lmaging may bcnormal with stretch/traction injuries but may show denervationhematoma and tissue disruption with penetrating trauma.
. Brochiol plexitis is suspected when a patient develops pain in anarm and no structural cause is identified. Subsequent developmentof weakness as the pain improves supports the diagnosis.
. Tumor infiltrotion is suspected with severe shoulder and arm painwith or without weakness. lmaging shows tumor compression orinfiltration in the region.
. Rodiotion plexopothy is suspected when a patient developsdysesthesias in the arm months after known radiation therapy.lmaging does not show a structural cause.
. Bleeding into the plexus can be seen on imaging and suspectedfrom exam.
Differential diagnosis . Cervicol rodiculopothy produces pain in the arm, but the lesionaffects only a single nerve root, unless there is polyradiculopathy.
, Mononeuropothy of the upper extremity can produce pain andweakness, but the deficit is distal to the plexus, which may beevident on exam or EMC.
Management . Tumor can be treated with surgery chemotherapy, andlor radiationtherapy. Surgery can make the plexus damage worser so this is lesscommonly used than radiation therapy and chemotherapy.
. Brachial plexitis often is treated with corticosteroids, although thishas not definitively been proven to be helpful.
. Management for the other causes is supportive.
Clinical course lmprovement depends on the cause of the plexopathy. ldiopathicplexitis commonly improves, with most having resolution of the painand eventual improvement in strength.
55O DISORDERS-NEUROMUSCI.]LAR DISORDERS-NEUROMUSCULAR 557
l!trrr ltirtl l'lcxollrtlltY
lh.rr hi,rl l'k'lrts: St ltt'trl.r
i l,,l, i 'rt.rl r,,rrtlr,rrtltott rltrrlr'tlI r, lrr, rl lrl.rrr', lr.r. l.rrtir'( I
, ,,nlrlrrllr)rr lrrrt l.rr k' I l.lir llrrlrl 1,1,'rrt. l,r< I(s ( 5 l)ullr l L', ottltilrttliott 31ruo\ \ 3".,,';.'i;1n,7, / r/r,":,:'
Suqrr,rrtaltul.tr \lirPhnni' /' / -lnerrc r( 1, 6\ \ncrv('\ / C5.
:i&.'
rpr\('l( ,, (), Y('r\('\ / C5.
\ll;:'l,tl::,\ \ \*2,\ ,.0*l \ \.y'. \
*i'dg" \.--\'*,
\ Y\\\l,,*,,,\
-lsl ril) \ \ lt,'l.nHust,'lli
s\a\ \ 6a,' \\ il'l:i,::''"
\ \ \ 1c5.6 7,rlr
\'rll,rr1 ,/r,,'rr r' (C5, {,) /ll.rrlr,rl trcrvt /r \, r.,7,1\,I1lt\lt'cli.rn netvt' ./c5, u,7,t,,I1t/
I'lrtrr nt,rvt, __--C7. 8,f 1t
-
lnconstanl contribution
r.t iritJiin-{roi i ",u"ncrvt'(C5, 6, 7)
pectoral ncrve (CU, l 1 )
Medial cutansrus nt'rve of .rrm (T1)
Meclial cutancous ncrve oi iorcarnr (C.8, T1 )
LJppcr sultscapular ncrvc (Ci5, 6)
Lower subscallular nerve (C5. 6)
Thora< odorsal (micldlc sullscapul'rri ncrvc (C6' 7' tl).a ; .,'
I atcral pet krral
^r$$\""'o''i ,

I rrrrrlrr )\(t( lltl l'lt'xoprrl lty
't:
lt.l
ul
dermatomal
ht,
riththe
Description
LUMBOSACRAL PTEXOPATIIY. -
Damage tothe lumbosacral plexus in the abdomen ((ur l)ro(hr((, l(.sensory and motor symptoms. The differential diagnosis is sirrul,rr trthat of brachial plexitis.
. Lumbosacral plexitis has similar causes to brachial plexitis; howr,vr.adiation plexopathy is uncommon, and idiopathic plexitis is lt:sslikely.
. Diabe.tic amyotrophy. is sometimes discussed under plexopathy, lrris really a polyradiculopathy
Pathophysiology
Clinical findings Lumbosacral plexopathy_is most commonly due to tumor. Bleeding,trauma, and idiopathic also are considered.
Clinical features of individual entities are as follows:
Tumor com.p.ression or infiltration of the lumbosacral plexuspresents with severe local and radiating pain into the leg.Patients typically have a known history oi renal orgastrointestinal cancer.
Troumo can produ.ce direct damage to the plexus, although inthis case, there is likely to be significant direct abdominaiorgu,damage. Pain in the abdomen and legs can be seen.
Lumbor plexitis is uncommon, and presents with hip and legpain, followed by weakness.
Bleeding into the plexus from femoral stick for angiography ortrauma produces a block of axonal transmission, r6su-lting indecreased sensation and often weakness that spans derriatomdistributions.
Laboratory studies . Routine labs are normal.
. MRI can show a structural lesion or layered blood, if present, in tl"paraspinal region.
. EMC can show denervation in a distribution appropriate to thedeficit; however, 3-4 weeks may elapse beforb'the EMC becomesabnormal, and a normal EMG does not rule out the diaenosis.
Diagnosis . Lumbosacral plexopathy is suspected when a patient presents witparn and/or weakness of one leg, often associated wiih pain in ttflank region or abdomen.
. lmaging can confirm a structural lesion. lf structural imaging isnormal, then tumor infiltration is Iess likely, but not rulei o"ut.
. EMG is initially normal, but subsequently becomes abnormal 3-4weeks later, and the distribution oi the findings can confirm thelocalization to the lumbosacral plexus.
Differential diagnosis . Lumbosocral rodiculopothy. Can present with weakness and/orsensory deficit.in one leg. The pain can radiate, suggestingradrculopathy, but the symptoms and signs are confined to onenerve root distribution.
. liob.elic omyotrophy. Presents with pain and subsequent weakneinvolving, mainly, the quadriceps. The clinical preseniation can beindistinguishable from lumbosacral plexitis.
552 DISORDERS-NEUROMUSCULAR
weakness
DISORDERS-NEUROMUSCULAR 555
Ltttttl rt)s(r( t(rl l'lcxoprtl lty
. Marr,rgr:rrrent of lumbosacral plexopathy is largely supportive unlesstreatable tumor is identified.
. Lumbosacral plexitis often is treated with corticosteroids, althoughthe benefits have not been proven.
. Hematoma eventually absorbs, resulting in return of the function ofthe plexus. Evacuation seldom is necessary.
Most patients improve, but the prognosis depends on the cause.ldiopathic plexitis results in significant improvement in most Patients.

l.tttttllrtstt< trtl l'lcxolrrrllty,,'tttt,t1t.1t
Lumbar l'lt'xtrs
Schema SuhcLrslal ncrvL' (T I 2 )
Whitc and gray rami communicantcs
lliohypogastric n"*" =- ... -'"-
..,
,.:,I I ioi n gu i na l nerv€r--------f; .,,
{
Clcnitofenroral ncrvc
Latcral cutanc-,ous
rt)
t1
L2
t3
nene,,f thish--___-_
Crav rami a()mmlrniaantes
Muscu la r bra nchcsto psoas and iliacus muscles
Aa c essory
Sacral and Coccygeal Plexuses
Schema
Vcnl ra I
rami oisp in,r I
nervos
Anterior division
Posterior division
umbosacral trunk
Anterior divisionPosterior division Cray rami communir ,rr,t,
inferior hypogastric
Superior gluteal nerve \\\
J::::H#:\
Nerve to quadratus femoris (and inferior gcn
Nerve to obturator internus (and superior
I54 DISORDERS-NEUROMUSCULAR DISORDERS-NEUROMUSCULAR 555
r lnosts
( r tltr rrl lllrrcss l'olyttctu()l)(rtlty
ill)lt{)n
r, rplrysiology
r, .rl f indings
lRtTrlAr. il.r.N[ss T oLYNEUROPATHY (CrP)
A common cause of weakness and failure to wean ICU patients fromtheir ventilator
The etiology of CIP likely is multifactorial. ICU care, critical illness,corticosteroid administration, and paralytic administration are all riskfactors, although they are not all necessary for CIP development.
Patients develop weakness with decreased tone after at least Iweek, and usually 2 weeks, of ICU care. There may be sensorysymptoms reported when the patients are questioned; however,pain is not a common feature.
The weakness often manifests as a failure to wean from theventilator.
rratory studies Routine labs are normal, or only show abnormalities associatedwith the underlying disease. Creatine Kinase (CK) often is measuredto look for myopathy, and is normal or only mildly increased.
lmaging is normal, and often not necessary when electrophysiologicstudies have demonstrated the neuropathy.
NCS and EMC show polyneuropathy with mainly axonal features;widespread denervation is seen.
CSF is normal or shows mildly elevated protein.
. CIP is suspected when a patient recovering in the ICU has slowweaning and is noted to have flaccid weakness, even in theabsence of sedatives and paralytics.
. Diagnosis is supported by lack of markedly elevated CK, axonalneuropathy identified on NCS and EMG, and absence of otheridentified abnormality from study.
rrential diagnosis Criticol illness myopothy. A closely related condition with some ofthe same features. This is difficult to distinguish from CIP withoutbiopsy. EMC can give some guidance, but may not be definitive,especially early in the disease process. Sensory examination in thisclinical setting is imperfect, and many patients have other medicalreasons to have polyneuropathy confounding the use of this as a
distinguishing feature.
Acute inflommotory demyelinoting polyneuropothy (Guillain-Borresyndrome). Presents with weakness, which can develop in an ICUsetting. This occasionally is missed when a patient with knowncongestive heart failure (CHF) or chronic obstructive pulmonarydisease (COPD) presents with weakness that is presumed to bedue to their medical illness, and the neuropathy is not noticed. NCS
and EMG show demyelinating changes, and CSF protein is elevated.
ragement Treatment is supportive. lf AIDP has been eliminated as a possibiliryimmune-modulating therapy is not of proven value.
Physical therapy and occupational therapy are of tremendous help.
Medical management includes minimizing corticosteroids andparalytics. This general approach may not only be helpful for thepatient but also for lowering the risk in other patients.
ical course . Patients make a dramatic recovery from ClP. Patients who arequadriplegic regain strength, and ultimately ambulation, with timeand care.
. About 50o/o have total recovery.

( Iiltr rtl lllrtr,ss l,olyttr,tttoprrllry ,,,ttt^t,,t
History
Vlolot Nr,urorr I )isr,rrst's
ovlRvlt:w of Mol'oR NEURoN DISEASES (MND)
. Motor neuron diseases produce weakness through degeneration ofthe upper and/or the lower motor neuron.
. They are pure motor disorders, without sensory symptoms or signs.
. Progressive weakness in the ICU
. Ask about sensory symptoms
. Ask about a history of DM, cancer, or other causes of neuropathy
. Ask about medications and other exposures that can cause neuropathy or myopathy(certain antibiotics, statins, alcohol)
,rnbined upper and\ruer motor neuron5ease
The upper motor neurons are those whose axons make up thecorticospinal and corticobulbar tracts. Their cell bodies liepredominately in primary and secondary motor cortices. Theydirectly activate lower motor neurons, which primarily lie in theanterior horn of the spinal cord gray matter and in brainstemmotor nuclei.
These disorders typically are painless and slowly progressive.Symptoms of weakness, spasticiry and increased deep tendonreflexes predominate.
. The lower motor neurons have their cell bodies in the anteriorhorns of the spinal cord and in the brainstem. They form the longmotor axons, which supply the muscles of the entire body.
. Lower motor neuron disorders cause weakness without spasticity,unless combined with upper motor neuron dysfunction. Decreasedtone and decreased reflexes are seen.
. Degeneration of both the upper and lower motor neurons isusually idiopathic. ALS is the principle.
. The upper motor neuron degeneration causes weakness especiallydistally with atrophy of the intrinsic muscles of the hands.
. The lower motor neuron degeneration causes spasticity of the legswith impaired coordination. There are no sensory deficits.
. The differential diagnosis consists of simultaneous unrelated uppermotor neuron damage (e.g. spondylosis) plus lower motor neurondamage (e.g. neuropathy).
. Motor exam - weakness may be proxlmal (myopatiry), Uistal lnerropa-hy1, o, botf,. Sensory exam - any sensory loss and distribution *-distal, proximal, or spinal level.. Rellex exam - absent DTRs suggests AlDp, ClDp, Clp; increased suggests spinal orcerebral cause
. Lab: CPK, aldotase, myoglobin, TFIs, Brz,
' Ncs & EMG: can differentiate neuropathy, myopat-hy, neuromuscular transmission defect' Muscle biopsy: confirmation of certain myopathies and supportive of some n"rroprt ,"". Nerve biopsy: confirmation of certain neuropalhies
. Weakness, latigue
. No sensory delicit
. Dx by NCS and lab
. Weakness and latigue
. No sensory deficit
. Dx by NCS and lab
Lambert-Eaton Myasthenicsyndrome. Weakness, fatigue
dry mouth. No sensory loss. Dx by NCS and tab
Myopathies
Critical illness myopathy. Weakness and decreased
tone. Dx by EMG and tab. Confirmed by biopsy
Rhabdomyolysis. Weakness often with
muscle pain. Dx by lab (including lCpK)
lnflammatory myopathy. Weakness 1 muscle pain. Dx by EMG and lab. Confirmed by muscle biopsy
Neuropathies
Critical illnesspolyneuropathy. Weakness, decreased tone. Loss of DTFIs. Dx by NCS, EMG, lab. Bx?
AIDP. Weakness, decreased tone. Often with pain. Loss of DTRs. Dx by NCS, lab, LP
CIDP
. Weakness, decreased tone
. Loss of DTRs
. Dx by NCS, lab
. May need nerve bx +/o Lp
556 DISORDERS-NEURON/USCULARDISORDERS NEUROA/USCULAR T57

Motol Nt'tttott I )ist'rtst's,,,,t,,r',t?
l't itttrrty Lrrlt,rrrl St lt'r'osis
| ,, .r
t rlrr
.tr,'fi:
.-r'(
Midbrairr
s 11)
{)
,'A
d
\"d.#Basispedunculi
pontrs
t1t_*
'{i:
t:j
Motor system
Fibers oriSiinate in motor cortex .rttr I
descend via posterior limb of inlorrr,,lr:apsule to basis pedunculi of mirllrr,rr',
Longitudinal bundlcs branch uponentering basis pontis ancl rejOin lO
cnter pyramids of medulla
At lowcr medulla, bulk of fibers t r,,'median planc to form lateralcorticospin.rl tract; somo [ibcrscontinue downward in the ipsilatcr,rLl,rlcr,rl ,,rtlir o\Pin,rl Ir.r( lj r)lher.rles, ending ip.ilaler,rl in lh(',rnlen,,r()rticospinal tract
Synapsc occurs at spinal Ievel: Lalcr,rlcorticospinal fibers synapsc onipsilateral anterior httrn cells; antt'ri,,rcorticospinal iibers synapse oncontralateral antcrior horn cells
- \ -, l,-'**d*...
Pyramids
t"q
tq
Ahove mid-thorar:ir:level
,;iJ:r::"'-
Belolv miclthoracic ..
lr:vel ..:
i*i*;*r"
)gement
Spi na I
corcl
i.,,
{,'Anterior c0rticospi nal tract
Lateral cortircspinal tract
tl
"tlt"#}
|ll)lron
r1rltysiology
,rl findings
pRIMAnY $rERAr Scrrn0$rl
x1fg$,"r.ir" rp.rti. p
Cause is unknown, but is a degenerative condition with no knowntriggers
This rare disorder usually presents as slowly progressive spasticparaparesis, which eventually progresses to include the upperextremities.
It sometimes is considered a variant of ALS. ln many cases that arefollowed for long periods of time, some lower motor neuroninvolvement eventually develops.
Age of onset usually is in the fifth or sixth decade and equalincidence between the sexes.
atory studies . Routine labs are normal, multiple labs are performed to look forreversible causes.
. lmaging of the spine is normal. MRI usually is performed.Myelography can occasionally show structural abnormalities notseen on MRI.
losts PLS is considered with a patient has progressive paraparesis andimaging studies do not show a structural cause.
PLS is a diagnosis of exclusion, only after ruling out multiplesclerosis, hydrocephalus, cervical spondylotic myelopathy, B,,deficiency, adrenomyeloneuropathy, HTLV-l infection, Lyme disease,and other identifiable causes of gradually progressive myelopathy.
ential diagnosis Amyotrophic loterol sclerosis. Considered in the differentialdiagnosis. Some patients, when followed over long period of time,will eventually develop lower motor neuron findings. Before this,PLS patients do not have denervation on EMC.
Spinol cord /esron. Always in the differential diagnosis. Spondyloticmyelopathy features prominently in the differential diagnosis. Othercauses include tumors, vascular malformations, and disc disease.The absence of back pain and imaging abnormalities favors pLS.
Tronsverse myelitis. A demyelinating disorder related to multiplesclerosis. Myelopathy can occur with TM or MS, and typicallyProgresses over a few days without a later progression.
There is no known treatment for the disorder itself, but spasticity maybe partially ameliorated with the use of baclofen or tizanidine.
al course Patients progress slowly. ln most, the symptoms remain confined tothose of the spinal cord. However, in some individuals, there is laterdevelopment of lower motor neuron degeneration.
558 DISORDERS-NEUROMUSCULAR
*\:w*'
DISORDERS-NEUROA/USCULAR I59

Prlmnry Loterol Sclerosls rurtttnut!
Second thoracic
lascit ulus grar ilis._[-asciculus ( unedlus------------1 \Dorsolateral [ascir ulus- \ \
rl issauer's Zoner \ \
. ;-Marginal zpnt'Lateral corticospinal tract j-----u o
* ' t
Subiontio gcl.rlirros,r
Nur leus pr4rriu.Rubrospinaltrdcl I i "*, -.------------- Nucleus dorsalis o[ ( l,rr l'
Lateral hornVentral :pinocert.bellar lract -
\:iJ,IJ,l..ri',,.,,,,,.,,Anterolateral system---l:-- .r\ ru----7-::t;':':il;;
,' * ,1,, Sub5iantia gelatinosa
l,rt'r.rl r.rtirrrspinrl lr,:tt--- i,1) Nutleuspropriu:
\1( ntrnl suinocerebellar tract --*-. lX N. @ -- ,f-:Jruil;;Anlerulalcral svslem- Vttt \ \#*--=---,Spin,,thalamit trartand \ )
-lowermulornouronsspinoreticular trac0 ., , . l,,t I I .:,:, in anterior horn
l,rlt,ral (medullary) reticulospinal rr^rt--J7/ | | |Lateral vestibuloi pinal tractJ/ | | nlnt"rio, *hite commissure
Medial (pontine) reticulospinal tract / | ,Vedial longitudinal fasciculus
Anterior corticospinal tract
First lumbar
Prlmory Ltrterol Sclerosls onnntk\t
Anterior corticospinal trJct
------- Marginal zone
.f Substantia gelatinosaNut leus proprius
ffi1i:,f:i:*,ilI:I;, -l x\K '1i cerrcor mn
spinorericurar rracr , ,l\ ) f:;,'"['Ji:,,';'""''Lateral rmedullaryr retir ulospinal nact----,/// / | ' I I'
Laterai vestibu lospinal traa--J ,/ | | ,qhterio, *nite commissureMedirl rpontiner retitulospinal lratlJ I l4bdial longirudin,rl last iculus
I ighlh llxrr.rcir'l.rr, rr ulrrrlir,rr rlr.--1
| )rr1s,rl.rlr.r,rl l.rsr ir ulrr'-------1 \lisr,rttlr's,/rrttt.r \
I )ors,rl spirtrx t'ru'lx'llar tract + I
| -- - nmAnterior(orti(ospinJl lra( I , *o
Descending monoamine axons(noradrenergic, serotonergic)
Descending fibers from hypothalamusand brain stem to spinal cord
Fasciculus gracilis
Dorsolateral fasciculus(Lissauer s Zone)
Dorsal spinocerebellar tract-.,Lateral corticospinal tract+ r i
i" Perkins}{5. MTA
Third lumbar[rs, ir ulus grat ilis-------1
Dorsolaleral lascir ulus \tlirsauer's lone, a
,
llnr,IV
Rubrospinaltract------:-"*'V-l]..,x,ll..+-Nrc]eusdorsaIis
Anterior corticospinal tracl
35O DISORDERS-NEUROMUSCULAR DISORDERS-NEUROMUSCULAR 16I

HEREDITARY SPASIIC PARPARTSIS (HSP)
Description Also known as familial spastic paraparesis and Strurrlpt'll lott,tttt.syndrome, this heterogeneous grouP of disorders prodtttcsgradually progressive spastic weakness, usually confined to tlrclower extremities.
The degree of weakness is variable. Numerous families have lrt','tdescribed.
Pathophysiology Causative genes have been identified on chromosomes x, 2, 3, t
11,12,14,,l5, and 19.
The most common mode of inheritance is autosomal dominant,although X-linked and autosomal recessive inheritance has beerrdescribed.
Clinical findings Patients present with progressive weakness, usually confined tolegs.
Exam shows spasticity, with increased tone in the legs and upgrplantar responses. Cait is stiff and awkward. Balance clearly is
impaired.
Laboratory studies . Routine Iabs are normal.
. lmaging of the spine shows no abnormalities.
. EMC shows no abnormalities on routine testing.
. Evoked potentials have been reported to show impaired conductof the ascending sensory axons through the cord.
Diagnosis Diagnosis largely is based upon positive family history in theappiopriate clinical setting. The clinical finding of extremely briskreflexes, brisk abdominal reflexes, and downgoing toes to Plantarstimulation are strongly suggestive of this disorder.
MRI of the spine is performed to look for structural cause and is
negative.
Labs for other causes of myelopathy, including B,, deficiency andHTLV-1, are commonly performed and would be negative in HSP.
Differential diagnosis Cord compressron. From any cause, can have identical clinicalpresentation; although this would not be expected to be familial.
8,, deficiency. Can produce myelopathy. Not all patients will havrother neurologic and hematologic stigmata of 8,, deficiency.
HTLV-t-associoted myelopothy. A progressive myelopathy that ca
have a similar presentation.
Management Treatment is symptomatic and family counseling is advisable.
Antispasticity agents such as baclofen, tizanidine, and thebenzodiazepines, are helpful for management of the spasticity.
Therapy and continued activity are important for maintenance ofcontinued mobility.
Clinical course The neurologic deficit is progressive. There are no treatments thatalter the course of the weakness.
I ltrlrltltrr y S;rrtsltt l'tttrtlrrltt'sis
.i I tl
lrill
rll,l
llllV I Assor rrrlt'rl Mycloprrllty
tlr,'
oilrll lnosts
l,,t:
,rgemen
ave
can
rllr( )n
,1rlrysiokrgy
,rl tindings
IrTLV,r A:isOCrAr[D MYTLOPATHY (HAM)rNoPtcAt. S/A{IIC PAITESIS oSP)
A pirjryrirg illr"tt ""d"
. HTLV-1 is the causative agent for adult T-cell leukemia and for TSP.
lnfection results in inflammatory infiltration and degenerationaffecting the spinal cord and brain white matter.
. HAM presents as a gradually progressive, often dysesthetic spasticparaparesis, with age of onset typically after 30. The arms can beaffected, as well, although less so than the legs.
. ln contrast to most other pure upper motor neuron conditions,bladder dysfunction commonly is seen.
,rtory studies Routine labs usually are normal.
HTLV-l testing is confirmatory of infection
HAM is suspected in a patient with myelopathy without a structuralcause having been identified. ln these patients, MS, B, deficiency,and HAM should be considered and tested for.
Diagnosis rests upon HTLV-l-specific antibody or PCR testing ofblood and CSF.
lmaging is normal.
CSF often is obtained and shows no specific abnormalities.
ential diagnosis . Multiple sc/erosrs. Can present with myelopathy with a subacuteonset.
. 812 deficiency- Can produce myelopathy, and the patient may havenone of the other hematologic or neurologic stigmata of 8,,deficiency.
t Atthough there are a plethora of agents now available for treatmentof HTLV-Ill, there is no known treatment for HTLV-|.
lmmune-modulating therapy occasionally is helpful-plasmaexchange and corticosteroids have been tried with only temporarybenefit.
Management of spasticity is supportive. Baclofen, tizanidine, anddiazepam commonly are used.
al course Progressive symptoms are expected, and there is no treatment thatalters the course of the disease.
562 l)t!( )tit)t lis NtLlRol\/LlscUtAR DISORDERS NEUROMUSCULAR 565

