Embed Size (px)
DESCRIPTION
Citation preview
![Page 1: [318 eth]](https://reader038.pdfslide.us/reader038/viewer/2022102813/5464124baf79598f6d8b49b5/html5/thumbnails/1.jpg)
Journal of Advanced Nursing, 1997, 25, 554–561
Ethnography: studying the fate of healthpromotion in coronary families
Rosemary M. Preston MSc RGN RM DipN DipEd RNT RCNT
Senior Lecturer, Faculty of Health Care and Social Studies, Luton University, Luton,England
Accepted for publication 20 March 1996
PRESTON R.M. (1997) Journal of Advanced Nursing 25, 554–561Ethnography: studying the fate of health promotion in coronary familiesThe concept of the ‘mindful body’, ‘coronary candidacy’ and ‘preventionparadox’ are three of many interesting themes explored in this paper whichexamines how, and to what extent, health information is received andtranslated into the daily domestic setting by coronary family groups. Taking anethnographic approach to collecting data highlights both the advantages anddisadvantages of this methodology in practice. Certainly, the emergence of ahealth promotion orientation in health care is an area which is intimatelyconnected to aspects of human culture and society that have long been a centralconcern of anthropologists. This mini-ethnography provides an anthropologicalunderstanding of the knowledge, beliefs and behaviours associated with heartdisease and its prevention. The concept of the ‘mindful body’ is provided as acritical interpretive approach to analysing the potential outcome of prescribedlifestyle changes, as given to coronary sufferers and their families during theperiod following coronary artery bypass surgery. Data drawn from this studyconfirms the evidence of lay epidemiology which works within the culturalfield of fate, luck and destiny, and which has interesting implications as to hownurses might plan for their health promotion strategies in the future.
The intent of this paper is to address this challengingINTRODUCTION
question by drawing on data from an ethnographic studycarried out in the South Buckinghamshire Hospital TrustHealth promotion is conceptualized by Tones (1986)
as any deliberate intervention which seeks to promote area, England (Preston 1993). The study set out to examinehow, and to what extent, the health informationhealth and prevent disease and disability. It incorporates
health education and gives prominence to the influence of advice given by the community cardiac support nurse wastranslated into their everyday domestic setting. Choosinglegal, fiscal, economic, and environmental measures on
commnunity health. In contemporary Britain, health pro- an ethnographic design proved to be an interesting experi-ence for the researcher. A critical examination of thismotion is increasingly seen as an emerging frontier within
its health care system and, as suggested by King (1994 approach to research is offered in this paper for those con-sidering ethnography as a design in the future.p. 209), offers an intriguing challenge to the nursing pro-
fession in particular. Certainly in specific areas of healthcare, like heart disease prevention and its management as
CONSIDERING AN ETHNOGRAPHICa chronic illness for life, nurses are in the frontline of
PERSPECTIVEattending to the health promotion needs of their client andassociated family groups. Whether this is in the acute The emergence of a health promotion orientation in health
care and the conceptual system that underpins it, is anhospital sector or in the community setting. However, aninteresting question is raised by Dines (1994 p. 219), who area which is intimately connected to aspects of human
culture and society that have long been a central concernasks, ‘