SPINAI. MUSCULAR AINOPHY (SMA)
Description Progressive lower motor neuron degeneration, predorrrin.rrrlly rrr
childhood
Pathophysiology SMA is a genetically transmitted disease with predominantlyautosomal recessive transmission, although rare X-linked andautosomal-dominant cases have been described.
The primary causative gene is the SfflN-/ gene on chromosomea gene unique to humans. Absence of SMN-l protein functionleads to premature death of spinal motor neurons.
Clinical findings Spinal muscular atrophy is one of the leading causes of childhoodneurologic disability-with an incidence of 1/6000-1 /9000 births.
Age of onset is correlated with amount of protein function and isdivided into four broad categories:
Eorly-onset type I , usually evident in infancy, also is known aWerdnig-Hoffmonn disease. Severe generalized flaccid weaknis noted, leading to death by the age of tuvo-usually as acomplication of respiratory failure.
When symptoms arise in childhood after the age of l8 montftype lll, or Kugelberg-Welander diseose, is diagnosed. Symptrare identical, but severity is milder and patients usually survivwell into adulthood.
Type ll is intermediate in onset and severity between types I i
lll, but there is no corresponding eponym. ln Type ll SMA, on:is behnreen 6 and l8 months. Patients never walk, but survivainto adulthood is common.
SMA type lV, or adult-onset spinol musculor otrophy, isexceedingly rare and not associated with the SMIVJ gene.Gradually progressive limb-girdle weakness with onset after a20 is seen, along with prominent fasciculations and lack ofrespiratory muscle involvement.
None of the patients have upper motor neuron findings.
Laboratory studies . Routine labs are normal.
. lmaging is normal. MRI often is done to look for a spinal causeIower motor neuron degeneration.
. EMC shows denervation, commonly with acute and chronicfeatures.
. Muscle biopsy shows denervation, and commonly is done to locfor myopathies, which occasionally can be difficult to distinguishfrom SMA, especially in the very young.
Diagnosis Electrodiagnostic testing, muscle biopsy, and genetic assays arehelpful in diagnosing these disorders.
Spirrrrl Mrrs< ul(u n ltl)l)lty
t rrllcrr.rrli.rl diagnosis
Spittrrl Mrrscrrltu' Atnrplry
SPlNAl. MUSCULAR ATROPHY (SMA)*cont'd
- Antyotrophic loterol sclerosis. A degeneration of the upper andlower motor neurons. ALS is not seen in youth. Also, corticospinaltract signs are not seen in SMA.
. Metobolic myopathies. Can present in childhood with weakness.They are mainly differentiated by muscle biopsy, although somehave manifestations on blood testing.
rown asweaknes,,SA
months,Symptorrr',survtve
/Pes I ar)(l/lA, ons('lsurvival
Iook
very
a8('
. Treatment is supportive. Patients will have the need for therapy,training in adaptive skills, and medical devices later in the course.
. There have been no treatments found effective for limiting theneuronal degeneration.
Weakness is progressive, although very slowly for some.
364 DISORDERS-NEUROfulUSCULARDISORDERS-NEUROMUSCULAR 365

Spittrrl Mttsr ttlrtt Al trrlrlty,,,ttr,t,,l f Arrryolroplrtr l rrlt'trrl Sr lt'rosis
Wcrrlrrig-l lo[[lrr.rnrr I )isc,rsc
Muscle biopsv specimen shrxving groupsof smarll atrurphic rrusclc fibcrs andarcas of normal or enlarged iibersigroup atrophy). (Trichrome stain)
:.,...
lni.rnt u ith l) pir ,rl lr.ll .lt,rP.rl th,,r.rr ir.g-h,g ':lp,,\ru ,. , nd :1ug hrr,rll,, p,,.,,,", .irrrplil,i,,r'. ::ll:,:;:''1.::llll, J.alrocar(togrJnt
,,,,Erec*omyosraphy (molor ;r' ;:; "",,* "r,,,"",,;l:rtrucardiogrrnr, \il,\{t '#,
llov rvith much t {
fr,1,;1- ,,t{-[,iitHr;::*werdnig-Ho{tmann disease {
,i r ll )l t( |t I
I roIrlry',i1;l6gy
rr, ,rl tirrdings
AMyo r H()r,r il(: r:ll"llltll9tERosrs (ALs)
Also l<rrowrr as "Lou Cehrig's disease," this is the prototypic motorncuron disease.
Degeneration of the upper and lower motor neurons is of unknowncause.
The usual clinical pattern is one of progressive painless generalizedweakness, often asymmetric at least at onset. Fasciculations andmuscle cramping are often seen both clinically andelectrophysiologically.
Because motor neurons both in the brain and spinal cord areaffected, there is a combination of upper-motor neuron and lower-motor neuron signs on neurologic examination.
Bowel and bladder functions are spared, but brainstem motorfunction and respiration are always eventually affected.
The disease typically strikes adults in the fifth decade and beyond,although age of onset varies. There is no difference in incidencebetween sexes.
As the disease progresses, significant weight loss occurs as a resultof loss of muscle mass. Disease duration is a dismal 2-5 years,and if there is significant brainstem involvement at the time ofdiagnosis, duration is much shorter.
oratory studies Routine labs are normal.
lmaging shows no significant cord compression or lesion.
EMC shows widespread denervation changes, as does musclebiopsy.
Muscle biopsy shows denervation, but is not needed for diagnosisin most patients.
rqnOSlS ALS is a clinical diagnosis. The combination of progressive weaknesswith fasciculations, atrophy, and upper motor neuron findingssupports the diagnosis.
lmaging of the cord usually is needed to rule out cervicalmyelopathy.
EMG is needed to document the lower motor neuron degenerationin at least three extremities.
[erential diagnosis Cervicol spondylosis. Can produce progressive weakness of thearms, with lower motor unit dysfunction in the hands and uppermotor unit dysfunction in the legs from cord compression. lmagingis needed for diagnosis. Some patients with ALS undergo cervicaldecompressions when there is doubt about the diagnosis, but atleast some of this is unavoidable.
Myosthenia grovis. Considered in patients with progressiveweakness without sensory symptoms. Ptosis and diplopia are notexpected in ALS, whereas they are common in MC.
Multifocol motot neuropothy. An autoimmune disorder characterizedby weakness without sensory changes.
3s;,r-{iff:
566 DISORDERS-NEUROMUSCULAR DISORDTRS_NTURON/USCUI AR 567

Management
Clinical course
Atttyrrlt'ollltit l.ttlt'tttl St lt'trrsis tt\tti,,tt
AMyoTROPHIC LATERAL SCIERoSIS (ALS)--<ont'd
Riluzole is the only medication approved for treatment ol ALS irr
the United States. Not all patients take riluzole, due to uncertarrrlythat the balance of benefit, cost, and adverse effects favorsadministration.
The remainder of treatment is supportive and palliative.
Progression is expected, with patients losing independence.
Patients should decide about whether they want tube feedings arrrlintubation with mechanical ventilation Prior to these issuesapproaching crisis. Some patients may decide that they want tohave complete support, whereas others will decide to withholdsome or all of these supports. Most physicians feel these decisiotr',are within the rights of the patient, and it is wrong to imposedecisions on them.
Fine movements of hand impaired; prominent metacarpalbones indicate atrophy of intcrossei muscles
Weak, dragging gait;foot drop or earlyfatigue on walking
Clinical signs
AtttyoIlo1rlrit l.rrIt'r'rrI S< lt,r'o.sis
Y
368 DISORDERS-NEURON/USCULAR DISORDERS*NEUROMUSCULAR 569

l)olto rut(l l'osl 1rolio Syrrrltonrr,
PARALYTIC POLIO AND POST.POTIO SYNDROMT
Paralytic polio has virtually vanished. Patients presentasymmetric paralysis.
l'olto rrnrl l'}osl polio Sytrrllotrrc
I'Al(Al.Y I l( l'()l.l() ANI) POST-POlfO SYruOnOfvfi-contid
l\rrolyti< lxtlio is suspected when a patient presents with muscle painfollowed by asymmetric weakness in association with a febrile illness,which begins days to weeks prior to the neurologic symptoms. Thisprodromal phase is typical of a viral illness with fever, sore throat,headache, nausea, and muscle aches. A virus can be detected in stoolsamples and also can be obtained from throat culture done early inthe course. lsolation of virus from the CSF is rare.
Post-polio syndrome is suspected when a patient with a history ofpolio has progressive weakness. EMG shows denervation- No othercause of neuronal degeneration is identified.
Parolytic polio. Essentially eradicated from the world as drr irrft.< trorr.,disease, it is caused by a picornavirus transmitted by the fecal or,rlroute. Remaining polio outbreaks usually are due to politicallymotivated boycotts of worldwide vaccination programs. Extrenrt.lyrare cases of polio occur as a result of the oral polio vaccine at ,i r.,r,of about I case per 2.5 million exposures.
Pgst-polio syndrome. The exact cause of this syndrome is unknowrrThere is no reported evidence of viremia in these cases. Acceptarrr .that the syndrome exists is not universal.
. Creater than 95o/o of persons infected with polio will experienctasymptomatic viremia and spontaneous clearing. Fewer than lrXr olexposed persons develop neurologic symptoms, although 2o/o 3t't,,will develop a viral meningitis, and another I0o/o will have a brit,lflulike illness.
. WlSn neurologic symptoms develop, they do so following a brit,lflulike prodrome; followed by severe generalized myalgiai withfocal, often.asym_metric, fasciculations; which is then followed byweakness that often is severe. The legs often are most affected,although any muscle or region can be involved, includingdiaphragm and bulbar muscles.
. Recovery typically is incomplete, with atrophy and asymmetricweakness that often is permanent. The remaining motor neuronswill undergo axonal sprouting so that partial reinnervation occurs,Ieading to some degree of recovery. This results in very large molorunits noted in electromyographic testing.
Post-polio syndrome:. Occasionally a syndrome develops in former paralytic polio victinrs
several years following the initial attack.. Patients typically complain of diffuse myalgias and recurrence of
weakness in muscles that were affected in the initial attack.. The lag between the initial attack and development of so-called
post-polio syndrome often is measured in detades.
lololytic polro. Routine labs are normal. lmaging is normal or showsinllammatory changes in the spinal cord with- high-resolution imagesCSF shows pleocytosis, which is initially polymorphonuclear, then"evolves to lymphocytic.
Post-polio syndrome. The diagnosis is more secure when newdenervation can be discovered by electromyography in the absenceof any other cause. This finding has suggesied the hypothesis that tlr,remaining pool of motor neurons has begun to age, fatigue, orotherwise wear ou_t prematurely as a result of dramatically increasedworkload. ln the absence of definitive EMC abnormalities, there ishesitation to suggest this diagnosis.
t , tlorential diagnosis
I L rlraSement
r rnical course
Pathophysiology
Clinical findings
Laboratory studies
Peripherol neurcpothy. ln a patient with previous polio, it canproduce what appears to be the post-polio syndrome. AIDB CIDBother immune-mediated neuropathies, and idiopathic peripheralneuropathies superimposed on the chronic axonal damage all haveto be considered.
Motor neuron drseoses. lncluding ALS, are considered in thedifferential diagnosis of post-polio syndrome. Corticospinal tractsigns suggest the more ominous diagnosis.
Porolytic polio.There is no treatment for the underlying infection.Therapy and support are the mainstays of management.
Post-polio syndrome. Support and therapy are needed for thesepatients, with an aim to maintain mobility and functionality. Somehave expressed concern that exercise may worsen the function inthese patients, but there is no evidence of this.
. Most patients with paralytic polio eventually improve, although therecovery is protracted and incomplete.
. Post-polio syndrome is a chronic condition and requires continuedactivity.
570 DISORDERS-NEUROMUSCULAR DISORDERS-NEUROMUSCULAR 577

l'olio rrrrrl I'osl-polio Sytttltf rtttc t trtttnut,tl
Paralytic residua ofspinal poliomyelitis :$a
c
iI1Ij
#*']i /,
il NctttotIttts( ul(Ir' Ittrtt lirlrr [)isortlcrs
Multiplc cripplingdeformities:contracturos,atrophy, severescol iosis andequ r novarus i
i-,f
d,1,, ,
I1' 'Y'+'",, ,il.hl. l*.Jr
ur{{$d -
I r)mmOnl, dtur€S
( oll.]monllatures
Myasthenic(l ambert-E',vndrome
lIotulism
Gcnurecu rvatum,atrophyof limb ,#.
, .lt)rt f,bi*' 1 .-., il..ttt;'ii.i '
t],)Ifl1
,.,f] il!'
N'ly
ovrl
st riptiorr
vlly 9r NIUI
These disorders cause weakness by interfering with the transmissionfrom the motor axon to the muscle fiber.
hophysiology Three disorders comprise the most important neuromusculartransmission problems:
Myasthenia
Myasthenic (Lambert-Eaton) syndrome
Botulism
resclinical . Patients present with weakness and often autonomic symptoms,
indicating a deficit in cholinergic transmission.
. Fatigability is common, with a significant drop-off in strength withrepetitive activity.
reslaboratory . There are lab tests for these disorders, discussed on the following
Pages.. NCS shows abnormal responses to repetitive stimulation, with
changes that differ depending on the disorder.
Disorder Essentiol Feotures
asthenia Antibodies to the acetylcholine receptor produce impairedneuromuscular transmission.
Ocular myasthenia is weakness confined to the extraocular musclesand eyelids.
Myasthenia gravis is generalized weakness in addition to ocularweakness.
tcEaton)
Lambert-Eaton myasthenic syndrome (LEMS) often is related tocancer, particularly of the lung. Patients present with weakness andfatigability, and typically have autonomic symptoms.
. Exposure to the toxin Clostridium botulinum produces failure ofneuromuscular transmission.
. Patients have weakness that progresses rapidly and has a slowrecovery.
q: 'r,t61,,
riffi'
572 DISORDERS-NEUROMUSCULAR DISORDERS-NEUROMUSCULAR 575

Nctttoiltttsr'ttlrtI f ttttt tiott I)isotilcls tt,rtrrlrlt
N cu rom uscu l.t r Tra nsrl ission
t My<rstlrt'rritr
Myclin shcath
Neurilemnra
;- Axoplasm
IMv.iib,il, //
[
Synrptit r left
Bascment mt:nrl rr,rr,,
Sarcolemnr.r
\ttrNucleus olmusclc ct'll
Postsynapticmenr b ra ne
!1..
&i ir:i
ia.'ii 'Iliil"tli' r.i$ {l
:(1i:"..ir
lunclional fold
Sart,rplr:mAcetylcholine receptor sites
rboratory
lr agnosis
-z 5thuenn ccll
-.,/- MitorhondriaBasement membrane
Ntrcleus of Schlvann ce]l
Pres) nrptic nreml;reno
Active zoneSl,naptic vcsiclcs
Il'
,( ill)lton
lrophysiology
MYl|I$n$
-
ALrto.rrtibodies against the acetylcholine receptor produce weaknessthdt can affect the entire body or only eye movement.
Autoantibodies bind to the acetylcholine receptor and causeincreased receptor degradation. The combination of the binding andthe turnover effects results loss of receptor so that an actionpotential in the motor neuron does not always result in an actionpotential in the muscle fiber. The normal l-to-l transmission frommotor axon to muscle fiber breaks down.
The cause of the autoantibodies is not known. The thymus isimplicated in the inception and generation of the autoantibodies.
Thymoma is present in some patients with myasthenia.
rical findings Myasthenia presents in hruo ways-ocular and generalized(myasthenia gravis).
Oculor myosthenro is characterized by ptosis and weakness of eyemovement that cannot be explained by a single ocular motor nerveor muscle lesion. Both eyes are affected, although not equally so.Patients with pure ocular involvement at onset usually remain pureocular; however, some will progress to generalized myasthenia.
Myasthenia grovis (MG) is characterized by weakness not only ofthe ocular muscles, but also of bulbar and extremity muscles.Dysarthria, dysphagia, and weakness with arising from a chair aresome of the common symptoms.
There are no sensory findings.
Weakness tends to be better in the morning and worse later in theday.
studies Routine labs are normal. Myasthenia antibody testing showsabnormalities in most patients.
EMG often shows no abnormalities on routine testing, but repetitivestimulation usually shows a decremental response from the musclewith stimulation rates of 5/sec. Single fiber EMC shows increasedjitter.
CT of the chest may show thymoma.
Myasthenia is suspected when a patient presents with diplopia andptosis. Bilateral symptoms are more commonly myasthenia thanunilateral.
Ceneralized weakness, especially with dysarthria and dysphagia,along with the bulbar weakness, supports the diagnosis ofmyasthenia gravis.
Myasthenia antibodies can confirm the diagnosis.
Chest CT is done on patients with myasthenia to look for thymoma.
574 DISORDERS-NEt]ROMtJSCtJLAR DISORDERS-NEUROMUSCULAR 575

Differential diagnosis
Management
Myrrst ltr,tt irt, t,tturrt tl
. Myosthenic (Eoton-Lambert) syndrome. A paraneoplastit syrrtlroIrrr.characterized by diffuse weakness and autonomic deficits.'Paraneoplastic antibodies can help to make this differentialiorr. I M(,special testing also can suggest myasthenic syndrome rather llr,rnmyasthenia, although not all EMC machines have the capabilily otthis testing.
. lnflommotory ryyopothy. Patients with polymyositis can presenl wrrl,weakness and fatigue without sensory deficit. EMC showsmyopathic features. CPK is elevated.
'
. Weakness is.managed by aceytlcholinesterase inhibitors. Long-tt,r rrrtherapy is with immune suppiession. Crisis is managed with llasru,,exchange or lVlC.
. lmmune suppression is a cornerstone of treatment withmyasthenia, and mainly is used for people with generalizedmyasthenia-m.yasthenia gravis. Corficosteroids, such as prednisorrr,,a.re begun as daily dosing, and ultimately adjusted to an alternatirrllday dosing schedule. The dose is taperei, so that most patients .rr,,able to get.to a low.alternating-day'dosing schedule. Strongeragents, such as azathioprine and other chemotherapy agenls, alsoare used, but are less common.
. Acetylcholinesterase inhibitors are used for most patients withocular myasthenia and myasthenia gravis. These are purelysymptomatic and not disease-altering. They inhibit the breakdowrrof acetylcholine at the neuromusculai junction, thereby improvingtransmission.
. Thymectomy is performed for patients with thymoma, and inpatients who have not had adequate response to immunemodulation treatment.
. lntravenous immuoglobulin (lVlG) is used for some patients incrisis, and can help to improve strength. The risk is relatively lowwith close monitoring of the patients.
. Plasma exchange (PE) is used for patients with crisis, and can be oltremendous benefit. PE often is often used if IVIG is not tolerated,contraindicated, or ineffective.
My,rsllx.rri.r (,r,rvis: ( lirrical M.rnifcslationsMYASTHENIA*cont'd
Ptosis and weakness of smileare common early signs
lmprovement afteredrophonium chloride
Mytrstltt,rrirr
&-i&
it
lmprovement is expected, although most patients are maintainedon a low-dose corticosteroid aftei their initial tapering.
Crisis may develop requiring hospitalization, administration or lvlCor PE, and/or transient increases in corticosteroids.
II\
']/\it Itrll{/)\t\l\ il i\\l //rt \/.dtJ,!
3O.k 1O.k
Regional distributionof muscle weakness
Patient with chinon chest cannotresist whenphysician pusheshead back
r- t't r{,VI L;Y,.r
.8 t',t' \' '
576 DISORDERS-NEUROMUSCULAR DISORDERS-NEUROMUSCULAR 377

LAMBERT-EATON MYASTnENIC SYNDROME (t.tMS)
Description Autoimmune disease affecting the neuromuscular juncliorr
Associated with cancer, especially small cell lung cancer
Pathophysiology . LEMS is a prototypic paraneoplastic condition. The most cornrn()associated cancer is small cell lung cancer.
. Most patients have antibodies to voltage-gated calcium chanrrt'ls(vccc).
. The deficit is in transmitter release.
Clinical findings . LEMS presents with a weakness and fatigue, mainly affectingproximal muscles.
. Autonomic symptoms, including dry mouth, constipation,impotence, and bladder dysfunction, are common.
. Tendon reflexes are decreased.
Laboratory studies . Routine labs are normal.
. Paraneoplastic panel shows antibodies to the voltage-gated calcirchannel.
. lmaging of the brain and spine is normal. lmaging of the chest irdone to look for neoplasm, and often is positive.
. NCS and EMC show an incremental response to repetitivestimulation at high rates.
. Positron emission tomography (PET) can be performed to look f<
cancer.
Diagnosis LEMS is considered when a patient presents with proximalweakness. Myopathy usually is considered first, but EMG does r
show myopathic features and CK typically is not elevated.Paraneoplastic panel is ordered, whether or not there is a knovcancer.
Diagnosis is confirmed by NCS, EMC, and the VGCC antibodies.
Vigilance for cancer must continue after diagnosis-many montlmay elapse between development of any paraneoplastic conditand diagnosis of the cancer.
Differential diagnosis . Myosthenio grovis. The main differential diagnosis. Patients presrwith weakness and abnormal response to repetitive stimulation,the pattern of abnormality is different. Also, there are differentresults of antibody testing with MC, as opposed to LEMS.
. ALS. Considered in patients with progressive weakness, althoughthe weakness is more prominent distally. Also, corticospinal tractsigns are seen in ALS, but not LEMS.
Management . Guanidine, diaminopyridine, and pyridostigmine are used toimprove strength of patients with LEMS, especially for diseaseis not associated with malignancy.
. Immune-modulating therapy often is used, including corticost(lVlG, or plasma exchange.
Clinical course LEMS is a chronic condition, requiring continuing treatment.
Vigilance for the late development of cancer is needed.
l.rttttlrct t l.ttlott [VlytrslItr,tIir Sytttltolrrt,
rly
I rrrrtlrr,rl I rrlott Myrrslltt'ttir Syttrllotttc
X r,l,lilrn shorving largetunror in hilunr of lung
Acct,vlcholinc lACh) rclcast:at neuromuscular. junctionrlt:creased; sparse, disorg.rnizcd activcr zoncsior ACh release
fa.5a
-
Nerve axon
Synapti c
vcsic les
i'j;
flrl
Ir
I]
oes nol
known
,dies.
nonthsonditiorr
Presenltion- lrrrl
ease thal
icosteroitl',
,aij,-::i,
!"--;*l= -r
) !--t1it riLr Lrltv in c limbing stairs orrrg from chair otien earl,v
lrtom due to weaknessr'lvic girdlc muscles
l ow-amplituder (,sponse
Dryncss of mouth due todecreased saliva secrction
Rostccl I Excrcisemuscle | 10 seconds
l<---------->
Electromyography with voluntary exerciseEach tracing represents -i superimposed action potentials evokod by stimulation
3 minrJtesafter exercise
7 Drop-uff/ greater th.rn
, rt rest
-,\-Depressedresponse
3 secondsaftcr excrcisc
Creatly increasedrcsponse (over200'1,); no drop-off
at 3/second
I0 minutesa{ter exerclse
Return torested response
7 Slightl/ drop-cft
578 DISORDERS-NEUROMUSCULAR DISORDERS-NEUROMUSCULAR 579

BOTULISM
Description Paralyzing illness due to toxin ol C. botulinum strains
Pathophysiology . Botulinum toxin is produced by clostridium strains in anacrobicconditions.
. The toxin binds to the presynaptic terminal and prevents releascacetylcholine from the terminal.
. Exposure to botulinum toxin is from food or wound infection.lnjections of botulinum toxin can produce localized weakness, bsystemic botulism does not occur at therapeutic doses.
Clinical findings Botulism presents with autonomic symptoms, including nausea,abdominal cramps, diarrhea or constipation, followed bygeneralized weakness. Weakness of ocular motor and bulbarmuscles also is present. Pupillary constriction is impaired as well
Laboratory studies Routine labs are normal.
lmaging of the brain and spine is normal. lmaging often isperformed of the brain when there are bulbar signs; of the spinewhen extremity weakness predominates.
NCS and EMG show reduced amplitude of the compound motoraction potential. Special testing may show an incremental responto high rates of repetitive stimulation and an augmentation ofresponse with exercise. The response often is patchy, with somemuscles being normal.
Diagnosis . Botulism is suspected when a patient presents with rapidlyprogressive weakness in the setting of autonomic symptoms shpredating the weakness.
. Diagnosis is supported by the typical electrophysiologic studies.
. Toxin can be assayed in body fluids and foods. lsolation of thebacterium without the toxin does not make the diagnosis.
Differential diagnosis Myasthenio grovrs. Presents with ocular motor weakness andgeneralized muscle weakness. Autonomic symptoms are notprominent. Also, the NCS and EMC findings differ with slow andfast repetitive stimulation.
Lombert-Eoton myosthenic syndrome. Presents with weakness aautonomic symptoms, although this is not a fulminant presentatas with botulism.
Management . Supportive treatment is essential and typically can be difficult.. Antitoxin is administered whenever possible, and is available
the CDC.
. Antibiotics are used for patients with wound botulism.
Clinical course Most patients improve with treatment, although the improvementprotracted and incomplete.
llolrr lisrrr
( h)'Iti(IiutD botulinumrvirlt,lv rlistributed in nature;r ,rr r it's hc.rt-rcsistant spores
{.'{k"-".***
'\,
I rtrxluced into, rrlrrurperly
1 't I'scrved
1, x)(lS
Tox i ns
absorbedfromintestine
Specific organismnot isolated. Algaethat redden watercarry it intoshellfish (clams)
Causative organisms of each o{ thesediscases, or exotoxins produced bythem, arc intrcduced into Cl tract
Cl upset of variablcseverity occurs in Iall ] diseases i
llot rt Iistn
Cigualcra
"r,j
Ciguatoxin attacksperipheral nerve, exactsite unknown.Weakness, paralysis,radicular pain occur.Prognosis generally good
ll rl rrl irrtr
" *llf
\lrclllish (rr,rl tirk')lloisorring
" tt[{,l0 ,,
' ,fo] ,
but
resPons(,10f
shortly
1t{il,I
."1'
,{ -"'*-\- .!' r
'q{-.#r),'Xl
-/--.-,i<..-
T1
Botu I i n:i ncubationperiod about24 hours
Shellfish toxln;incubation maybe less than ,30 minutes ,'
{--"" --; -:- "-lantlttior r
fronr
Eotulin attacksneuromuscular junction.Weakness, paralysis, respir-atory distress occur.Prognosis variable, maybe fatal
Shellfish toxln attackr' 'peripheral motor neuroo, , .Weakness, patalyslr, reepira-tory distress, iaresthesias , .'oceur. Prognosls vartablei..,tretter than in bstirlisit .:'.:-.
i tv:iitii I,:,;,iriii++18:
'.{;i r:.'
;,.* I I**1 r:
..*dj t;.,,r*if,3i;
580 DISORDERS-NEUROMUSCULAR DISORDERS-NEUROMUSCULAR'8I
I
ri
I

( )vclvicw ol Myoprtlltit,s
rn.rlly
SC
canrith
sensorye in f;tvrrr
. Myopathy - myopathic features on EMG. NCS is normal or reduced amplitudes
. Nt.luropathy - neuropathic features on EMG. NCS usually shows slowing +/o reducedrrrnplitudes, depending on the type (axonal, demyelinating)
. Ncuromuscular transmission disorder- EMG often normal. NCS special testing'.lrows impaired transmission
( )vr,rvicw ol Myrllxrllri(,s
My0lrrlhy su-slgctgd. Wr:irkrrcss, tatigue. No sensory symploms
NCS & EMG
OVERVIEW OT MYOT'ATHIT,S
Description Myopathies are muscle degenerations, which can be con13t'rrit,rl oracquired
Pathophysiology The final common pathway to myopathies is muscle degeneratiorr,which is caused by metabolic abnormalities in the muscle, toxins, orinflammation.
Clinical findings Myopathies present with weakness that is most prominent proxin
There are no sensory findings.
Laboratory studies . Muscle enzymes are elevated in most myopathies. Creatine kinasc(CK) and aldolase are usually markedly elevated. Mild elevation caoccur with neuropathy or motor neuron disease or in patients witl"burned-out" late state myopathies.
. lmaging is normal.
. NCS and EMC show myopathic features.
. Biopsy often can be specific about the diagnosis, whether type ofdystrophy or inflammatory myopathy is determined.
Diagnosis . Myopathy is suspected when a patient presents with generalizedweakness that is most prominent proximally. The absence of sen:involvement and the absence of corticospinal tract signs argue inof myopathy.
. Elevated CK and aldolase is supportive of myopathy.
. NCS is normal. EMC shows myopathic features.
. Muscle biopsy often is needed to give the definitive diagnosis.
lmportontMyopothies Essentiol Feotures
lnflammatorymyopathies
. Present with weakness, usually without pain
. Have an association with neoplasms and other autoimmune dise
. Rash with inflammatory myopathy is dermatomyositis.
. Muscle biopsy is diagnostic of the inflammatory component.
Musculardystrophies
. Degenerative conditions characterized by weakness and oftenhypertrophy of the muscles
. Occur in younger patients more than inflammatory myopathies
. Muscle biopsy is diagnostic.
Toxic myopathies . Present with weakness and elevated CK
. The list of possible offending agents is large. Alcohol is one of themost important ones.
Periodic paralyses . A group of disorders that present with attacks of weakness. Otherfeatures differ behrueen subtype.
. Patients usually have normal examination between attacks, althoudevelopment o{ static weakness can occur.
- l)ctermine the type- ( )onsider: dystrophy,
r rflammatory, metabolic,
Myopathy not eonlirmed. Still could be myopathy. Normal (e"9., FMS/CFS). Neuropathy. Neuromuscular transmission def ecl
. lFTs, ANA, ESR, Cortisol,(lPK, aldolase
- Muscle biopsy is, on{irmatOry
. 812, Folate, TFTs, ANA, ESR,Cortisol. CPK, aldolase. SIEP
. Antibody studies for myasthenia,myasthenic syndrome
. Weakness without sensorysymptoms, but withcorticospinal tract signs
. Dx: Clinical and EMG
. Weakness reported withnormal exam
. Labs are normal
. Weakness and fatiguewithout sensory symptoms
. Dx: Lab and NCS specialStUdiCS
. Weakness often withsensory symptoms
. Labs and EMG show thediagnosis
Lambert Eaton Myasthenicsyndrome. Weakness wilh autonomic
symptoms. Dx: Lab and NCS special
studies
Multitocal motorneuropathy. Weakness without sensory
symptoms. Dx: Clinical and EMG
Weakness olten withr ruscle hypertrophyIcPK, atdolasel)x: muscle biopsy
fy'eakness and latigueI ;ibs may show metaboliclr,,fect
382 DISORDERS-NEUROMUSCI.]LAR
althouglr
DISORDERS-NEUROMUSCUI AR 585

Ittllrtttrrrrrrlor y Myoprrllrrr,s
INTLAMMATORY MYOPATHIES_POLYMYOSITIS AN D I)T ITMA I oM Y0IiI I IS
Description lnflammatory myopathies produce weakness, mainly of proxrrrr,rlmuscles. They can be idiopathic or due to other syslcnri< <lisr,,rs,.
Pathophysiology Autoimmune disease, characterized by inflammatory degerrt:r.rtior r
of skeletal muscles. The cause of the immune attack is isuallyunknown, but cancer and connective tissue disease are preseirt rrrsome individuals.
Clinical findings There are three basic types-idiopathic polymyositis, idiopathicdermatomyositis, and inflammatory myopathy associated withconnective tissue or cancer.
Weakness is the most prominent symptom, mainly of proximalmuscles. Dysarthria and dysphagia are common, as is weakness olneck muscles; head instability is a common presenting sign.
Pain is not common, despite the inflammatory pathophysiology.Muscle pain without weakness is not polymyositis.
Reflexes are normal or slightly depressed.
Sensory function is normal.
Rash is seen in patients with dermatomyositis, and can be variablt,Rash across the cheeks, bridge of the nose, and dorsum of thehands can be seen.
lf the inflammatory myopathy is due to connective tissue disease,the common associations are lupus, rheumatoid arthritis, mixedconnective tissue disease, and scleroderma.
lnflammatory.myopathy due to cancer may be due to lung, breast,ovarian, or colon neoplasms.
Laboratory studies . Routine bloods are normal, but CK and aldolase are increased.. lmaging is usually not needed, but if the inflammatory myopathy is
thought to be due to malignancy, then body pET may'be revealing.. Paraneoplastic panel may be positive, and search for cancer should
always be considered.
. EMC shows myopathic features in the vast majority of patients.
. Muscle biopsy shows inflammatory changes in most patients.
Diagnosis . Polymyositis.is suspected when a patient presents with proximalweakness without pain or sensory abnormality.
. Diagnosis can be confirmed by elevated CK and aldolase,myopathic changes on EMG, and characteristic features of musclebiopsy. However, not all of these features will be present, but thediagnosis is secure with three of the four basic features.
. Dermatomyositis is diagnosed by making the diagnosis ofpolymyositis plus the characteristic rash.-
584 DISORDERS-NEUROMUSCULAR DISORDERS NEUROMUSCULAR 585
INI'I AMMAIoRY
,ll, rlltlr,rl rlt,rgttosis
rrical course
llr ll(ilnilr(tlot y Myo;rttl ltir.s
Myosthenio grovis. Ptesents with weakness but also with ocularmotor weakness, which is not expected with polymyositis.
AtS. Can present with dysarthria and dysphagia in addition togeneralized weakness. The weakness is more Prominent distallythan proximally. EMC findings are neuropathic rather thanmyopathic.
M YO I'A I I I I l.s-. . l'o l-YM YOSITIS AND D[RMATOMYOSITIS*-cont'd
- Mttsculur rlystrophy. Presents with proximal muscle weakness, butthe onset is slow. Onset in middle-aged or late adult life is notexpected.
. lmmune suppression results in complete remission for somepatients. Others need continued suppressive therapy. First-linetreatment is with corticosteroid such as Prednisone. lnitial dailydosing is followed by alternate day dosing with a gradual taper.
. Chemotherapy with azathioprine or methotrexate is used forpatients who do not respond to corticosteroids.
Most patients improve with corticosteroids andlor chemotherapy.Some patients have complete response and are able to eventually getoff meds, whereas others continue to require medications.

I tt I lr rttt nr( rl( )r y My, r1 rr tl lt it,s, I't,ttt,,,,i Mttsr ttlrtt I )ysttopltit's
L)crmalomyosilis .ud ltrlyrnyosilis
Ditlicu lty insrvallorving dueb esophagealrvr:akncss
I It.trl lrllrl rrr ll,,r, ,l
llrisilion tlrr, l. 1rt,r trr,rl
trrttsr lc tlr'.rIrtlst
,l
Gc:n*," l: -
[dcma and hcliotropc discolorationof eyelids .rnd erythemabus rash
Erythenratous, nodulareruption on fi ngers
Musc lebiopsv:atrophy ofnruscleiibers anrllymphocytci nfi l lration
Jt1: -,*a:frji:
,ol ,"*-i'j'" #'.r*r'1 ',;li
trx 5"ip:;Ji;r*"u X ",ieq-"f *" "
a
r,":i$ A.;r;. -'rffir,
Fl uorcscenceslide ofmusclcrcvea I i nggamnraglobulirrdcpositionin bloodvessel
i-.. .'i '. 'l
tifferentia
,',( ill)lt()n
rt hophysiology
MUs(rI.AR ryI]lgPt{tES- Mtrsr trl,rr dcgeneration results in progressive weakness.
. The rnuscular dystrophies are hereditary and the responsible genesand gene products have been identified for some.
. Muscular dystrophies are due to genetic errors. The most commonis dystrophin deficiency, responsible for Duchenne and Beckerdystrophy.
. The responsible products for many other types have not beenidentified, but a common thread is genetic defect leading tometabolic derangement leading to muscular degeneration.
ical findings There are many types of muscular dystrophies. Among the mostimportant are:
Duchenne muscular dystrophy
Becker muscular dystrophy
Myotonic dystrophy
Limb-girdle dystrophy
Facioscapulohumeral dystrophy
Scapuloperoneal dystrophy
The common features are weakness most prominent in proximalmuscles and absence of sensory abnormalities. Depending on thesubtype, other findings may include facial and bulbar weakness,muscle hypertrophy, myotonia, and/or cramps.
rboratory studies Routine labs are normal for most Patients. CK and aldolase areelevated for most muscular dystrophies.
Imaging is normal, and not needed for most patients.
EMC shows myopathic features.
Muscle biopsy shows myopathic features, and special studies fordystrophin and other gene products can help with the diagnosis.
iagnosis Muscular dystrophy is suspected in a patient with progressiveweakness, especially with onset in childhood.
Elevated CK and aldolase and myopathic changes on EMC supPortthe diagnosis.
Muscle biopsy confirms the diagnosis.
I diagnosis Spinol musculor otrophy. Considered in a child with weakness. Theweakness is more distal than with MD. Also, EMC and musclebiopsy show neuropathic findings rather than myopathic features.
lnflommotory myopothies. Can present with weakness withoutsensory signs. These can occur in youth, but are more common inolder patients.
aSement Corticosteroids have recently been shown to be effective inpreserving muscle function in children with Duchenne musculardystrophy.
No other treatments have been shown to alter the course of thedisease.
Physical therapy is helpful and is combined with braces, whenneeded.
586 DISORDERS-NEUROMUSCULAR
,4a n
DISORDERS-NEUROMUSCULAR 587

MUSCUL.A,R DYSIROITH I Es--{ont'd
Clinical course Progression is expected. Muscles become weaker.
The calves may show progressive hypertrophy, especially witlrdystrophin deficiency; however, this muscle is ineffectual, andweakness is present.
IndividuolDystrophies Essentiol Feqtures
Duchenne . An X-linked disorder related to dystrophin deficiency
. Patients present with weakness, pseudohypertrophy of the calves,Gower's sign (climbing up self to stand erect).
. Onset is in young childhood, and patients live into late adolescen
. Corticosteroids have recently been shown to maintain mobility, ar
are offered to most patients.
Becker-type . AIso a dystrophinopathy with abnormal dystrophin. This is alsoX-linked.
. Onset is later than with Duchenne dystrophy and patients live toadult life.
. The role of corticosteroids in treatment has not been established
Myotonic An autosomal dominant disorder that presents with weakness ttis more prominent distally. Hatchet facies, cataracts, and glucoseintolerance are other important features.
Limb-girdle . A family of disorders with mainly autosomal dominant inheritanctThe biochemical defects have largely been identified.
. Patients present with weakness that can be predominantly arm, It
scapular, andlor pelvic weakness, depending on the disorder. Thelimb weakness can be more prominent proximally and distally,depending on the disorder.
Facio-scapulo-humeral (FSH)
An autosomal dominant disorder that presents with facial vlfollowed by arm and shoulder girdle weakness. Despite theproximal weakness of the legs is common.
Scapuloperoneal . This is a group of disorders that present with weakness that isprominent in the scapular muscles and in the region of the tibanterior-anterior compartment of the lower leg. lnheritance isautosomal dominant or X-linked recessive.
Mttsr'ttlrtt I )yslloltltit's,rrrrrrirrr,,/
lll( r'
atrrrl
('.
Icg,
th.rl
weaknes,,te name,
tibialis
388 DISORDERS-NEUROMUSCULARDISORDERS-NEUROMUSCULAR I89
I )ur lrcrrrrt' Must ul.rr Dystrophy
d Y8 yrs old,atfected
M rrscrrlrrl I )yst nrplrit,s
Only males affected,but femaies may bccarricrs
dd2 yrs old,.rlli'r lt.d
ii'1..",;'
Minimrl or no s) mptr)ms
5 yrs old,normal
10 yrs old,normal;may ormay notbe carrier
15 yrs old,afiected
I 5 ycars
2 yerars
m.t" ,:* t,
if 1i i: \,] l:
iili14{.
'l tf
; )i ':')
Scvere cripplingdeformities and contractures

Ioxir Myoptrllrit's
TOXIC MYOPATHIEIi
Description Muscle inflammation and degeneration can develop in respottst' lotoxins, which may be drugs.
Pathophysiology The most common toxic myopathy is due to alcohol intoxicatiorr'
Statins have been implicated in causing toxic myopathies'
Types of abnormalities can range from myalgia.without overtpdthology to focal ischemic myopathy to chronic myopathy to actrl
rhabdomyolysis.
Clinical findings . Myatgio is muscle pain and can develop in almost any cause ofmyoiathy. However, myalgia can occur without pathologic.changein'ttre muscle. Myalgia is iommon in patients with statin therapy,
and the incidence in placebo-treated controls is almost the same'
Exam is normal.
- Rhobdomyolysrs presents with muscle pain and.swelling. Muscles..
are weak,'partly due to Pain and partly due to decreased contractilt'ability if the myopathy is severe.
. Focol myopofhy presents with focal muscle pain and swelling'
Laboratory studies . Routine labs are usually normal, although alcoholics often have
chemicat signs including hyponatremia, hypomagnesemia, increased
LFTs, and others.
. Myoglobinuria is seen in patients with rhabdomyolysis.
. EMC is abnormal in patients with rhabdomyolysis, and often shows
signs of acute muscle destruction.
. CK is elevated in patients with myopathy.
. Muscle biopsy shows myopathic changes. ln some patients, focal
ischemic changes can be seen.
. lmaging is usually not needed.
Diagnosis . Myolgio is a clinical diagnosis and often has no.pathologic.. ...orr""lut". CK is performed, but is usually normal or only mildlyincreased-even minor trauma can increase CK'
. Chronic myopothy is suspected with weakness with or without pain
in the absence of sensory findings.
. Rhabdomvolysrs is suspected when a Patient develops swollen and
tender muscies. Elevatid CK, renal insufficiency, and myoglobinuriasupport the diagnosis.
Differential diagnosis . Criticol illness myopothy. Considered in a sick patient withweakness and increased CK, but this occurs usually after at least
7 days of hospital care.
. Benign elevation rn CK. Seen in some patients and is notassoZiated with muscle destruction or risk of renal failure.
. Polyneuropothy from ony couse. Can be associated with mildelevation in C( but EMC shows neuropathic changes rather thanmyopathic changes. Also, there are usually signs of sensoryinvolvement in symptoms, signs, or NCS.
39O DISORDERS-NEUROIMUSCULARDISORDERS-NEUROMUSCULAR 597
t Iirrical course
Ioxir Myoprtlltics
IOXIC MYOPATHIE$-cont'd
. Ir('.rlnr('nt is supportive with discontinuation of the offending agent.
. Statins should be discontinued, if possible. Howevel the incidenceof myopathy due to statins is generally overstated.
Most patients improve, with the degree of residual deficit dependingon magnitude of the problem. Rhabdomyolysis may result inincomplete recovery.

lrrxit Myo;lrtllrils tt,ttrrtt,t
Effects of Alcohol on frrd Organs
Cellular damageEthanol
l't'l'ior li< I'rurtlysis
Acetaldohyde Freera d ica ls
I ntracel I u la rfree radicalsinterferewith cellmembranefunction andprotein synthesisand alter DNA
+
Acctaldehyde damagescytoskeleton and enzymesystems and induccs antibodiesagainst cell components
Hcpalic rlamage includes {atty liver,olr rrh,rlir hlpatiti' and, irrhoris,i
'\ 'N t,.A
, \f L-.-1 t i IFv ".<n
!' :./!
"(. ." , -''Neurologic damageranges from Korsakoiidcmentia to sultclinicalcognitive derfects
Fatty acid cstcrsinterferc withprotein synthesisand mitot:honclrialand ccl I membrancfu nction
Phosphatidylcthanol altersregulatory ancl communicationfunctions of cell mcmbrane
\ZV'Phosphr tir ll,lcthr noI
I )r'\
t',rll
r .boratory
Alcohol causes end-organ damagc via ethanol metabolites and ethanol gcncratedcompounds, which alter structure and function of ccll components
Organ damage
, r&d t*.tHI o.f,-tt,,/d Vu{eS
lmmune system suppressionincreases risk for infection andsome cancers
lncreased risk forspontancous abortion
Cardi,rvastulali\"- ).damagr. inc ludes . '
"*,{
a rrhythrn iasand cardio- tmyopathy t
Tcratogen icefiects may loadto fetal alcoholsyndrom.e
,:" .' "" J i'r.' ,ii
#{+
\( il1)lron
lrophysiology
I'IITIODIC PANAf,YSIS . ..A grotrp ol disorders with a common feature of episodic weakness
Basic types of periodic paralysis are hyperkalemic, hypokalemic, andnormokalemic. All are inherited as autosomal dominant:
Hyperkolemic periodic porolysrs features a marked increase inpotassium increases markedly during the attack.
Hypokolemic periodic porolysrs shows a fall in potassium duringan episode.
Normokalemic periodic potolysris is associated with no change inpotassium but is thought to be related to hyperkalemic periodicparalysis. Potassium loading can cause an attack in someindividuals.
rical findings Periodic paralysis presents with episodic weakness without pain.The pattern differs between elements.
Hyperkalemic periodic paralysis presents with diffuse weakness thatis most prominent after exercise.
Hypokalemic periodic paralysis presents with weakness that is mostprominent after heavy carbohydrate meal or strenuous exercise.Patients may awaken from sleep with paralysis after a precipitatingevent.
Normokalemic periodic paralysis presents similarly to hypokalemicperiodic paralysis.
studies Routine labs are usually normal between attacks. During attacks,there may be an increase or decrease in serum potassium,depending on the subtype of the disorder.
lmaging is normal.
NCS usually is normal. EMG is normal between attacks, unless fixedmyopathic changes develop.
ignosrs Periodic paralysis is suspected when a patient presents withcomplaints of episodic weakness.
Exam is normal.
EMG is normal between attacks, although late in the condition,myopathic findings clinically and on EMC can develop.
ferential diagnosis other causes of myopathy have to be considered, although there arefew disorders with episodic weakness.
nagement . Hyperkalemic periodic paralysis is treated by hydrochlorothiazide,with or without acetazolamide.
. Hypokalemic periodic paralysis is treated by daily administration ofpotassium.
rical course Most patients improve with treatment, although recurrent attacksare common.
Persistent myopathic changes are seen subsequently.
592 DISORDERS-NEUROMUSCULAR DISORDERS-NEURON/USCULAR I9I

l't't itr<lit l'rtt ttlysis ,t,rtrrtttt
ii\.t:
Hylxrkalcnria. ( lttr.trlt.ll.rl rlrr r.lr,rit slt'toitl trtr', llttt,l lr,,',1\,rrrrlll rl'
tli,trrltt',t, r'lr . l, ot,tlr I rsllt otrt,t t t rr rll I
h,vpctlt'ttsiott ttt.tY tttr lttr (' I )(,l,r" l(rrr I
dtplction, rt'sLtl l itrg i rt lt r',tl't tr ",',,,revcn par.rlysis, rtt'llcri,t,,tttrl/.rarrhl'thrni.rs.
dl*' I *{di,rr i rt!
li
l.,a
ii.,
( ritilrtl lllrtlss Myoptrllry
':rr,,."y.f- .,,{'{i&..*.
. *_"
Perioclir: paalysis is usuallv associatecJ
with h,vpol<alcrria lrul traY also occurrrith h1p, 'k,rlemi.r ot tlo'trrrrl,tl''mi''H,vperthvroidism m.rY also be associated
rvith hypol<alenric pt'riotlic paralvsis
t tifferential
14anagement
Hyperkalemia. Arld isorr's rlisc.rse {pri rlar,v.rcirenocortical insrrfiiciency), char,rclcrizer'l hv
bronzing of skitr, rve.tktress, rvcighl loss, ancl
hrp,,llt"i"tr. i.,rt-,t i.rlod ttilh, lcr.rlt',l.etutlr1,,,t.,-.irrm. M,rnilo'l.r:i(,tl-,n.,t 1,, p;l.l in''.r' lr\l.rB('5. \\ illr rr c.'ln,'t' l)r,'( l,,nrln.rlint
,( r rl)lron
lrophysiology
CIII I I CAI" I.LLNI,$S- LPaticrrts in critical care units have an increased incidence ofmyoPathy.
The same risk factors for critical-illness PolyneuroPathy are riskfactors for critical-illness myoPathy-bed rest with disuse,corticosteroid therapy, and paralytic agents.
rical findings Diffuse weakness and depressed reflexes is the most commonclinical presentation. Patients often have failure to wean quicklyfrom the ventilator.
Sensory symptoms are absent.
)oratory studies Routine labs are normal. CK and aldolase are tyPically elevated.
EMC show normal sensory conduction but compound motor actionpotentials are very small. Electrical stimulation of the motor nervesmay not activate the muscles.
Muscle biopsy shows necrosis in severe cases, atroPhy mostprominent of type 2 fibers in milder cases.
lmaging is normal and usually not needed.
agnosis Diagnosis is clinical, with weakness, hyporeflexia, hypotonia, andelevated muscle enzymes.
EMC can be supportive of the diagnosis.
Muscle biopsy is definitive, although it is not needed in mostpatients, because in the appropriate clinical settinS, supPortive care
is satisfactory for ruling out other diagnoses that would altermanaSement.
ial diagnosis Criticol illness polyneuropothy. Presents with diffuse weakness,hypotonia, and hyporeflexia. CIP is difficult to distinguish from ClM.
Sensory findings are identified in CIR but because there are fewsensory complaints, the diagnosis can be missed.
A/DP. Presents with weakness and areflexia, and can be ofincreased incidence around the time of a serious illness.
Rhobdomyolysrs. Can present with weakness and a myopathicpattern on EMc. CPK is extremely high, and there is risk for renalfailure.
Myosthenio. Can present as diffuse weakness that may initially beatiributed to CHF, DM, or some other medical illness.
Treatment is supportive. There is no intervention other than avoidingprecipitating events.
linical course Patients typically have improvement, but necrotizing damage to themuscles may not recover.
594 DISORDERS-NEUROMUSCULARDISORDERS-NEUROMUSCULAR 595

OVERVIEW OT INTECTTONS OT THE NERVOUS SYSTEM
Description lnfections are one of the cardinal mechanisms of neurologic discast'lnfections of the nervous system mainly include meningitis arrd
encephalitis.
Pathophysiology lnfections of the nervous system can be bacterial, viral, fungal,parasitic, or prion.
Viral syndromes are most common, with bacterial meningitis beingfairly common in busy emergency departments.
Methods ofinvolvement
lnclude:
Abscess
Meningitis
Encephalitis
Sepsis syndrome
Post infectious effects
lnfectious agentsaffecting thenervous system
lnclude:
Bacteria
Fungus
Virus
Parasite
Prion
Type of Infection Essentiol Feotures
Bacterialmeningitis
Fulminant meningitis with headache, nuchal rigidity, and fever.
Appears toxic.
Occurs in a normal host
Prominent leukocytosis in the cerebrospinal fluid (CSF)
Requires antibiotics for improvement
Viralmeningitis
. Subacute to acute meningitis with headache and some nuchal rigidity.May have fever.
. Mild to moderate lymphocytic pleocytosis in the CSF
Fungalmeningitis
. Subacute to chronic meningitis with any of headache, cranial nervepalsies, and cognitive changes. Meningeal signs often are absent.
. More common in immunocompromised host
. Mild to moderate lymphocytic pleocytosis in the CSF
. Antifungal treatment is required for improvement.
Viralencephalitis
. Acute to subacute encephalitis with headache, confusion, andsometimes fever
. Mild lymphocytic pleocytosis, with increased red cells with HSVencephalitis
. HSV encephalitis responds to antiviral aSents, but most viruses d() not.
!96 DISORDERS-INFECIIONS
()vurvicw ol lttlct:liotts ( )vr,r vir,w ol lrrlt,t liorrs
l-ssentiol feotures( ltrotrrr rlrrrrenting disease, often with myoclonusCSF rnay be normal, and specific testing for prion products is neededThere is no effective treatment.
SECONDARY EFFECTS OF INFECTIONS
lylx,(), lnlrr ll()n
l'rrln (.n( r';rlt,tlrlrs
trrfections of the nervous system can produce secondary effects in a number ";;;rarh.*'clude mass effect, edemi,.post infeitiouiirl"-rr";, syndromei, unJ.euiotogic, onsequences of sepsis syndrome.
'4ass effect and edema can deverop from infection and can produce damage to otherwiserrrinvolved neurons through .o-pl"*ion .rJl!.""a.rv ir.rr"riJ. - ve"'|u6! L,
t'ost infectious autoimmune syndromes incrude acute disseminated encepharomyeritis
^DEM), acute inrammatory d'emverin.ti;s p;il;;;p-.th'i i;i;;i, Jnti"i"i,,io,r,uo. rntlrese conditions, there are central o, purip'r,'r,iui'a".yerinating changes, respectivery.
Inmune deficiency associated with Hlv increases the incidence of neurologic disorders as
Most brain abscesses are bacterial, although fungi and parasites canproduce solid foci of infectron.. Abscess is diagnosed by biopsy, and treatment may include medicationwith or without resection, dep6'nJing-o;ih;';iioioly una tocation.
DISORDERS-INFECTIONS I97

( )vt'l'vit'w ol I ttltrt'l itltls t t,nnnu\l
Bacterial meningitis
lnflammation andsuppurative processon surface ofIeptomeningesof brain andspinal cord
\
\*
',yrrrplorrrs ol CNSrrrlr,r liotr
( linic<rl Scenorio
tr.vcr with headachervrthout otherrrttrel69i6 5;*nt
t ,'ver with confusion,,r focal signs or'.r'izure, with orrvrthout headache
tircal deficit withr r raging suggesting, r I rscess
t ,rnfusion in a
1',rtient with knownrr rr rn unodeficiency
l.vtrlrrtrliorr r)l SusJ,(,( l('(l ( NS lrrlt,t'liorr
I t'vr,r wrllr lrt'adache
Contusion of subacute onset
Development of seizures with mental status changes
Synopsis ond Approoch
Bacterial meningitis could cause this manifestation, although viralmeninSitis and noncentral nervous system (CNS) infections alsocan do this.
Neurologic evaluation usually is normal in this scenario.
ln the absence of signs of CNS dysfunction, blood testing, andurgent lumbar puncture (LP) can be done.
Meningitis, brain abscess, and encephalitis all can produce thispresentation.
LP should be delayed because of the risk for herniation if there ismass lesion. Therefore, emergent imaging with CT is indicated priorto LP. Antibiotics are given prior to the imaging, and, therefore,there is no delay in treatment.
LP is performed if the imaging is normal.
Patients being evaluated for an indication other than suspectedinfection may have a scan that suggests abscess. Magneticresonance imaging (MRl) and computed tomography (CT) are notspecific enough to make the differentiation of abscess vs. tumor;however, there are guidelines.
The urgency of evaluation is greater if the patient is thought to havt,potential for abscess, and biopsy usually is indicated if the lesion isat all accessible.
Direct effects of the immunodeficiency virus and opportunisticinfections have to be considered.
lmaging with CT or MRI usually is done first, because brain abscessis common, especially in patients with AIDS, where toxoplasmosispredominates.
Brain abscess
Y) airn\'I
I,v
q-Multiple abscessesof brain
[vAr.uAiloN oF suspr,('t l l) crNTRAi rvinvous svirel,t (cN$) rNFEcTroN
-{
a\-{. \,
598 DISORDERS-INFECIIONS DISORDERS-INFt( II( )N., tII

I vrtlttrf lf ()n ol Sttslrcr lr,rl ( N.\ lttlr,r lir tn ,,,ttttrttt,,t
Encephalitis. Viral or prion infection of
the brain. CT and MRI may show
regions of edema,enhancemenl
. LP may show mild elevationin protein, WBC, or RBC
. EEG often slow, withcharacteristic periodicpattern in HSV encephalitis
Prion encephalitis. MRI may give specilic
abnormalities. EEG often shows periodic
discharges. LP can be supportive
CNS infection suspected. Fever with headache, or. Altered mental status of subacute onsel. Seizures and altered mental status
. CT usually first
. MRI if possible
. Labs: CMP GBC, CRP, ANA, ESFI, blood cultures
. Echo: for suspected bacterial abscess
. LP: il no mass lesion for possible meningitis, encephalitis
. Brain biopsy: lor abscess and occasionally lor encephalitis
. lnlection oJ the CSF usuallyviral, may be bacterial orlungal
. Virat: CSF I WAC, I protein.
. Bacterial: CSF 1t WBC,t protein, J glucose
. Fungal..CAF T WBC,
J protein, may be J glucose
Herpes encephalitis. MRI often shows focal
temporal lesions. EEG may show periodic
discharges. LP may show positive
serology
Non-HSV viral encephalitis. MRI normal or multifocal
abnormality. LP may show mild-moderate
pleocytosis, mononuclear. EEG usually slow
. Focal or multifocal inlectionof the brain
. Cause is usually bacterialand related to sinus ordental disease. Cons,dercardiac emboli. Considerimmune disorder
. Abscess may be in spine.
. Specific entity determinedby surgery - aspiration,biopsy, or excision
Bacterial abscess. MRI/CT shows enhancing
lesion(s). Bacteria identified on biopsy
Fungal abscess. MRI/CT shows enhancing
lesion(s). Biopsy shows lungi
Parasitic abscess. MRYCT shows enhancing
lesion(s); often multiple. Biopsy makes the diagnosis
Meningitis
Bacterial meningitis. MRYCT normal or meningeal
enhancement. LP shows CSF leukocytosis;
glucose often reduced
Viral meningitis. MRYCT are normal. LP shows moderate
lymphocytic pleocytosis. Viral serologies may be
positive
Fungal meningitis. MRI may show meningealenhancement, may behydrocephalus
. LP shows fungal element andolten positive serology
4OO DISORDERS INFECTIONS DISORDERS-INFECTIONS 40I
,( Itl)ttoil
hophysiology
rr^cr!l1lryA b.rcterial infection of the spinal fluid
This is a serious infection with a fulminant course.
Strains of bacterial meningitis include:
Hoemoph il us i nfluenzoe
Streptoccus pneumonioe
Nerssezo meningitidis
Listerio monocytogenes
Medical conditions that predispose to meningitis include sinusitis,immune-deficiency states, skull fractures, or other reasons for skulldefects, such as neurosurgery. shunts, implanted stimulation andrecording electrodes, sickle cell disease, and splenectomy.
inical findings Headache, fever, and neck pain are common presenting symptoms.
|f;ental status changes often develop, ranging from confusion to
Seizures can develop.
Meningeal siSns commonly are commonly seen, in addition to theneck pain and stiffness.
boratory studies Routine labs show elevated white blood cells (WBCs) in mostpatients. C-reactive protein (CRP) may be elevated. The remainderof the labs is normal.
lmaging with MRI or CT usually is normal, although MRI may showmeningeal enhancement. Cerebral edema can be seen. Regions ofcerebritis also can be seen.
CSF shows a polymorphonuclear pleocytosis that is in thethousands, unless there is an immune deficit. Protein is oftenelevated and glucose is reduced. Very low glucose is a poorprognostic sign.
ldentification of the organism depends on microscopic examinationand culture of the CSF. Counter-immune electrophoresis (ClE) is a
rapid test performed on CSF that can identify the most commoncauses of bacterial meningitis; however, the identification must beconfirmed by culture.
aSnosrs Bacterial meningitis is suspected when a patient presentsemergently with fever, headache, and is found on exam to haveneck stiffness.
lmaging often is done to look for abscess, because LP should beavoided with cerebral mass lesions. This is especially important ifthe patient presents with mental status changes or seizures.
LP is the definitive test, and shows yellow cloudy fluid, usuallyunder increased pressure. Perfectly clear and colorless fluid arguesagainst bacterial meningitis even before analysis of the fluid. CIEcan suggest a specific organism, but is not definitive, and thereoccasionally are false positives. Microscopic examination can identifythe organism in some patients. Culture is definitive.
lirr lct irrl Mcttinr;ilts

Differential diagnosis
Management
littt'lt't'ittl Mt'rtirrt;itis,rrrli,rr,r/
BAC:[[&IAI. tr{tN ING lTl$--cont'd
. Brain obscess. Can present with fever and headache, and ftrc,rlsigns are not always present. lmaging is required for the diagrrosr.,
. Aseptic meningitis. Can present with headache and may beassociated with fever. The toxic appearance of most patients willrbacterial meningitis is not mirrored in most patients with asepti<meningitis. CSF analysis makes the diagnosis.
. Encephalitis. Can present with fever and headache, and somealteration of mental status or seizures is common. The meningealsigns seen with bacterial meningitis are not typical. CSF may showsome inflammatory change, but not to the degree of bacterialmeningitis.
Antibiotic treatment is begun as soon as the diagnosis of bacterialmeningitis is suspected. For best identification of the organism, theLP should be performed prior to start of antibiotics course; however,this is not always feasible. Patients who need an imaging study priorto LP should have antibiotics begin so that treatment is not delayed.The risk for administration of unneeded antibiotics is small incomparison to the risk of delay in treatment.
Most patients with bacterial meningitis improve, although this is notinvariable. Some patients will develop cerebral edema, herniation,and brain death despite prompt medical treatment. Others will be lcltwith neurologic deficits and/or seizures.
.,.."*" ",,1,' ,u;r-ln ne()nJles
, ;)'Cru.-n"gutive bacilli, 50%(E. coli, Klebsiellanneirrrrrrrriat:. etc.)
ii"...;"',,.,Streptoco( ci, 20'ilo
Other (5. aureus, Listeria monocytogenes, H. in{luenzae', etc.)
Mrlrl r orttrttott r.turalivt' org.tttistttsI I trllrt tt.,t,',,lrll ,,rrr.,r'r .", ,{)",, rrl
IrInIr),rlr', til rl('vr'lrlrtttli r ottttlti|s 1'){)')1,
rlrlrrr lrorr rn I I \ rvillt I lilr v,t r inr')
H. influenzae, 5Ook
" .1,"' "N. meningitidis,25ok
Other (listerla, etc.)
lkrr tct'ittl Murirtr;iti.s
Sources of infection
Pneumonia
Infection ofleptomeningesis usuallyhematogenous,but may bedirect fromparanasalsinuses, middleear, mastoidcells, or CSF
leak fromcribriformplate defector via dermalsinuses-
Basal skulliracture
Otitis mcdia
Mastoiditis
Dermalsi nuses
. r:!a
.l
ii
,. ", '.-r'.. S. pneumoniae, lOo,o
" "'i Cram-negative bacilli
Other (Usteda, etc.)
ln children
IB:i,.
h,*a
4O2 DISORDERS-INFECTIONS DISORDERS-INFECTIONS 4O5

lltrritt Alrsr css
BRAIN ABSCESS
Description Loculated infection of the brain
Most are due to bacteria, although fungal and parasitic infectionsalso can create abscesses
Pathophysiology The most common bacteria to produce brain abscesses include:
S. oureus
Streptococci
Enterobocter
Pseudomonos and other anaerobes
. Fungi and parasites form a small proportion of brain abscesses.
. Many brain abscesses develop from contiguous spread from sinusand other tissues. Neurosurgical procedures, skull defects, trauma,and other breaches of the skull increase the risk for brain abscess.
Clinical findings . Fever is present in patients, especially with bacterial abscesses. Thtfever may be mild and overlooked.
. Headache is common, and can be generalized or localized.
. Mental status changes can include confusion, lethargy, and evencoma if severe.
. Seizures can develop.
. Focal signs can include hemiparesis, hemianopia, frontal lobedef icits, aphasia, neglect.
. Onset of the symptoms is within days to a few weeks, dependingon the organism.
Laboratory studies . Routine labs are normal, but peripheral WBC usually is elevated.CRP and erythrocyte sedimentation rate (ESR) also are commonlyelevated.
. lmaging is normal, except for MRl, which occasionally may showenhancement of the meninges.
. LP usually is not done when brain abscess is suspected; however,performed it has a polymorphonuclear pleocytosis with elevatedprotein, but normal glucose. Organisms typically do not grow outthe CSF.
. Brain biopsy can reveal the organism on microscopic examination.Culture is needed for confirmation of the precise organism.
Diagnosis . Brain abscess is suspected when a patient presents with fever andfocal neurologic deficits or seizures.
. lmaging shows an enhancing lesion that may have the radiographiappearance of an abscess; however, biopsy is needed to make thedefinitive diagnosis of abscess.
Differential diagnosis Bocteriol meningitis. Presents with headache and fever, and inpatients who develop meningoencephalitis, there may be cognichanges and seizures. lmaging can make the differentiation.
Broin tumor. Can present with headache and focal findings onexam or seizures. Cognitive changes are common. There are nooutward signs of infection in these patients, and while imagingcannot be definitive about etiology, biopsy can.
404 DISORDERS INFECTIONS
cognrtrve
DISORDERS-INFECTIONS 405
M.rrt,rgr.ntt,rtt
i linical course
llrrrirt Alrscr,ss
Appropriate antimicrobial therapy for the eradication of theorganism is needed. Before tissue is obtained, broad spectrumantibiotics with good CSF penetrance are given, followed by moredirected therapy when an organism has been isolated andcharacterized.
Surgical resection of a brain abscess depends on the individualclinical situation. An accessible lesion in a patient with mass lesionof unknown etiology most likely needs, at the least, surgical biopsy.Total resection of a brain abscess usually is not needed, and,furthermore, can leave the patient with extended deficit.
Most patients improve, although abscess in patients with immunedeficiency can be the opening of a variety of immune attacks.

llt<titt Allst t'ss trrttr,rrrrt
Brain abscess
\
\
Paramening,eal I n fecl iorrs
l/r
Scar oi healed brain abscess wilhcollapse oi brain tissue into cavity
\LF--
Subdural abscess
r ,.,,.il !.,,1r".
't'
Ostcomyelitis of sl<ull, withpenetration of dura to formsubdural "collar button" absr:ess
CT scan shows brain abscesswith thin enhancinpl rim andccntral necrosis
---{-,*' }T
\{*rn-,1';,, Muiriprr',,b\(e\\es-t ,"f ''r. / y ut lrrrin
406 DISORDERS-INFECTIONS DISORDERS-INFECTIONS 407
I )r
I'
Spittttl l.ptrlrrrtrl Al)s( (,ss
r(,\( ill)lt()n
, rtIropltysiology
sl,tNAt, ltl,ll.)URAL A$lictss
A lr,rr lcr,rl rrl't.tion in the spinal canal, but outside of the dura
. Sprrral cpidural abscess usually develops from extension fromsurrounding tissues. Discitis is one potential cause. With time, theinfection can migrate into the adjacent epidural space. Any form ofspinal procedure or injury also can predispose to epidural infection,including spine surgery lumbar puncture, and local spine trauma.Local skin infection also can predispose to infection. This is also ofincreased incidence in bacterial endocarditis.
. Bacteria involved in epidural spinal abscess include StophylococcussPecres.
linical findings . Patients usually present with pain in the back, which may alsomanifest erythema, swelling, and warmth suggestive of localinfection; however, these findings are not always present. Radiationof the pain in a root distribution is common.
. Exam shows normal function if there is no compression of the cordor cauda equina. Rapidly expanding mass effect of the abscess canproduce myelopathy or cauda equina syndrome, depending on thelevel of the lesion.
ratory studies Routine Iabs show signs of infection with elevated blood WBC, ESR,and CRP.
Blood cultures commonly are done, with suspected spinal epiduralabscess to look for bacterial endocarditis.
lmaging urgently is performed when spinal epidural abscess isconsidered. MRI is most sensitive, but may miss a small developinginfection. Contrast-enhanced MRI is most sensitive. CT is much lesssensitive. Myelography can show the lesion, but the LP required forthis procedure should be avoided if this diagnosis is suspected.
LP usually is not done, but if CSF is obtained, it shows mild-to-moderate pleocytosis with elevated protein. Glucose is normal.
Culture of the abscess gives definitive identification of the organism.
Spinal epidural abscess is suspected when a patient presents withback pain and has fever or other signs of infection. A history ofspinal surgery skin infection, or risk factors for SBE increases thelevel of suspicion.
Urgent MRI is the procedure of choice for demonstrating theabscess. Contrast-enhanced MRI is most sensitive, and mustspecifically be requested, because most routine spine studies donot use contrast dye.
Surgical exploration and drainage is not only therapeutic, but alsoprovides substance for microscopic exam and culture.
ial diagnosis Meningitis. Can present with spine pain and signs of infection, butthe spine pain is less well localized and headache typicallypredominates over the spine pain.
Discitis. lnfection of the disc space. Many of the same conditionsthat predispose to spinal epidural abscess can predispose to discitis.Differentiation rests on MRl.
Extrospinol infection. Can produce severe pain in the spine withsigns of infection.
/raSnosls
I 'ifferent

m Splnol Epldurol Abscess conrnued
. Treatment begins with urgent administration of antibiotics when thodiagnosis is suspected.
. Surgical exploration and drainage of the abscess is the definitivetreatment. Cultures and smears may alter the choice of antibiotics.
development of severe neurologic deficit, and, therefore, treatmentof the abscess usually can halt the progression of symptoms.lmmunocompromised hosts may present a challenge to antibiotictreatment.
. lf spinal cord or cauda equina compression has resulted inneurologic deficit at the time of diagnosis, then residual weaknessand ataxia is common.
Splnol Epldurol Abscess m
a t. t7!',
Abscess in epidural spacecompressing spinal cordand its blood supply
Pain on percussion of spine.Local warmth may be noted
Epidural abscess
Fat in epidural space
Arachnoid
Anteriorartery
Dura
Posterior spinal arteries
:
,l
Clinical course
408 DISORDERS-INFECTIONS DISORDERS-INFECIIONS 409

Sr'ptir I luotttlropltlclrilis
SEPTIC THROMBOPHLEBITIS
Description lnfections of the sinuses can predispose to septic thronrbosis ol llrr'intracranial veins. The clinical manifestations differ dependirtg orr
which sinuses are affected.
Pathophysiology . lnfection of the ear and sinuses, including paranasal and mastoirl,can result in venous thrombosis with resultant impairment in
venous drainage.
. lnfectious occlusion of intracranial veins also can occur from othcrintracranial and cranial infections.
. Occlusion can be of the cavernous sinus, lateral sinus, or sagittalsinuses.
. Findings can be due to increased intracranial Pressure or venousinfarction.
Clinical findings - Patients can present with combinations of fever, headache, altere<l
mental status, or focal symPtoms.
. Exam may show papilledema; focal deficits, including weakness(although this usually is not complete); hemiparesis; or seizures.
. Lateral sinus or sagittal sinus thrombosis can produce features ofincreased intracranial pressure with headache and papilledema.
. Cavernous sinus thrombosis can produce orbital swelling andinjection, often with cranial nerve palsies. Any ocular motor nerves
can be affected, resulting in diplopia. lnvolvement of the firstdivision of the trigeminal nerve (V,) can produce pain and sensorydeficit on the forehead, extending to the vertex.
. Signs of ear or sinus infection may be evident.
Laboratory studies Routine labs may show elevated WBC, ESR, and/or CRB but this isnot invariable.
lmaging with CT or MRI may show the inflammatory changes in thtear,-maltoid, and/or paranasal sinuses. MRI additionally may showvenous infarctions in the brain, which can be multiple and smallerthan most arterial cortical infarcts.
MRV or CTA can show lack of flow in the venous sinuses, andsometimes a clot even can be seen. There is significant variability ir'
venous anatomy, so hypoplasia or aplasia should be differentiatedfrom thrombosis.
LP sometimes is performed in patients with venous sinusthrombosis; however, there are some individuals who will have LP
performed when bacterial meningitis is considered in the diagnosisin these patients, there will be increased intracranial pressure andoften a lymphocytic pleocytosis.
Diagnosis Septic thrombophlebitis is considered when.a patient presents withheadache and signs of increased intracranial Pressure. Presence ofthe signs of infection supPorts the diagnosis.
Differential diagnosis Meningitis. Can produce headache and signs o{ infection. and also
is a polential consequence of sinus and ear infection'
Broin abscess. Can present with similar symPtoms, but imagingshows enhancing lesion rather than venous infarction and venousocclusive disease.
4I O DISORDERS-INFECTIONS DISORDERS-INFECTIONS 4I I
Sl:l' I l(. I IInOMIIOPHLEBITIS*cont'd
l\,4, r r. rll('l r t(,nt
' lrrrical course
I r latcral proptosls, conjunctiva I
lrcmosis, and ophthalmoplegia
Involvement of cranialncrves (lll, lV V, and VI)results in ophthalmoplegiaand facial analgesia.
Trochlear n. (lV)
Network of v;rivclr,,,,,veins allows nri!1,r1 roloi septic thronrlri lrorrr
sinus or orbil sit, .to cavernous sirlr.,
Sr,plir I lrrorrrlroplrltlrllls
Arrlrlrrolrrs ,rrc used for intracranial thrombophlebitis. lrrili,rl lrro,rrlsl)('(trurn therapy can be focused when an organism andsensitivities are known.
Anticoagulation often is often used, although there is some risl< lorfacilitating intracranial hemorrhage.
Surgical treatment of the sinusitis or ear infection may be ultirrr,rtr,lyneeded.
Most patients improve, although there is the possibility of incrtast'rlintracranial pressure to the point that there is decreased brain-perfusion pressure.
lntracranial Complications
Cavernous sinus thrombosis
'-4rffie
,l! :l
tSeDti.thJombosi. \,1n cavernoussinus
Jssi{ &,,*&,e\;ao
Communicationbetween cavernoussinuses results inbilateral disease
M, ;l'1,'r'
H'i#*',:;,ffi

I trrrr;trl Mr,rrirrr;itis
TUNGAL MENINGITIS
Description lnfection of the meninges is an uncommon cause of norrb,r<lcrr,rlmeningitis.
Pathophysiology . Cryptococcus is the most common organism to cause fungalmeningitis, although Candido and Aspergillus, as well as someothers, can.
. Fungal meningitis rarely is seen in immunocompetent hosts;patients with AIDS are particularly susceptible to cryptococcalmeningitis.
Clinical findings . Patients present with any combination of headache, confusion,visual difficulty, or ataxia. Fever may be present, but is an inconst,rrfeature.
. Meningeal signs commonly are not seen.
. Exam may show confusion, ataxia, or papilledema.
Laboratory studies . Routine labs usually are normal, although there may be signs ofim m unodeficiency.
. lmaging with CT and MRI usually is normal. Contrast-enhanced MRsometimes may show meningeal enhancement. Hydrocephalus mirbe seen on either imaging modaliry and contributes to symptomsand signs.
. LP shows increased CSF pressure, lymphocytic pleocytosis with,I00-300 cells. Protein commonly is increased and glucose may be
reduced.
. Cryptococcal antigen is a rapid test for screening CSF forcryptococcal meningitis. Although therapy can be initiated on thebasis of these results, final diagnosis depends on cultures.
. Fungal cultures make the definitive diagnosis of all fungalmeningitides.
Diagnosis . Fungal meningitis is suspected in patients with headache andconfusion, although the differential diagnosis is large.
. lmaging is performed to look for mass lesions or subarachnoidhemorrhage; in fungal meningitis imaging may be normal or showenhancing meninges. Hydrocephalus is present in a smallproportion of patients.
. CSF analysis is confirmatory with the typical profile described abovCryptococcal antigen is positive in most patients with cryptococcalmeningitis. Fungal culture is the definitive diagnostic study.
Differential diagnosis . Bocteriol meningitis. Has a more fulminant course than fungalmeningitis. The CSF profile differs substantially.
. Normol pressure hydrocepholus. Presents with ataxia, dementia,and, often, urinary incontinence, with imaging showingcommunicating hydrocephalus. However, this especially is seen inelderly patients. CSF is normal with NPH.
. Encepholitis. Presents with headache, confusion, and often ataxia.lmaging also may be normal. CSF can even look similar, and,therefore, specific antigen assays and cultures for fungi are done I
help with the differentiation.
4I2 DISORDERS_INFECTIONS DISORDERS-INFECTIONS 4I 5
I rrrrr;rrl Mr,rrin(lilis
aI \Ji;
tt, t /
ln{ection is by respiratory r()utc.I'igeon dung and air conditionersrnav lre factors in dissemination.
India ink proparation Accumulation of encapsulated.hou inH Irudding .rnd 1 ryploq or r i in .ubarat hnuid \n.r( er Jpsule IPAS rrr melhen,rmine-silrer.l,rirr,
I tIN( ;AT. MENINGITIS_<ont,d
Arrlrltrrrg.rl trcatment depends on the agent and host factors.Arrrl->hotericin, flucytosine, and fluconazole are commonly usedaBents.
Prognosis is generally good if the host has adequate immuneresponse to the infection. Patients with few CSF WBCs have a pooreroutcome because they lack the robust immune response that is
required along with the antifungal treatment.
Cryptococcosis

VIRAL MENINGITIS
Description Viruses can easily invade the meninges, producing an acutemeningitis that can be difficult to distinguish from bacterialmeningitis.
Pathophysiology . A host of viruses can produce viral meningitis, includingenteroviruses, HSV2, CMV EBV LCM, HIV and adenoviruses.
. HSV2 is more likely to cause meningitis than encephalitis, wherthe reverse is true for HSVI, which is more likely to causeencephalitis.
Clinical findings . Patients present with headache and fever, often with neck pain.Confusion and seizures are not expected, and when present theyindicate meningoencephalitis.
. Neurologic exam often shows meningeal signs. Neck stiffness iscommon, although the severity of meningeal signs is not what isseen with bacterial meningitis.
Laboratory studies . Routine labs are normal.
. lmaging is normal. Usually, there is insufficient meningealinflammation to be seen on MRl.
. LP most commonly shows a lymphocytic pleocytosis in the CSF,usually less than 100 cells, although several hundred cells can beseen. Thousands of cells suggest bacterial infection. protein may Ielevated, but glucose is normal.
. Specific titers for certain viruses can be performed. Culturing CSFviruses has an extremely low yield.
Diagnosis . Viral meningitis is suspected in a patient with headache and ferespecially in the absence of other signs of infection.
. lmaging usually is performed to look for abscess.
. LP is definitive for meningitis. The lower WBC, lymphocyticp_redominance, and absence of bacterial antigens argue-in favorviral meningitis.
Differential diagnosis . Brain obscess.,Can present with fever and headache, although fosigns commonly are seen. lmaging makes the differentiationl
. Bocteriol meningitis. Can present similarly to viral meningitis,alth-ough the onset is more fulminant with bacterial meningitis. Cprofile is different, with greater WBC and a polymorphonuclearpredominance.
. Fungol meningitis. Especially with Cryptococcus, it produces asyndrome. of aseptic meningitis, which only reveals the organismwith special testing. The CSF formula can look very similar.
Management . There are no treatments for most viruses.. HSV can be treated with acyclovir.
Clinical course Most patients improve, and in general, the prognosis is better formeningitis than for encephalitis.
Vilrrl Mt'rrin(,itisi
br'
for
fever.
rol
foc.rl
CSI
4I4 DISORDERS-INFECTIONS
vinrl
DISORDERS-INFECTIONS 4T5
,** Wts'
CSF shows lymphatic pleocytosis (usually < 100 cells) andprotein may be elcvated but glucose is normal.
Vtrrrl Mcrtilr(lrlis

l t rr r,plrr rlrl rs
ENCEPHALITIS
Description A diffuse infection of the brain. Most are viral, although r(rr(. (,rs(.., (
bacterial encephalitis can develop.
Pathophysiology Viruses are the most common cause of encephalitis, with a widt,range.of .possible pathogens. Herpes encephalitis is a prototypirencephalitis, important to diagnose because it is treatable.
Bacterial encephalitis is uncommon, and is most likely related toSBE. ln some patients with SBE, the bacteria produce extensivecerebral and meningeal inflammation withoui forming definedabscesses,
Cancers can be associated with a paraneoplastic encephalitis. Thisautoimmune, and a remote effect of the cancer.
Clinical findings . Encephalitis presents with rapid onset of confusion, often withheadache. Fever is seen in some forms of encephalitis, but not all.
. Focal neurologic signs may develop, especially with encephalitisthat produces. necrotizing changes, especially HSV. Hemiparesisand/or aphasta are common.
. Seizures can develop with any encephalitis, especially HSV
Laboratory studies . Routine labs commonly are normal, although elevated blood WBCis sometimes seen. This is much less common with viral thanbacterial infections.
. lmaging can show diffuse or multifocal regions of edema andenhancement. HSV encephalitis shows chinges most prominent inthe temporal areas.
. LP shows inflammatory changes in most patients, indicating thatthis is commonly a meningoencephalitis. The CSF profile differsdepending on the type of encephalitis
. Electroence.phalogram (EEG) shows slowing and disorganization ofthe record in most patients, consistent with encephalo--pathy.However, many patients with HSV encephalitis will have periodicdischarges in the temporal regions.
Diagnosis . Ence_phalitis is suspected when a patient presents with fever,headache, and confusion. The addition of'focal neurologic findingsand seizures supports the diagnosis and is most often seen with"HSV.
. lmaging is performed which may show focal or multifocalinflamm.atory changes. Predominant involvement of the temporallobes with necrosis suggests HSV.
. CSF analysis shows a profile similar to aseptic meningitis withIymphocytic pleocytosis and elevated protein. The ele"vation in WBCis moderate.
. Rapid.testing for HSV by polymerase chain reaction (pCR) is nowavailable. West Nile virus (WNV) also is testable from the'serum anrCSF.
. plood tests for many forms of encephalitis are now available,including,st, Louis, California, eastein equine, and western equineencephalitides.
4T6 DISORDERS-INFECTIONS
nd
DISORDERS-INFECTIONS 4T7
I trIIcrt,rrli,rI tlr,r1irro,,r,,
\.,4dnagement
!inical course
l.rrr r,plrrrlilis
llrttrrr <tbscess. Can present with confusion, seizures, and focalrrt'urologic signs. lmaging shows a defined abscess. lmaging givesdifferent results, with focal abscess formation rather than cerebritis.
Meningitis. Can present with conlusion and seizures, although inthis case, some cerebritis is implied.
. Management of most patients with encephalitis is supportive.Routine medical manaSement for seizures and cerebral edema, aswell as fluid and nutritional support, are needed.
. HSV encephalitis is treated with intravenous acyclovir. Treatment isbegun as soon as the diagnosis is suspected, because treatmentshould not await the results of the HSV-PCR testing. Therefore,many patients are begun on treatment lor HSV who will notultimately be maintained on treatment when the labs return.Because MRI and EEC cannot definitively distinguish HSV fromother meningitides, treatment of many encephalitis patients is
needed.
Most patients improve, though not all. Patients with necrotizing HSVencephalitis are often left with neurologic deficits including aphasia,focal weakness, and/or seizures.
Patients with WNV and many of the other encephalitides also canhave neurologic deficit, with damage from edema or secondaryinfarction.

l .t tt r'; rl tr r l r l is , ,,,ttlrtt tt
Lumbar puncture toranalysis of CSF viralDNA, cytology, andchem istrics
Clinical Fc.rlurcs of HSV trrtt.ph.rlitis
Tl pir ,rl io,rturr'. ' )l ,r ut, , )n\, t , 'lfcvcr, headacht:, mcntal st.ttus, andbehavior changcs rvith or withoulfocal signs Ior:alizing to temporal lobr:,dvsph.r'ra .rnd hiz.rrre hlh,r\ i, 'r mJ)localizr:)
Seizure activity is
common, often rvithinI week of initialsymptoms.
MRI domonstratingtemporal lobe involvcmcnlis a diagnostic cornerstonc
PCR amplification of HSVDNA from cerebrospinalfluid provides majordiagnostic i nformationand is vcry sensitive.
HSV enccphalitis CSFcytology and chemicalstudies typical ly show:WBC: moderateRUC: +/Protein: modcrateClur:osc: normal
;**-. ','+';'[*'"' '' t' t' t';fh,.l &.Si?&l{i**n'l$? W.eit{e{e
''
l rff
,ld
,( rrl)lr()n
lrophysiology
l,Rt()N DIti[Al_
( lrronrr rrcurologic disorders producing mainly cognitive and motor,,u,t,,,trt, *- Prions are proteins that alter native proteins to produce cellular
degeneration.
- Prion diseases can be transmitted or inherited, because bothmechanisms can result in the abnormal prion proteins, whichproduce the disease.
. The incubation period can be many years for prion diseases. Modesof transmission have included surgical procedures, such as braininstrumentation and corneal transplants, and ingestion of infectedmeat. Modern methods of handling and surveillance reduce thechance of prion transmission in foods, but safety cannot beensured.
rrical findings CreutzfeldtJakob disease (CJD) is the prototypic disorder. Patientspresent with rapidly progressive dementia, ataxia, myoclonus, andexaggerated startle.
This is termed myoclonic encephalopathy, which has a limiteddifferential diagnosis in an adult.
)oratory studies Routine labs are normal.
Imaging with MRI may show changes in the basal ganglia,particularly the globus pallidus and putamen, in patients with CJD.
CSF is normal. I4-3-3 protein and neuron-specific enolase havetraditionally been assayed, but these are not helpful in solidifyingthe diagnosis. Assay of the PrP gene is more definitive.
EEC commonly shows slowing and disorganization of thebackground; however, periodic discharges can be seen in CJD thatsuggest and support the diagnosis; these findings are not Presentthroughout the course of the disease.
agnosis Diagnosis of prion diseases is considered in patients with myoclonicencephalopathy. However, the myoclonus is not prominent in allcases, and in some forms of prion diseases, coSnitive dysfunction is
Iate. Therefore, suspicion is raised when a combination of cerebellarand corticospinal tract dysfunction develops.
erential diagnosis . Multiple sclerosis. Can present with multifocal signs with cerebellarand corticospinal tract dysfunction. MRI and CSF can distinguish thisfrom CJD.
. Vosculitis. Can present with multifocal CNS findings. MRI and labstudies can distinguish these possibilities.
nagement Treatment is supportive. Although medications have been tried, nonehave proven to alter the course of the disorder.
nical course Prion diseases are progressrve.
l't'iort I)iscrtsr,s
4I8 DISORDERS-INFECTIONSDISORDERS-INFECTIONS 4I9

Speciflc PrionDiseose Feotures
CreutzfeldtJakobdisease (CJD)
. Prototypic prion disease, presents with encephalopathy, ollcn wrrmyoclonus.
. Diagnosed by biopsy, although immunoassay of the PrP gives slrtindication of diagnosis.
Gerstman-Straussler-Scheinker (CSS)
- Autosomal dominant form of prion disease
. Patients present with progressive ataxia and dementia, whichprogresses to death within a few years.
New variant CJD(nvOD)
. Thought to be caused by the same agent that causes bovinespongiform encephalopathy (BSE)
. Patients present with progressive dementia, which is oftenpreceded by psychiatric disturbances and sensory complaints.
. Patients with nvCJD are younger than patients with CJD. Mostpatients were in the United Kingdom, or at least were residing inthe United Kingdom during the period of susceptibility to infectior
Fatal familialinsomnia
Patients present with insomnia plus other neurologicmanifestations, including autonomic dysfunction, motor deficits,dementia. The presentation is variable, and all patients do notdevelop all symptoms.
Patients progress to death within a few years.
Genotypic analysis makes the diagnosis.
l't itrlt I )ist,rtst,s tt,tlt,ttu.tt
Denrentccl paticntcrhibiting myoclonus
. r , \r1 llrlll lr,)m l)Ul.r'il('llt . .t
,.. .h,,rrirrH*tlcn'rrr'1"..t' r,l ttcurrrl. JnLl .l)iltrqtl{,tm
a-' . t]"
lrr.rin,li.',ur,. t1,irr,r) , ',rrl;' .t.u,rll\ .hrrr. rirril.rr
all(l
Transmissible Spongiform EncephalopathyCreutzfeldtlakob disease
II ." ". * g loss of nrotor neurons.
-i" 1 *i! q,,:
Fp 1 l .l 1,1,r ij"'r-r: r.,r"ir'ilr.li ",'1i,/"'-r'r"',Fp2 F,l 1-',";.i r,.1,",;' l, ,,1'',i'.1'r'i; ;, j. ',
F3-C3 I '\' ,., .r ,, .,', .' ." 'fF4-C,+ ",1,
.;,., -:.1r,, \ii,, s1.. ;';-r1; ,,'r -',.. "1, .C3-P3 ,1 ,',. !r'f - {. ,1 i,']\ .^- .4, ".. i.",i. "1 ,1
p:l O l,rr.-.:i*.,a /;- l,^ ";,--1'"r,",.r,.-r' .!^..\ ..--r.'. .
Pzl-O2 /vv,,,-,.r.r/- "i/\"?--\r^"\iaJ--\,-r,r *-;-aj-\
_-_-.j 75 pV1 scc
;1...c
,t
Et:Ci sholvingcharacteristicdiffusc pcriodicw.rvar p.rttern
420 DISORDERS-INFECTIONS DISORDERS-INFECTIONS 42I
.,,( ill)lt()n
llrophysiology
ilr,MAN rMYy
/\s llrr,r.rusative agent for AIDS, HIV has tremendous direct andirrdirect effects on the nervous system. Neurologic effects are related,yet supplement, the systemic non-neurologic effects of the virus.
HIV is a retrovirus that mainly is passed through sharing of bodyfluids from sexual intercourse, blood transfusion, transplantation,and other significant fluid or tissue exposure.
HIV causes immune deficiency that predisposes to a number ofopportunistic infections.
HIV also has direct effects on the nervous system, including AIDS-dementia.
nical findings Clinical presentation depends on the specific entity, discussed below,
Disorder Feotures
)5-dementia Progressive dementia develops due to the virus, itself, rather thanan indirect by opportunistic organism.
Treatment is supportive. Medications commonly used forAlzheimer's disease are tried, but efficacy is unproved.
xoplasmosis Toxoplosma gondii is a protozoa that is almost exclusively seen inpatients with immune deficiency. When a patient with AIDSpresents with mass lesion, tumor is possible, butToxoplosma ismore likely. lmmunocompetent individuals have asymptomaticinfection.
MRI or CT shows multifocal enhancing lesions.
Toxoplasma serology is confirmatory in the appropriate clinicalsetting.
Treatment is successful for most patients with sulfadiazine andpyrimethamine, although sustained treatment is needed for manypatients.
Lymphoma The main disorder in the differential diagnosis of patients withmultifocal lesions in a patient with AIDS. The lesions are focal ormultifocal.
Lymphomatous meningitis can be seen with symptoms separatefrom parenchymal CNS lymphoma.
CSF shows a lymphocytic pleocytosis and sometimes positivecytology.
Treatment is with radiotherapy and chemotherapy, but response istypically incomplete.
oSressrveultifocal: koencepha lopathyML)
An opportunistic infection caused by the JC virus. Before thedevelopment of AIDS, PML mainly was seen in cancer patients,particularly those with lymphomas and leukemias and otherdisorders with immune suppression.
Demyelinating changes in the brain are focal or multifocal, and canbe cerebral, cerebellar, and/or brainstem.
Aggressive retroviral treatment of AIDS patients can result in someimprovement; otherwise, there is no effective treatment.
NS
I ltttttrur llnnurn()(l('lr( ir,rrr y Virrrs
ukoencephalopa,ML)

Disorder feotures
Cryptococcalmeningitis
. Seldom seen in immunocompetent hosts
. Treated successfully with antifungal agents in most patients,although those with markedly impaired immune response havt'poorer outcome.
Polyneuropathy . Has varying manifestations in AIDS patients. A painful sensoryneuropathy is common.
. lmmune mediated neuropathy is commonly seen, resembling Alor clDP.
. Herpes zoster is common.
. Cytomegalovirus polyradiculitis can be seen.
Myopathy lnflammatory myopathy equivalent to polymyositis can be seen.
Degenerative myopathies are seen.
I ltttttrttt lttttttttttork'lit icttr y Vit'ltS,,,rrr,,r,,/ ()vctvicw ol Nt,ttto ottrolor;y
(,vr.RVr t]w or NtuRo"oNcotocY
N,'o1rl,rsi,r is one of the prime methods of neurologic disease.
Neoplasms can be benign or malignant, have direct or indirecteffects.
Local effects of neoplasms include tumor infiltration andcompression. Remote effects include paraneoplastic syndromes.
Benign and malignant tumors can all have compressive effects.Remote effects are only seen with malignant tumors.
Local effects of neoplasia are suspected when a patient presentswith clinical findings of a mass lesion of the brain or spine.
Remote effects of neoplasia are suspected when a patientpresents with encephalopathy, ataxia, or weakness in the absenceof local tumor identified as cause of these findings-paraneoplastic syndromes.
Asepl ic ----------1 7- Photophobiameningitis
\ /Headache-------
- -l /:.:;," ,/ / :;i",".* /
/ ,, Pharvngitis-
/ ,,PharvngitisLYmPhadenoPathY'
//
*";i:;;:",
Clinical Course and Features
Monlhsoost-infection YearsT-------\
Blood test for ELISA and Western blot, alsorecommended: CBC with differential, C6PD, hepatitis {
and hepatitis B serologies, liver and renal function,VDRL or RPR, and platelet count
Predisposing Conditions
Shared /'needles ,-HIV Yi
Multiplesexualpartners to blood
products
I )r..,( ill,lt()n
t',rthophysiology
, linical features
rr:oplostic Syndrome
t erebellar tumor
feotures
. Features of brain tumor include headache, papilledema,he.miparesis, aphasia with dominant hemisphere lesion, andlorsetzures.
. Aggressive molignont tumors arc more likely to present withneurologic deficit.
. Benign ond low-grode molignont tumorc arc more likely topresent with seizures.
. Primory broin tumors are more likely to be solitary.
. Metostatic tumors are more likely multifocal and usually have aknown history of cancer, although brain "mets" can occasionally lr,'the presenting sign of the cancer.
. Benign introporenchymol tumors usually are astrocytomas.
. Benign extro-oxiol tumors usually are meningiomas.
. Molignont primory tumors usually are gliomas.
. Malignont metostotic tumors can be from anywhere, but are moslcommonly from lung, breast, gastrointestinal (Gl) causes,melanoma, or lymphoma.
Produces ataxia, which can affect gait and limbs. Brainsteminvolvement from direct extension or compression can producediplopia with upper stem involvement, dysarthria, dysphagia witlrlower stem involvement, hemiparesis or quadriparesis withcompression of the corticospinal tracts at any level.
Most common in children, especially cystic astrocytoma.Cerebellopontine angle lesion includes acoustic neuroma an<lmenrnSroma.
/t/
'"/ /-\
"W'
Acute symptoms are often nonspecific,mimicking mononucleosis and otherviral illnesses
,,,d/
/
ii:,:l''*^5-*
Months post-infection
422 DISORDERS-INFECTIONS DISORDFR,, Nlr )t,t ,\ r, I ,!, r

Neoplostic Syndrome Feotures
Spinal cord tumor Presents with pain at the level of the mass lesion. Weakrressbelow the level is expected, with spasticity if the corticospinal tr,ris affected. Lumbar spine lesions affecting the conus medullarisand cauda equina produce flaccid paraparesis and sphincterdisturbance.
Extro-oxiol spinol cord tumorc can be benign or malignant. Beniginclude meningioma and neurofibroma. Malignant can be fromextension from adjacent spine, include lung, breast, ovarian, ren,ror other malignant tumor. Lymphoma can produce compressionwithout destruction of adjacent tissue.
lntromedullory tumors include astrocytoma and ependymoma.Metastatic intramedullary tumors are not expected.
Neoplastic meningitis Can present with pain and neurologic deficit in the distribution c
multiple cranial and spinal nerves. Diplopia, sensory disturbancewith pain, weakness, and signs of increased intracranial pressurewith headache, nausea, and vomiting is common.
Always malignant. Some common tumors to cause this are lung,breast, and Gl.
Paraneoplasticsyndrome
. Systemic symptoms not associated with structural lesion in apatient with known cancer suggests paraneoplastic syndrome.
. Limbic encepholitis often is due to small cell lung cancer. andpresents with cognitive changes.
. Peripherol neuropathy can be due to small cell lung cancer,breast, or ovarian cancer.
. Myosthenio can be related to thymoma or, less likely, lung car
( )vt't'vit'w ()l N('ttl'() ()tl( ()l(xry tttttrrtt.,t ( )vr,r'vir,w ()l N(,ur'() ()tl( ()l()(,y
\orrrr' ( ()lrrn()rr Marrifcslaliorrs rlI lJrain TumorsA. lrrlr.tr r,uri.rl lrrtssrrrl lrr.rrl
I lrrrl,tt lrt'irnay bcfrorttal,parietal, oroccipita l)
Nauseaand/orvomiting
t -,'.t
.L \.
Benigr r
'om. ren.rl
Papilledema
ol Il. various focal manifestations
Bitemporal hemianopsia
.,.rr.l
.g"tr,*""*6ffi Disorders ofmentation,speech, or
Personal itY'r,
U
rd.,
j Reflex.,rr abnormalities1..., , (Babinski sien)
:
I .--
.t \Jr;/t.l/
424 DISORDERS-NEOPLASMS DISORDERS-NEOPLASMS 425

I'tttttrtty lltrritt Ilurrors
.ts oltypc
:fici.r I
which
PBTMARY BRAIN TUMORS
Description Can be malignant or benign. Tumors produce symptoms rn,rirrly lrymass effect and destruction of functioning brain tissue.
Pathophysiology Primary brain tumors can be of several causes. Exposure to radi.rlrrand genetic predisposition is responsible for some of tumors.
The most important primary brain tumors are: astrocytoma,oligodendroglioma, glioblastoma, lymphoma, meningioma,neurofibroma, and primitive neuroectodermal tumor (PNET).
Clinical findings . Patients with brain tumors can present with any combination ofheadache, nausea/vomiting, mental status changes, focal weaknesspapilledema, andlor seizures.
. Patients with malignant tumors are more likely to have focal deficitPatients with benign tumors are more likely to have seizures,although these generalizations are not always correct.
Laboratory studies Routine labs usually are normal. Syndrome of inappropriateantidiuretic hormone (SIADH) is occasionally seen, and may produrelectrolyte abnormalities.
lmaging identifies a solitary mass lesion in most patients withprimary brain tumors. lmaging features can usually differentiatebetween tumor and infection. Also, differentiation betweenmalignant and benign can be suggested.
Definitive diagnosis depends on pathologic evaluation, which isperformed on biopsy or resection.
Management . Management depends on many features, including age and status (
the patient, location and geometry of the lesion, and presumed typ,of lesion.
. Resection is performed if possible. lf not, then debulking is beneficifor most tumors. Biopsy is performed if surgical resection would bedevastating. Central nervous system (CNS) lymphoma is oftensensitive to radiation and medical therapy so if this is identified onfrozen section, then resection is not performed. Resection can curesome lesions, especially benign tumors such as meningiomas.
. Chemotherapy and/or radiation therapy is performed for somepatients with malignant tumors. Unfortunately most malignantgliomas do not respond well to these treatments. PNETs and CNSlymphoma can respond quite well.
Specific Tumors Feotures
Astrocytoma . Tumors of astrocytic origin can be benign or malignant. Of themalignant tumors, anaplastic are less aggressive, whereasglioblastoma is the most aggressive. Clioblastoma multiforme (GBMis the most malignant of the astrocytic series, and is discussedbelow.
. Patients usually present with seizures, but may have focal deficits.Weakness and ataxia can develop.
. Diagnosis is suspected by magnetic resonance imaging (MRl), whiclshows a lesion with variable levels of enhancement, depending onthe grade of the lesion. Low-grade astrocytoma has littleenhancement, whereas anaplastic astrocytoma enhances, althoughnot as greatly as GBM.
426 DISORDERS NEOPLASMS DISORDERS-NEOPLASMS 427
\;x.r ilrr Irrnror r
rligodendroglioma
, ,lioblastoma,rrultiforme (CBM)
I'tittrrrry lltrrirr ltutrols
l 0ulurcs
Irr,,rtrrrr.rrt begirrs with proper diagnosis. Resection is performed ifpossiblc. But astrocytic tumors can infiltrate brain, resulting inexpanded deficit if there is aggressive resection of the lesion.
Radiation therapy and chemotherapy are offered for patients withmore malignant lesions.
. Much less common then astrocytoma. Can be low-grade oranaplastic.
. Pathologic features make the diagnosis.
. Patients present with focal deficit or seizures. lf seizures are notpresent at the time of diagnosis, they commonly develop later.
. Treatment is with resection. Chemotherapy is given especially foranaplastic oligodendrogliomas. Radiation therapy is given for mostpatients with anaplastic forms and patients with low-grade formswith incomplete resection.
. The most malignant form of glioma. This is highly undifferentiated,aggressive, and infiltrative. GBM is a single lesion, although migratorycharacter may give it a multicentric appearance.
. Diagnosis is suspected when imaging identified an irregularinfiltrative enhancing lesion.
- Debulking helps treatment, although complete resection is notpossible.
. Radiation therapy is almost always given. Chemotherapy usually isperformed as well.
. Prognosis is poor. Response to treatment is incomplete andtemporary. Progression is expected.
. Arises from the arachnoid layers, and begins extra-axially. Can extendinto the substance of the brain.
. Patients present with mental status change, focal deficit, seizures.Meningioma in the posterior fossa can produce hearing loss andataxia.
. Surgical resection is curative for many patients. lf the tumor hasextended into the brain, resection may not be complete. Rarepatients with malignant meningiomas may require radiation therapyafter debulking.

f )t'itntrry llrttitt ltttttot's tt\tnrrt\t
Specific Tumors Feotures
Acoustic neuroma . Benign tumors of CN-8. They are of increased incidencc irr p,rtrr,rrt.,with neurofibromatosis type 2.
. Although acoustic neuroma is a common name, the \erm vestilttrktrschwonnomo is a more recently used term.
. Patients present with hearing loss, tinnitus, and ataxia. lt is easy toascribe these findings to vestibulopathy, and, therefore, the diagnosoften is delayed.
. lmaging with MRI is sensitive for most acoustic neuromas, althouglrspecial views of the internal auditory canal may be needed to seethe lesion.
. Brainstem auditory evoked potential shows abnormalities that aresuggestive, although not diagnostic, of acoustic neuroma.
. Treatment is surgical if removal or debulking is needed. Somepatients have lesions that can be followed. Stereotactic radiosurgeryis another alternative.
Primitiveneuroectodermaltumor (PNET)
. lncludes the medulloblastoma, which is predominantly seen inchildren.
. Patients present with typical features of mass lesion and oftenhydrocephalus.
. MRI shows mass filling the 4th ventricle.
. Surgery is performed to resect as much of the tumor as possible.
. Radiation therapy and chemotherapy are given to reduce residualtumor.
. Steroids are given to reduce edema before and after surgery.
. Many children have a good response with long-term survival.
Craniopharyngioma . Arises from Rathke pouch or the craniopharyngeal cleft near thesella. lt is a slow-growing cystic lesion.
. Patients present with headache, visual loss, and may havenausea/vomiting. Some patients are asymptomatic and the mass isfound when a scan is performed for an unrelated reason.
. MRI shows a cystic mass in the suprasellar region. Calcifications areseen. Significant mass effect and even hydrocephalus can be seen.
. Surgical approach can be by a variety of methods, which woulddepend on size, location, and geometry of the tumor.
. Radiation therapy can be performed. Chemotherapy is sometimesused, although the effectiveness is debatable. Neuro-oncologistconsultation is needed.
428 DISORDERS NEOPLASMS DISORDERS-NEOPLASMS 429
l'titttrrt'y llt'rritt Ittttlrlts
Large acoustic neurinoma fi | | i ng cerebel lopontine angle,distorting brainstem and cranial nerves V Vll, VIll, lX, X
Meningioma invadingsuperior sagittal sinus
v"I
A
(\\.;'+ /-l^
,@d ,*/.d'i tW *
Yni u,N., /' *" -.1'';l \ =., -.1lY-' *7,-/
Large, hemisphericglioblastoma multiformewith central areas ofnecrosis. Braindistorted toopposite side
/'
r\Y, /I .r-'tf
{ Np-;(1 , '
:4vilViri
\(.
_i*.. \*\,{ a#
:,ill',.?,":;t:,r;; rr*-Y
I 't:

ffl Metastotlc Broln Tumors E
Br-ain metastases develop from malignant tumors. They have theireffects by mass effect, vascular changes, and tissue destruction.
Spread of tumor to the brain can be hematogenously or via directextension. Direct extension is more an issue with spihe tumors thanwith brain tumors.
Common tumors to produce brain metastases are:. Lung
. Breast
, Colon
. Renal cell
. Melanoma, Ovarian
. Patients usually present with focal or multifocal lesions with theirresultant symptoms. This can include headache, focal weakness,and coordination deficit.
. Signs of increased intracranial pressure are common, especially withextensive cerebral edema, multiple lesions, or hydrocephalus.
'
. Routine labs are normal.
. llngglng shows one or more enhancing lesions. MRI cannotdefinitively differentiate between tumor and abscess, but there areguidelines.
. Biopsy with pathology gives definitive diagnosis.
. Brain metastases are suspected when a patient presents with anycombination of focal weakness, seizures,'and headache. Onset isinsidious.
. lmaging suggests brain tumor. Clear differentiation between primarvand metastatic lesion cannot be made, but multiple lesions iuggesimetastatic disease.
. Pathology makes the diagnosis, from biopsy or resection.
. Primory broin tumor. The main differential diagnosis. Multiplelesions suggest metastases.
. Abscesses..Can be multiple and resemble metastases, especially inpatients with SBE.
. CNS lymphomo. Can be multifocal, and resemble metastases fromdistant tumor.
Pathophysiology
Laboratory studies
Differential diagnosis
. Diagnosis by biopsy is the first step in management. Resection isperfbrmed if the lesion is solitary. Multiple lesions are not resectedbecause of the possibility of extensive damage.
. Steroids are used for edema.
. Anticonvulsants are used for patients with seizures. Prophylacticanticonvulsants commonly are not used.
. Chemotherapy and radiation therapy are used for some patients,depending on the type and location of the metastases and primarytumor.
Metastatic tumors to the brain seldom are the cause of death;patients more commonly die from their systemic disease.
Metostotlc Broln Tumors
ei4'O DISORDERS-NEOPLASMS DISORDERS-NEOPLASMS 457

IVlllrtsltrlir lirrrtrt
Common primary sources
Tumors Melaslalit' kr llr.rin
I\\t
\rMetastatic met.rstases of small cell anaplitsti(o,rl , t'lJ,r.rrr in,)m,r oi Iung I,, lrr.rin
Axial CT demonstrates edema within the right frontal polc. An ill-defined hctcrogeneous region is seen peripherallri rvhich enhantlsaftor iodinated contrast administration. Inciclental snralI remotelacunar infarct is seen lvithin thc lcti putamen (arrorvhcacll.
Cerebellar mct.rstasisof cutaneorrs mclanoma
CT rvilh contrast cnhancementshorvs a similar large metitstasesin thc right cerebellum rvithcffacenre.nt o{ thc fourth ventricle
i.
-{
\{
-i,
Melanoma (skin ormucous membranes)
W
452 DISORDERS-NEOPLASMS DISORDERS-NEOPIA"i\/., 455
.,( r ll)lt( )ll
lrophysiology
SI'INAI. CORD TUMORS
. (,rrr l;t' I)rirnary or secondary
- Primary tumors are usually benign, whereas tumors that spreadfrom distant sites or contiSuous regions are typically malignant.
Primary tumors of the spinal sac include neurofibromas,meningiomas, ependymomas. Secondary neoplasms can spread byblood, cerebrospinal fluid (CSF), or contiguous extension from thetumor, which has metastasized to adiacent vertebrae.
rrrical findings Presenting findings usually are back pain and weakness. Theweakness is most commonly seen in the legs, although cervicalspine tumors can produce arm deficits; the pattern of weaknesscorrelates with the level of the lesion.
Reflexes are increased in the legs with cervical and thoracic spinelesions; they can.be reduced with lumbar spine disease and caudaequrna comPressron.
Bowel and bladder control deficits are common.
rboratory studies Routine labs are normal.
MRI shows a structural lesion in most circumstances. An enhancedstudy should be performed when neoplastic, infectious, ordemyelinating causes of myelopathy are suspected. lntrinsicneoplasms of the spinal cord may have normal MRI unless contrastis used.
Computed tomography (CT) may show spinal column destructionbut is much less sensitive for tumor in the canal.
Spinal cord tumor is suspected when patient with known cancerpresents with back pain and leg weakness. Non-neoplastic causescan be suspected, and some patients will have disc disease orsome other benign structural lesion.
Signs of myelopathy or cauda equina lesion support the diagnosis.
MRI confirms the diagnosis in most patients. lf the MRI is normal atthe level of the symptoms, then the MRI should be performed onmore rostral spinal segments, because the lesion can be above thelevel of the deficit.
lf MRI cannot be done because of artificial valve, pacemaker. orother implanted device, CT myelography can make the diagnosis. lnthis case, total myelography should be performed.
CSF analysis can be performed to look for neoplastic meningitis, butthere is some risk for increasing the deficit when lumbar puncture(LP) is performed when there is a structural spinal lesion.
rlagnosls
Slrrrrrrl ( orrl lrttttots

Differential diagnosis
S;rirtrrl ('otrl Iulll()t's tt,uttnnttt Sllrrr<rl ( orrl lurlr()r's
Neoplostic meningitis. Can present with radicular symptonrs .rrrlspinal cord involvement occasionally can occur.
Tronsverse myelitis. As a component of MS or acute disseminatt,rlencelphalomyelitis (ADEM), can present with myelopathy with anintraparenchymal enhancing lesion.
Degenerative chonges of the spine. Can produce cord compressiorr,which can subsequently appear as cord changes on MRI-myelomalacia can be difficult to distinguish from inflammatorychanges.
Surgical decompression is commonly done when spinal cord tunroris resulting in secondary compressive myelopathy.
Resection of extra-axial tumor can give the diagnosis. Biopsy orresection of intramedullary tumor is seldom done, and carriessignificant risk for neurologic deficit.
$PINA[, CORD TUMOnS*cont'd
Most patients improve with treatment, but the residual deficit iscommon.
Whether the lesion is curable is determined by the pathology andanatomy.
.,"1,
lntradural extramedullary tumor(meningioma) compressing spinalcord and deforming nervc roots
4T4 DISORDERS-NEOPLASMS DISORDERS-NEOPLASMS 455

l'rtt'rutr,oIrlrrsl i( Syn(ll()tll(,\
PARANEOPLASTIC SYNDROMES
Description . Paraneoplastic syndromes are remote effects of cancrtr. Ilrt'rr' ,rrr,several paraneoplastic syndromes and corresponding antiborlics,and the numbers are increasing.
. Can be described by the specific antibodies and the clinicalsyndromes
Pathophysiology Antibodies are created in response to the tumor cells. They attackneurons of the CNS and parasympathetic nervous system (pNS),producing a host of clinical presentations.
Clinical findings The most important clinical manifestations are:
Encephalomyelitis
Cerebellar ataxia
Opsoclonus-myoclonus syndrome
Polyneuropathy
Myasthenia gravis and LEMS
. There are other disorders that can occur as well, but this is lesslikely.
. Details of the specific entities are discussed below.
Laboratory studies . Routine laboratory studies are normal. Specific assays forparaneoplastic antibodies often are revealing.
. lmaging usually is normal.
. CSF may show a mild pleocytosis and elevated protein.Paraneoplastic antibody testing on the CSF is available.
. lmaging of body may reveal a cancer, with lung, breast, and ovabeing of specific interest. Positron emission tomography (pET) nhelp identify a neoplasm, in addition to MRt and CT.'
Diagnosis . Paraneoplastic syndrome is suspected when a patient with knowncancer presents with neurologic symptoms that are not associatedwith a structural lesion. CSF shows pleocytosis without neoplasticmeningitis. Paraneoplastic antibodies are positive.
. Paraneoplastic syndrome is suspected in patients without knowncancer when there is cerebellar ataxia or subacute onset ofdementia or encephalopathy without identified cause.
. lmaging is performed to look for structural lesions causing thesymptoms. LP also is often done.
Differential diagnosis . Neoplostic meningitis. Can produce weakness and multifocalneurologic deficits with no obvious abnormalities identified onrmaSrng.
. Metostotic tumor. Can produce ataxia and weakness, although it isusually identified on imaging with MRt.
aflanmay
416 DISORDERS-NEOPLASMS DISORDERS-NEOPLASMS 4I7
r,rlittrtt'ttI
l'A llANl ( )l'l.ASI lC SYNDI{OM[,S*cont'd
- llrr,rt, is no proven treatment of ParaneoPlastic syndromes.Corticosteroids, intravenous immunoglobulin C (lVlG), or plasmaexchange are used to suppress the autoimmune resPonse.
. Treatment of the tumor can produce improvement, althoughtreatment does not always help the paraneoplastic syndrome.
rical course Patients may improve with treatment with immune-modulation ortreatment of the underlying tumor, but persistent symPtoms areexpected. Also, there often is progression of the causative tumor.
Speciflc Entity Features
cephalomyelitis Encephalopathy with cognitive changes, Iethargy, and Progressivefunctional decline can be seen with anti-Hu, APCA-2, ANNA-3.
Most common associated tumors are lung (especially small cell),breast, and testicular.
Seizures can develop, and may be the presenting sign.
'rebellar ataxia Progressive cerebellar ataxia with appendicular and axialmanifestations can be seen with anti-Yo (APCA-l), APCA-2, Tr, andperhaps other antibodies.
'ripheral,uropathy
Can be sensory and/or motor.
Small cell lung cancer can be associated. Anti-Hu and anti-Yo aremost correlated.
ia gravis . Associated with thymoma in some patients
. Removal of thymoma can result in eventual improvement in theMG, although the improvement is delayed.
rmbert-Eatonyasthenic syndromeEMS)
Produces weakness and autonomic insufficiency
Small-cell lung cancer is most commonly associated with LEMS.
Diagnosis is established by clinical symPtoms, NCS and EMG
findings, and antibodies to voltage-gated calcium channels.
syndromeus . Characterized by rapid irregular eye movements (opsoclonus),
myoclonus, often associated with ataxia or dysarthria.
. Breast cancer often is associated, with anti-Ri antibody.
lyasthen,nG)
rmbertryasthe
rpsoclonuiyoclonus
l'tu rurt,olrlr rsl ir .Syttrltotttt's

Antibody Torget Clinicol Associqtion
Hu (ANNA-l) . Anti-Hu or antineuronal nuclear antibody-l is associated withencephalopathy or neuropathy. Small cell lung cancer is thc chit'lassociated tumor.
Ri (ANNA-2) Associated with opsoclonus-myoclonus syndrome, and also is set'rwith breast cancer. Other cancer associations have been determitrras well.
Ta (Mal, Ma2) . Anti-Ta antibodies can be associated with limbic encephalitis. Ma2associated with testicular cancer. Mal antibodies may contribute,but Ma2 appears to be the most important element.
Yo (APCA-I) Anti-Purkinje cell antibody is associated with paraneoplasticcerebellar degeneration or peripheral neuropathy. Myopathy andcorticospinal tract degeneration also can be seen.
Voltage-gatedcalcium channel(vccc)
. Antibodies to the VCCC are found in most patients with LEMS.
Tr Tr is an anti-Purkinje cell antibody seen in patients with subacutecerebellar ataxia associated with Hodgkin's lymphoma.
ANNA-3 . Antineuronal nuclear antibody-3 is yet another anti-Purkinje cellantibody associated with small cell lung cancer.
. Patients may have cerebellar ataxia, brainstem or limbicencephalitis, or myelopathy.
I'<t t tt ttt't lg ll(lst i(' .SyIl( ll'()IIl('s t,rtttrtrrr'rl
Nt.ttrotttttsr rrl,rr M.rrrilr.sl.rlionsoI llronllrolir.rrir ( .rlr irrorrra
Lambert-Eaton syndrome: weaknessof proximal muscle groups (often
manifested by diiiit ultl in ri'ingfrom chair)
l't r t r t ttr,o1 rl<tsl ic SyttrIr'()tIl(,r.i
S u bac utecerebel lardegeneration,vertigo, ataxia
\?*...
?l#I *?l.!':. {. 41*s \ -*q ,1
'I mv 0.,|*,Jt z1
"' al
l€4 sec 3 stim/sec
k--r]1 sec lo stim/sec
,j
;li.clil
ty
li: "* "1" ;.q{"*
,,S!t'.i.,,r tEX[. ,
t#,
. il
Wffi{ltilt{ilfiff1{lllllllll
Electromyographic abnormal ityin Lambert-Eaton syndrome(readings from hypothenarmuscles with stimulation ofulnar ncrvc at wrist). Notelow amplitude and initial decline(Normal = 5 mv or morewith no initial decline)
Peripheral neuropathy;paresthesias, pain,loss of function
458 DISORDERS-NEOPLASMS DISORDERS-NEOPLASMS 4I9

Apptorrr lt lo loxir /Mclrrlrolir I)isorrL,rs
APPROACH TO TOXIC/METABOLIC DISORDIRS
Description . Toxins are suspected when a patient presents with mental statrrschanges or weakness that is not related to identified structur.rl,infectious, or immune mediated disease.
. Withdrawal from many agents also can present with mental statuschanges.
Types ofpresentations
. Encephalopathy
. Ataxia
. Movement disorder
. Myopathy
. Neuropathy
Red flags fortoxic/metaboliceffects
. Toxic and metabolic abnormalities are suggested by development olneurologic deficits, which are diffuse, nonfocal, and without astructural cause.
. lnfectious and autoimmune etiologies must be considered.
Presentotion Feotures
Encephalopathy . Mental status changes due to toxins usually have a subacute onset.Differentiation from dementia is the short duration and presence ofdisordered level of consciousness, from agitation to lethargy to
. Many toxins can produce encephalopathy, including analgesics,antidepressants, neuroleptics, anticonvulsants, andsedative/hypnotics.
Ataxia Can affect gait andlor limbs
Chronic alcohol intoxication can produce cerebellar degenerationwith predominant gait ataxia. Any drug that can produce mentalstatus alteration can produce ataxia. Anticonvulsants can produceataxia and nystagmus even at doses that do not produceencephalopathy, especially phenytoin and carbamazapine.
Movement disorder . Can be created by numerous drugs. Not all of these effects are attoxic doses.
. An akinetic-rigid syndrome indistinguishable from Parkinson's diseican develop from neuroleptic administration.
. Valproate and amiodarone can produce a tremor, but in rare casesalso can give a parkinsonian appearance.
. Chorea can develop from certain medications, including someanticonvulsants, levodopa, antipsychotics, oral contraceptives,amphetamines, cocaine, and tricyclic antidepressants.
. Dystonia can develop from chronic use of neuroleptics.
. Tardive dyskinesia develops from use of antipsychotics-the neweratypical neuroleptics have a lower incidence of TD.
440 DISORDERS-TOXIC/METABOLIC DISORDERS-TOX|C/tVETABOI l( 44r
Itr csr,rtlrrl iorr
l,4yo1r,rl lry
Apptortr lt lo loxir /Mcltrlrolit I)isotrk'ls
Ieotures
:,::'r:,,'".,,.0 from alcohol intoxication, and frank rhabdomyolysis can
Statins have been described as producing myopathy, although theincidence of myalgia and myopathy attributed to statins is largelyoverstated.
Cocaine can produce myopathy and rhabdomyolysis.
Corticosteroids with chronic use can produce a myopathycharacterized by atrophy of type 2 muscle fibers. Acute myopathyalso can develop with rhabdomyolysis, although this is rare.
. Several chemotherapeutic agents can produce peripheral neuropathy.Vincristine and cisplatin are two of the prominent agents, but thereare others.
. Phenytoin can produce a sensory neuropathy.
. Cold can produce a motor neuropathy.

I lcrtvy Mclrrl lrtloxicrrlion
HIAVY METAL INTOXICATION
Description Heavy metals are an uncommon but important cause of neurotoxirity
Pathophysiology The most important elements to produce heavy metal intoxication .rrt.
Lead
Mercury
Arsenic
These elements interfere with the normal metabolism of the neurons.
Element Findings
Lead . Main sources of lead toxicity are paints in old houses, enamel on sonlimported toys and jewelry and industrial exposure.
. Clinical features include central and peripheral manifestations. Centralsymptoms are headache, irritability, Iethargy, and associated cerebraledema. Peripheral symptoms include distal numbness and weaknessdue to neuropathy. Acute high-dose exposure is more likely to productcentral findings, whereas chronic lower-level exposure is more likely toproduce peripheral neuropathy. Non-neurologic findings in adults caninclude lead lines in the gingival tissue, which can be seen with anyheavy metal intoxication.
. Laboratory findings include elevated blood lead level. Some patientsmay have anemia, especially children.
. Treatment is with cessation of exposure, chelation, and supportivetherapy.
Mercury . Mercury intoxication can be from organic or inorganic mercury.Minamata disease is an example of organic mercury intoxication.lnorganic mercury intoxication comes from contact or inhalation of themetallic mercury or the vapor.
. The clinical features of mercury intoxication are varied, but can includecognitive difficulties, symptoms of peripheral neuropathy, ataxia, visualand hearing loss. Emotional instability is common.
. Blood and urine mercury levels are increased.
. Nerve conduction study (NCS) and electromyelogram (EMC) showaxonal neuropathy.
. Chelating agents are used for treatment.
Arsenic . Arsenic poisoning usually is from exposure to certain insecticides andthrough intentional poisoning. Certain herbs may contain arsenic. Todexposure from smelting is not expected.
. Acute intoxication by ingestion produces pain with burning in themouth, followed by gastrointestinal (Cl) distress.
. Chronic intoxication can produce peripheral neuropathy with sensoryand motor symptoms.
. Diagnosis is made by urine measurement and assay of hair and nails,
. Treatment is avoidance of exposure and supportive. Chelating agentscan be used, but their benefit is controversial.
442 DISORDERS TOXIC/METABOLIC DISORDFRS-TOXIC/MFIABOI IC 447
(:, .
{,-
Antique copper utensils (e.g., still krr
bootleg liquor) and runoff wastt'lrorrrcopper smelting plant may be sourr cs
of arsenic poisoning
llistory of nausea and vomiting may.rr66r.sl :rsenic poisoning in pdlrcnlivith pcripheral neuropathy
Although 24 hour urinalysis is best diagnostic test forarsenic, hair and nail analysis may also be help{ul
Spotty alopecia associated withperipheral neuropathy characterizesthallium poisoning
Mees' lines on fingernails arecharacteristic of arsenic poisoni ng
;...,,j.:i
Ilr,rtvy Mr,lrtl lttloxir rtliott
l1'rrplrlr,rl Nlrrrop.rllry ( .tttsctl lry I !r'.rvy Mcl.rl !'oisrrrirrg
ilrunI,,,,',I nrr I
,PolsoN iI r r;r
!I .-:k! ./../t{ -' -d"
Rat poison is the mostreadily availablesource of arsenic
^J':A
i;
1l
itt'-{t
tJr
,iw,J' x
4{trLead poisoning, now relatively rare, causesbasophilic stippling of red blood cells.24-hour urinalysis is diagnostic test
l3 "r
.#" ".*sry/4n
Pl
., *;

r ,.r,. .r.,,': , , ';' ': ,: .;
: ' !: :.:l l IfIOLINE$TERASI INIIIEITOR$
Description . Used in weak form for patients with Alzheimer's disease arrtl otldementias, as well for myasthenia
. High-potency agents include some pesticides and nerve agents.
Pathophysiology Binding and inhibition of the acetylcholinesterase produces increas,availability of acetylcholine at the terminal, which is the basis forbenefit in patients with dementia and myasthenia. Hyperstimulatiorresults in damage to the nerve terminal with use of high-potencyagents such as organophosphates.
Clinical findings . Acute intoxication results in Cl distress, confusion, seizures, cerebedema (if severe), and can result in death. The acronym SLUDGErefers to salivation, lacrimation, urination, defecation, Gl distress,and emesis.
. Delayed neurotoxicity can be manifest as peripheral neuropathicsymptoms, including weakness with cramps and sensory symptorThe prominence of motor deficit is more suggestive of delayedneurotoxicity than sensory symptoms.
Laboratory studies . Routine labs are normal. Red cell cholinesterase activity is reducin patients with acute exposure.
. lmaging is normal.
. Electrocardiogram (ECG) can show arrhythmia.
. There are NCS and EMC abnormalities; however, these special trare not routinely performed.
Diagnosis . Cholinesterase inhibition is suspected when a patient presents wisalivation and Gl distress. This suggests acute toxicity.
. Delayed neurotoxicity is considered when a patient presents withneuronal degeneration without another identifiable cause.
. Red cell cholinesterase assay only is helpful for identification ofacute toxicity; delayed neurotoxicity depends on a history ofsignificant exposure.
Differential diagnosis . Encepholitis. Can present with seizures, mental status changes,Cl distress, although the profound salivation is not expected.
. Other couses of polyneuropothy can present with distal sensorymotor findings, which can resemble the delayed neurotoxicity.
Management . Treatment for acute intoxication is supportive. Seizures are treatedwith diazepam or other benzodiazepine.
. 2-PAM is an antidote that often is given in addition to atropine,especially for patients with severe intoxication.
Clinical course Most patients improve from the acute intoxication, althoughneurotoxicity has no effective treatment.
( ltolint,stt,t'usc It)l)il)il()ls
l,l
re.tslr I
DT
atirrr r
erebr,rl
symPtonr\
e<l
an(l
,attrl
delayed
tesl\
willr
444 DISORDERS-TOXIC/M ETABOLIC DISoRDERS-TOXIC/METABOt r(' 4/r5
a&aW"
( lrolittt'slr,r'os(' Inltil)il()r'ri
lhc l'upils in l'oisoning
^ ,{ nu": \ ,V. '
't
Miosis (pinhole pupils)Seen in poisoning by morphine andmorphine derivatives, some types ofmushrooms, cholinesterase inhibitors,parasympathomimetics, nicotine, chloralhydrate, sympatholytics, and some othercompounds

*{Y
446 DISORDERS-TOXIC/METABOLIC DISORDERS-TOXIC/M ETABOLIC 447
)r'\( nl)tton
wrlllPllylt slNployEl ,- Alrrrost as rnuch of a medical problem as intoxication
- May develop because the patient runs out of money, decides tostop a habit, or is institutionalized (e.g., jail, hospital) and has noavailability
. lf the patient has not been honest about their substance use,withdrawal will not be anticipated by others.
'athophysiology The agents from which patients withdraw are so diverse thatgeneral pathophysiology cannot precisely be discussed.
ln general, alcohol and drugs produce adaptive changes in the brainthat can evoke dependency on several planes: molecular, neuronal,andlor psychologic.
Lack of "feeding" a dependency can create a craving for thesubstance, as well as autonomic symptoms common to withdrawal.
findings Common findings with withdrawal are anxiety, agitation, andcraving. Adrenergic symptoms are common, including tachycardia,diaphoresis, abdominal pain, and nausea.
Alcohol withdrawal can produce confusion, seizures, fever, andhyperventilation. Delirium tremens (DTs) is progression of thewithdrawal state to prominent cognitive change. Seizures may occurprior to the DTs.
Opiate withdrawal can produce many of the same symptoms, andcommonly causes nausea, vomiting, dianhea, and abdominal pain.
studies Routine labs usually are normal.
Drug screen commonly is normal because patients have been offthe agent(s) for several days.
Magnetic resonance imaging (MRl) and computer tomography (CT)are normal, except for atrophy, which is a common finding withchronic alcoholism.
Electroencephalogram (EEC) may be normal, but if there are mentalstatus changes, slowing is common.
Cerebrospinal fluid (CSF) commonly is obtained to look forencephalitis or meningitis, but is normal.
Withdrawal syndrome is suspected when a patient presents withanxiety, agitation, diaphoresis, and tachycardia.
The presentation can suggest CNS infection, and, therefore, imagingand CSF analysis often are performed, especially if the diagnosis isnot certain.
Normal studies and a history from the patient or associates ofsubstance use make the diagnosis.
Clinical
Laboratory
Diagnosis
Wil lrtlrrrw<rl Syrrrlrrrnrt,s

Differential diagnosis
"r
Expression and severity of symptoms varywith duration and degree of dependenceand with recognition and treatment of earlywithdrawal
Sweating
Flushing andtemperature elevation
Ceneralized seizures occur in87" of cases. Focal or multipleseizures suggest other cause
' --lWi I lrrlrrrwrr I Synrtrrrrrrt's
Visual and auditoryhallucinations
Anxiety andconfusion mayprogress todisorientationand delirium
W i t I rr I n rwr t I .Sy t tr I t'ott)(,ri,,,,,ri,,,/,r,
$YNDf,OMES---cont'd
CNS infection. With encephalitis or meningitis, can present irr asimilar fashion.
Hyperthyroidism. Can present with some of the same symptoms
Pheochromocytomo. Can present with episodic hyperadrenergicsymptoms, although the episodes are briefer than withdrawalsyndromes, and blood pressures (BPs) are extremely high.
Supportive care is essential, with management of the autonomicinstability and sedation when needed. Benzodiazepines arepredominantly used.
Clonidine or propranolol often is used for cardiovascular protection
. There is a real risk of death from withdrawal, mainly fromcardiovascular causes.
. With treatment, most patients do improve, although the risk forsubsequent substance-use problems continues to be problematic.
I )(\ k,,t\(,lnllA( r(.sulls ir)
l'flcx.rulononrichypr.rexcitabi I ity
Headache
E Vomiting
t Heartrate
Narrsea
t Bloodpressure
,r".o\ iiil,l l.
J\&"
tu -41':
448 DISORDERS-TOXIC/M ETABOLIC DISORDERS- TOXIC/MEIABOLIC 449

Wi I lt<ltrtw<t I Sytt<l rt lttt('s r,rrrrrrrrrl
Sweati ng
Dilated pupils
Lac rimatio n
Rhinorhea
Yawning
:l)
a
l
!\
Insomnia and muscle achesmediated via p receptorsand relieved by p agonists
Opiod Withdrawal
Signs and symptoms
Na useaandvomiting
l;fl *::,
Locus ceruleusn
Anxicly and
ngitation
i":l
High-dose benzodiazepine withdrawalproduces signs and symptoms similar toalcohol withdrawal
cl-q@GABA-* xBenzodia-).)zeprne J
At therapeutic levels, benzodiazepinesact synergistically with CABA to inhibitneurotransmission, preventing anxiety
lnsomnia and 7nightmares
Low-dose (therapeutic) withdrawal
h"
d
i;J
-x
{{
J0llhlA,€RAl&;roA^, ,/ / I
L,/7dr,tutd"s
Sensory hypersensitivity
Sound
Noradrenergic effectsof withdrawal (mediatedvia locus ceruleus)increase heart rateand blood pressure
JlSHl{ i\.€$lAK;xnI5r? ,/ r''
L./Y,*nAdt*
cl- lF."cABA-L)
',.i--l
'Benzodiazepine
Symptomrecurrence
Low-dosewithdrawalsyndrome
Low-dose withdrawal syndromeSymptoms typical of sedative/hypnoticwithdrawal, fluctuating hypersensitivity tosensory input, muscle twitching,depression, and depersonallzation
I ligh-rft rsr. willrrh.rw.rl
I lylr'rgryrcrr,
Wi I ltr I trrwrr I .Syttrlrotrtcs
lk.nzorli.rzcgrino Wi lhdrawal
r.ffii, --..*, i
li. r" 4
ffiT'u --
Withdrawing long-term benzodiazepine causes loss of synergism with CABA inhibition,resulting in recurrence of original symptoms and low-dose withdrawal syndrome
\\!:'3' %.1::Depression and
450 DISORDERS-TOXIC/M FIABOLIC DISORDERS-TOXIC/M FIABOLIC 45I

l.lcr'lrolylr, Alrrror rrrrrlil ics
th,rl
rf thr,use<1,
ELECTROTYTE ABNORMALITIES
Description Numerous electrolyte abnormalities can produce neurologicmanifestations. This discussion concentrates on neurologicmanifestations oI the electrolyte abnormalities.
Sodium Disorders
Hypernatremia . Hypernatremia is usually due to dehydration, with concentration ol I
blood sodium.
. Clinical features are confusion, Iethargy, and sometimes agitation.Seizures and/or myoclonus may occur.
. Associated medical findings are tachycardia, oliguria, hypotension th,is orthostatic, and generalized weakness.
. Treatment is with hydration. Acute hypernatremia can be rapidlyreversed. Chronic hypernatremia requires slow reversal because of tlrisk for cerebral edema. Nonsodium containing fluids usually are usehowevel if the patient has marked hypovolemia in addition tohypernatremia, isotonic fluids often are administered initially.
Hyponatremia . May be seen in alcoholics or in patients with certain medicalconditions such as renal failure, hepatic failure, pneumonia, orcongestive heart failure (CHF)
. Clinical features are nausea, vomiting, confusion, and lethargy.
. Seizures and coma may develop with profound hyponatremia.
. Treatment depends on the clinical situation, including concurrentmedical illness, tonicity, and volume status.
Potossium Disorders
Hyperkalemia . Usually related to renal insufficiency, potassium supplements,rhabdomyolysis, or other potassium-releasing injury
. Clinical features are paresthesias and diffuse weakness. Cardiacanhythmia may produce palpitations, although the incipientarrhythmias may not be symptomatic.
. Treatment can include calcium supplements and glucose with insulinSodium bicarbonate especially is used with hyperkalemia cardiacarrest. Many diuretics can enhance excretion of potassium, and is allthat is needed for many.
. Binders usually are not needed.
Hypokalemia Usually is due to potassium-wasting diuretics and Gl losses
Clinical features include generalized weakness that is due toimpairment in muscle contraction. Associated symptoms includenausea, vomiting, abdominal cramping, and palpitations. ECC mayshow characteristic T-wave changes and arrhythmias.
Treatment is with potassium supplementation. lf hypomagnesemia isconcurrent, both need to be treated.
452 DISORDTRS-TOXIC/M ETABOLIC DISORDERS-TOXIC/MFIABOLIC 455
Ilypcrr,tlr trrrr,t
lypocalcemia
!ypermagnesemia
ryPomaSnesemra
l lr,r Irolylr, Al)n()r'tn(rlitics
l )isortklrs
Ilrr. rrrost (()nunon cause is malignancy with bony erosion. Sarcoidosis,rrrrl lryperparathyroidism also have to be considered.
Clinical findings are confusion, nausea, vomiting, abdominal pain, andweakness. With rnarked hypercalcemia, coma may ensue.
Diagnosis can usually be made by measurement of calcium, albumin,and parathyroid hormone (PTH) levels. A history of malignancysupports that diagnosis.
Treatment begins with hydration in most patients. Loop diuretics canhelp to reduce the calcium level. Dialysis may be needed for patientswith renal failure, in whom aggressive hydration is not possible.Treatment of the parathyroid abnormality or malignancy also is donewhen possible.
Prognosis for patients with malignancy with hypercalcemia is notgood, but because of the tumor-not the calcium abnormality.
Mognesium Disorders
. A host of metabolic derangements can produce hypocalcemia. Thesecan include cirrhosis, renal failure, sepsis syndrome, any cause ofhypomagnesemia, rhabdomyolysis, malignancy, PTH deficiency, andcertain medications.
. Clinical features are muscle cramps and twitching, dysesthesias, andparesthesias. With severe hypocalcemia, confusion, lethargy orirritability, and coma can develop; seizures are also possible.
. Treatment is with calcium replacement. Administration can be oral forpatients with mild symptoms and modest hypocalcemia, andintravenous for more severely affected patients.
Some of the important causes are acute renal failure, rhabdomyolysis,malignancy, diabetic ketoacidosis (DKA), and excessive administrationof magnesium (e.g., for eclampsia)
Clinical features are nausea, vomiting, and generalized weakness.Arrhythmia is common and can range from conduction delay to death.
Treatment is with hydration and supportive care. Diuretics can reducemagnesium levels, albeit slowly.
. Most commonly seen in alcoholics. Malnutrition from any cause alsocan produce hypomagnesemia. Certain drugs, including diuretics andchemotherapy agents, can be a cause.
. Clinical features include generalized weakness, muscle cramps, andtwitching. Severe cases may have confusion, lethargy or irritabiliryataxia, and/or seizures.
. Treatment is with magnesium replacement. Seizures can be treatedwith benzodiazepines.

I lypor;lyt:t'nrirr rrrrrl I lygrt,r'r;lyr crrrirr
Both are associated with significant neurologic implications.
Patients with stroke have a poorer outcome with significanthyperglycemia or hypoglycemia.
Feotures
The reduction in glucose after a meal. lt is most often seen rnfemales, usually younger than age 45 and often overweight.
Patients can present with weakness and hyperadrenergicsymptoms. Hunger, anxiety, tremulousness, and tachycardia aretypical symptoms.
Patients with reactive hypoglycemia are at risk for diabetes,including both normal and overweight patients.
Treatment is with dietary manipulation, including frequent smallermeals, complex rather than simple carbohydrates, and exercise.
lnsulin administration can result in hypoglycemia intentionally orunintentionally. Patients may not always notice the hypoglycemia,especially with long-standing diabetes, where the adrenergicresponse to hypoglycemia is blunted.
Treatment is with glucose replacement and supportive care.
Prognosis is usually good; however, profound and prolongedhypoglycemia can produce permanent damage.
Features
Hyperglycemia in the setting of insulin deficiency. DKA can be thepresenting symptom of diabetes mellitus.
Clinical features are thirst, polydipsia, and polyuria. Associatedsymptoms are weakness, fatigue, nausea, vomiting, and anorexia.Exam shows tachycardia and signs of dehydration.
Patients may be confused or even comatose. Ketotic breath ischaracteristic.
Diagnosis is suspected when a patient presents with ill appearanc(.,some of the typical features, and with glucose level >300mg/dl.Acidosis also is present.
Treatment is with fluid replacement, balance of electrolytes, andinsulin administration. Patients with DKA often are fragile.
Hyperglycemia with hyperosmolarity in the absence of ketosis.Unlike DKA, this is predominantly a disorder of patients withestablished diabetes, and is less likely to occur as a presentingmanifestation.
Neurologic manifestations include confusion and lethargyprogressing to coma. Focal signs, including hemiparesis andloraphasia, can suggest stroke. Seizures can develop.
Glucose often is markedly increased, higher than with DKA, and<500*mg/dL.
Treatment is with hydration, critical care support, correction ofelectrolyte abnormalities, and insulin. lf infection was a cause,appropriate antibiotic treatment is needed.
Reactivehypoglycemia
lnsulin-inducedhypoglycemia
Diabetic ketoacidosis(DKA)
Hyperosmolarhyperglycemianonketotic coma(HHNC)
454 DISORDERS-TOXIC/METABOLIC DISORDTRS-TOXIC/N/ FIABOLIC 455
I lygror;lyr ctttirr rrrtrl I lypr,r'rlly( (,tnio
taken upby musclc
lnsulin permits rapidentry of glucose intomuscle and fat cells
Ciiculattoo
Blood glucose falls
Rapid dcclineof blood glucosestimu latesadrenal medulla
Brain deprivedof glucose
:!
f -.I [: U:rI llv s
It. t.
: '11,.t:; ,
. r.l,tl
ji'
Epi nephri ne
l./\n \ r(,t\',s\\'c.rti ne,I rcnlottac hyr a rcliarvt-.t kness
[)isoricntation,r onvu lsions,unconsc iousnessshock
,\u

[t B12 Deficlency Brz Deficlen.y fEl
81, deficiency usually is due to impaired absorption rather thandietary deficiency. Long-term B,2 deficiency results in dysfunction ofthe posterior and lateral columns of the spinal cord. ln addition, thereoften is polyneuropathy and central brain demyelinating changes.
An impoftant cause of weakness and ataxia because of central andperipheral effects
. Patients present with any combination of peripheral, central neural,or hematologic problems. Not all are present in all patients.
. lmportant symptoms are:
. Ataxia
. Weakness
. Fatigue
. Sensory loss
. Neurologic symptoms commonly develop prior to developmentof hematologic abnormalities.
. Exam may show cerebellar ataxia, corticospinal tract signs withincreased tendon reflexes and upgoing plantar responses,decreased reflexes from polyneuropathy, confusion from cerebralinvolvemen! and visual loss from optic neuropathy.
Routine labs are normal, except some patients may have alreadydeveloped a macrocytic anemia. B,, level is low but measurementof methylmalonic acid and homocysteine provides even greaterdiagnostic sensitivity.
lmaging with magnetic resonance imaging (MRl) may showabnormalities on T2-weighted imaging consistent with the lesion.These lesions improve with treatment.
Clinical findings
Laboratory studies
B,, deficiency is suspected when a patient presents with acombination of clinical signs that cannot be explained by a singlelesion. For example, cerebellar ataxia, myelopathy, and signs olneuropathy would suggest 8,2 deficiency.
Diagnosis is confirmed by measurement of B,r, methylmalonic acid,and homocysteine levels.
Differential diagnosis The main elements in the differential diagnosis are other conditionsthat produce multifocal abnormalities.. Multiple sclerosis. Can present with the combination of cerebellar
and corticospinal dysfunction. Cognitive dysfunction can develop,although this is usually with advanced disease. Polyneuropathy isnot expected.
, Vosculitis. Can produce multifocal central and peripheral findings,and is considered in patients with Br2 deficiency. Differentiation ison labs and MRI appearance. Biopsy often is needed to make thedefinitive diagnosis of vasculitis.
81, replacement is key. lnitial B,, administration can be as often asdaily, with reduction in frequency of injections as the B,, has beenreplenished. Life-long replacement is needed. lnjections are neededinitially.
Most patients improve, although some deficit may persist. AlthoughB,2, methylmalonic acid, and homocysteine levels normalize withinl-2 weeks, weeks to months are required for improvement in theneurologic condition.
456 DISORDERS-NUTRITIONAL DISORDERS_NUTRITIONAL 457

ll,, I )r'ltr it'lt( / ,,,rrrrrrri,,i
Degeneration of posterior columns, andcorticospinal and direct spinoccrcbel lartracts, chiefly in midthoracic spinal cord
Subacute Combincd Dcgenoraliort
Ataxra,especial lyin darkncss
.f "t*tt. | /
G lossitiscommon
Pernicious anemia with macrocytosis,poiki locytosis and polychromatophi liaalmost always present. Hemoglobinmay be normal, mean corpuscularvolume elevated. Bone marrowcharat:teristicallv abnormal
458 DISORDERS-NUTRITIONAL DISORDERS-NUTRITIONAL 459
I )r..,( ill)lton
I ',rIlrophysiology
rluAMtNr-D-Erl!]ryg_( ,rrr protltrt.o the combination of ocular motor abnormalities,l,,,ly!r!roluthy, utu*iu, und ..- Thiamine deficiency usually is nutritional. Classic presentation is in
patients with alcoholism, although thiamine deficiency syndromesare also seen in some patients with cancer.
. There are multifocal degenerative changes with damage especiallyprominent in the mammary bodies and periaqueductal gray matter.
t linical findings Thiamine deficiency has two distinct presentations-Wernicke'sencephalopathy and Korsakoff's syndrome. Without treatment,Wernicke's encephalopathy progresses to Korsakoff's syndrome,and, therefore, they should be considered manifestations of thesame disease process.
Wernicke's encepholopothy produces a combination of diplopia,nystagmus, confusion, and cerebellar ataxis. Patients may not haveall the features. The ocular motor features often include loss oflateral gaze and horizontal nystagmus. The ataxia involves gait andtrunk more than Iimbs.
Korsokoff's syndrome presents with confusion, confabulation, andpsychotic features.
Most patients with chronic thiamine deficiency have some degreeof polyneuropathy, giving distal sensory deficit with or withoutmotor deficit.
Laboratory studies Routine labs are normal, although some patients will have findingsconsistent with chronic alcoholism, including hyponatremia andelevated liver function tests (LFTs). Transketolase and thiamineIevels can be reduced. Pyruvate levels may be increased.
lmaging with MRI often shows abnormalities on Tr-weightedimages in the thalamus and periaqueductal gray.
Lumbar puncture (LP) usually is normal, but is often obtained forstudy to look for infection, hemorrhage, demyelinating disease, andother conditions that may resemble Wernicke-Korsakoff syndrome.
Diagnosis . Wernicke's encephalopathy is suspected when a patient presentswith encephalopathy and has ocular motor defects. Abnormal labs,abnormal MRl, and determination of a history of predisposition byalcoholism or other chronic disease support the diagnosis.
. Korsakoff's syndrome is suspected when a patient presents withconfusion and confabulation, and is suspected of having a history ofalcohol abuse or other chronic disease.
Differential diagnosis . Encepholitis ond certoin forms of meningitis. Can present withconfusion and ocular motor abnormalities. LP with cerebrospinalfluid (CSF) analysis can distinguish these diagnoses.
. Multiple sc/erosrs. Can produce multifocal abnormalities onexamination. However, cognitive abnormalities are not commonearly in the course.
I ltirttttittc I )r,licir,ttr y

Management
I ltirttnittc I )t'lit'it'rrt'y,,\ttt,tt,,t
TIIIAMINU D[f ICtrENCY.*<ont'd
Administration of thiamine is the definitive treatment. lmrnedi,rtt'injection of thiamine on suspicion of diagnosis is followed by d.rrlyoral thiamine.
Before the thiamine administration results in definitiveimprovement, psychosis and agitation may have to be treated.Neuroleptics and benzodiazepines commonly are used; the latter,in part, can treat the alcohol withdrawal, which commonlyaccompanies thiamine deficiency.
Most patients improve, especially if the patient is treated early. Fullydeveloped Korsakoff's psychosis often ends in incomplete recovery.
l'r inr ilrrl lrxxl sortrr t's
Wholt'grain ccreals
1," ffiU
Alcoholdiet :'
ili;ii
I lritrrttirrt' I )t'lit'icttt y
Thiamine pyrophosphate(cocarboxylase) acts viaaldehyde
,i"
I
ili,illlil1:ti
,'rl-r'
H,C C.I
N
W&wVegetables
Heptose phosphate
Triose phosphate
Catalyzes condensationof pentose (ribulose)(Transketolase reaction)
Deficiency causesaccumulation of pentose;blockage of directoxidative pathway of
Oxalacacid4
tMalicacid
&{Nfl jii,xxi * {:i :}[:x'" {p. ;:u'::ul,tffi:::ff lx:"'1
glucose and TPNH production
Catalyzes dccarboxylationof pyruvic acid to acetate
Deficiency causesaccumulation of pyruvicacid; blockage of entryinto Kreb's cvcle
Catalyzes decarboxylationof o-Ketoglutaric acid
Deficiency causesaccumulation o{o Ketoglutaric acid;blockage of Kreb's cycle
I-'entr)s0 shuntdircct oxiclativc lr,rth6-phospho-gluconrc acrd + TPNH
rpN++co,2J Pentose-t Phosphate + reNH
id',# (lI colr sisrlr$
'rili'[{ Phosphatase
,;:l
,.rii
rii:Iii Pvruvic
***r,"--^ |Cor<
460 DISORDERS-NUTRITIONAL DISORDERS NUTRITIONAL 46I

DI.dBf,TT$ MEILITUS (DM)
Description . Divided into types 1 and 2
. Type I diobetes has a childhood onset and is due to impairedinsulin control over glucose. Patients are insulin dependent.
. Type 2 diobetes has an adult onset and is due to insulin resistanccwith some level of insulin production deficit.
Pathophysiology . Type I diobetes is predominantly a genetic condition, with thepossibility of environmental triggers.
. Type 2 diobetes is more likely in obese patients, in pregnancy, andwith a family history of adult-onset diabetes.
Clinical findings . Patients may present with symptoms of hyperglycemia, includingpolydipsia and polyuria.
. Patients may present with diabetic ketoacidosis (DKA) orhyperglycemic hyperosmolar nonketotic coma.
. Patients may be asymptomatic for years prior to the diagnosis.
Laboratory studies . Routine labs may show hyperglycemia, but this is not invariable,because the levels are erratic. Blood glucose commonly is high.
- Hemoglobin Arc (HbArc) is elevated in patients with diabetes,indicating persistence of deficits of glucose control.
. Long-standing diabetes can produce laboratory findings ofneuropathy, renal damage, and cardiac damage. Neuropathycommonly is present at diagnosis.
. lmaging usually is not needed, because this is not a structuralproblem. If there are focal neurologic signs, magnetic resonanceimaging (MRl) or computer tomography (CT) is needed to assessfor stroke, etc.
Diagnosis Diabetes is suspected when a patient has polyuria with polydipsia.With this history random glucose often is found to be high. Clucoselevels and HbA,5 make the diagnosis.
Differential diagnosis Diobetes insipidis. Can produce polyuria, but this is not associatedwith a disorder of glucose control.
Management . Diabetes is managed with a host of treatments. Overall glucose ismanaged by proper diet, exercise, and medications to regulateglucose levels.
. Management of DKA and hyperosmolar hyperglycemic nonketoticcoma (HHNC).
. Pain from polyneuropathy is treated with standard medications forneuropathic pain.
. Cerebrovascular complications from diabetes mellitus (DM) arecommon, and Iargely include small-vessel ischemic disease.
Clinical course Most patients stabilize with improvement in glucose control andresolution of DKA and HHNC. Howevel long-term complications ofthe diabetes are inevitable.
r"I )irrlrt,lt,s Mt'llitrrs
kB,lE;Gv,
\ '**
\,wAnkle drop
Autonomicdysfunction
Extra ocular musclc paralysis(ptosis, strabismus, diplopia)
I )irrlrr,lcs Mr,llllrrs
Pupil lary abnormalities
Orthostatic\ hypotension
462 DISORDERS-ENDOCRINE DISORDERS-ENDOCRINE 465

r' I lryroi<l I )isolrk,r's
weakness,
and
THYROIO DI$ORDERS
Description Common and can present with cerebral or neuromuscular findirrgs
Pathophysiology . Thyroid pathology is diverse and both hyperthyroidism andhypothyroidism have neurologic manifestations.
. Hyperthyroidism can be caused by autoimmune, medication-related,neoplastic, and idiopathic disorders.
. Hypothyroidism can be caused by toxic, metabolic, autoimmune, antlidiopathic causes.
Hyperthyroidism
Clinical findings . Symptoms include nervousness, irritability, weakness, palpitations,fatigue, and weight loss.
. Thyrotoxic myopathy produces weakness that is mainly proximal, witlwasting of muscles of the shoulder girdle. Periodic paralysis candevelop. Myasthenia gravis also can be associated.
. Exam can show the weakness plus tachycardia, exophthalmos, hairloss, and increased sweating.
Laboratory studies . Routine labs usually are normal.
. Thyroid function tests usually show elevated T. and T, withsuppression of thyroid-stimulating hormone (TSH).
. lmaging is normal.
. Nerve conduction study (NCS) and electromyography (EMC) mayshow myopathic features.
Diagnosis . Hyperthyroidism is suspected when a patient presents with weaknestremor, and/or nervousness. Most patients with these symptoms willnot have a thyroid disorder, but this has to be considered.
. Thyroid function tests should be considered in patients presentingwith the neurologic complaints of tremor, irritability, memory loss, arweakness.
Management . Some of the symptoms of hyperthyroidism can be treated withmedications like B-blockers.
. Both radioactive iodine and thyroid surgery can reduce active thyroidhormone production.
Hypothyroidism
Clinical findings . Symptoms of hypothyroidism include weakness, fatigue, weight gain,depression, confusion, and irritability.
. Exam may show myopathy with weakness-most prominentlyproximally. Polyneuropathy is common. Ataxia with a cerebellarappearance can be seen. Decreased facial expression with motorfindings may suggest parkinsonism.
Laboratory studies . Routine labs usually are normal.
. Thyroid hormone levels typically are low with increased TSH.
. Imaging is normal, and often not needed.
464 DISORDERS-ENDOCRINE DISORDERS-ENDOCRINE 46'
I lypol hyroirllsln
I )r, rlin( )srs
M.rnagement
Ilryroirl I)isotrh,ts
llypollryrortlrsrn ollcrt is suspected whcn .t l).ttictlt l)r('s('tlts wtlllw(,(rlcl(.ss, l,rliguc, and weight gain.
Diagnosis is confirmed when thyroid function tests show dt:trt',tsltlthyroid hormones and increased TSH.
Replacement with thyroxine results in clinical improvement.
Long-term therapy is expected, with rapid worsening if treatmcrrt is
discontinued.

I ltyloirl I )isrrtrl(,t\,,urrrrrrr,,/
Hyperthyroidism
'i I ,"i,j.-,, -e"rrpi*tl.n -,S-'SFacial flushingI u( rdr ilu5rililB _______*l . "
Age I 2 tr r 50 ye.rrs 't ,.../usurllyt _----> -Palprble lymph nodes/
Muscle wasting--/ , -- ,.4''*-Warm, velvety skin
--T Palpilalion. tJ(hv( ardiJShoflnes: otbroalh/ -lz ., poor r(.(ponse to digiralis
Breastnnlrrgg6spt,_1, .__-- lntreasedappetileB)ne(rlm,l\ltd rn mdle ! -
;'15---::"-- Diarrhea
...'. .. (occasional)
-t . \Tr".r,ry\ \- . * Clubbing o[ iingers
.lvvarm, morst palms---=f \
{rl \
Loss of weight
Oligomenorheaor amenorrhea
Hypothyroidism
:--:- Exophthalmos(,olter
precordial pain (occasional)
.itril
Menonhagia(amenorrhea mayoccur late in disease)
H,i, a.. u,itrr. -ffi- ffi:,rui:;Jff "'
Fd::'i.:jJi:: K: ;Ll' I:,:-.:Tl"
Sensation ofcoldness -*-
Diminished I
yellowish (carotenemia),1!
Pulse slow ------.L
perspiration i
Skin coarse, dry,scaling, cold i
(follicular keratosis),
p
Weakness
Reflexes,prolonged
.if
ii\"i.
/'N"ru,,,,r,r,,r'I Erritahility
( Rertlcssn.ss
I Emorional instabiliry[lnsomn ia
I )r,,,( ill)lt()n
l ', r llroplrysiokrgy
ADRr:NArP_floRL( ,rrr rrrr lrrrlr' ,,,t,,lti.i"nay o, o
. tlyperodrenolism often is due to exogenously administeredcorticosteroids; however, Cushing's syndrome can develoP fromoversecretion by the adrenal gland.
. Hypoodrenalism (Addison's diseose) often is triggered by a seriousillness such as myocardial infarction (Ml), maior trauma, or sePsis.Withdrawal of exogenously administered corticosteroids is anothercommon cause.
Adrenol Excess
t linical features Patients with long-standing adrenal insufficiency have weakness,fatigue, hypertension, obesity, and skin striations. This results in a
typical cushingoid appearance.
Females have irregular menses and excess hair growth. Males havereduced libido.
i aboratory studies Measurement of blood cortisol level initially is performed. The mostspecific diagnostic test is the 24-hour urinary free-cortisol test.
Dexamethasone suppression test helps to differentiate excessiveproduction of adrenocorticotropin hormone (ACTH) from the Pituitaryvs. ectopic ACTH production-suppression suggests pituitary Productionwhereas ectopic ACTH-producing tumor is not suPpressed.
MRI of the pituitary is performed if a pituitary cause is susPected.
MRI or CT of the abdomen is performed if there is the possibility ofadrenal tumor-producing tumor. CT of the chest is performed ifectopic tumor is suspected with a lung origin.
Diagnosis Adrenal excess is suspected when a patient Presents with a cushingoidappearance, especially if they complain of weakness.
Management Treatment depends on the reason for the adrenal excess. Any one orcombination of surgery chemotheraPy, and radiation can be used.
Adrenol Insufficiency
Clinical features . Chronic adrenal insufficiency produces weakness, fatigue, anorexia,and weight loss. Hyperpigmentation also is seen, although it can bemissed as a complaint-unlike other causes, this hyperpigmentation is
prominent in pressured areas and skin folds.
. Other less common symptoms include hypotension, nausea, vomiting,diarrhea, and abdominal pain.
Laboratory studies . Cortisol is measured, but the ACTH stimulation test is standard.Patients with adrenal insufficiency do not respond to ACTH; thecorticotropin-releasing hormone (CRH) stimulation test is thenperformed. Primary adrenal insufficiency Patients have high ACTH
levels, but do not produce cortisol. Pituitary abnormalities result inabsence of an ACTH response. Hypothalamic defects result in delayedACTH response.
. MRI of the brain may be performed to look for destructive lesions ofthe hypothalamus or pituitary if indicated by the lab results.
Ar lr t,rrtrl I )isolrk'r's
466 DISORDERS-ENDOCRINE
recoveryr
r L*r/r, l' r'-t
DISORDERS-ENDOCRINE 467

[I Adrenol Dlsorders u',tthtte(t
Adrenal insufficiency is suspected when a patient presents withweakness and fatigue. Adrenal insufficiency is one of the diagnoses toconsider, in addition to hypothyroidism.
Cortisol levels and ACTH stimulation tests make the diagnosis ofadrenal insufficiency, with further testing to determine the cause.
Adrenol Insuf6clency
Administration of corticosteroids results in prompt improvement. Oralhydrocortisone can be used, although there are other preparations.
lf there also is mineralocorticoid deficiency from adrenal lesion,fludrocortisone also is given.
l,rt llrrls(buffakrhump)
Cushings (hyPercortisolism)
Moon face
ecchymoses
Darkeningof hair
Pigmentaccentuationat nipples,at frictionareas
Pigmentconcentrationin skin creasesand in
Adrenol Dlsorders m
Hypotension
Loss of weight,emaciation,anorexia,vomitin&diarrhea
Addison's (hypocortisolism)
4{tr
Skin pigmentation
468 DISORDERS_ENDOCRINEDISORDERS_ENDOCRINE 469






















![[Shinobi] Bleach 469](https://img.pdfslide.us/doc/110x75/568c47701a28ab49168ddcf9/shinobi-bleach-469.jpg)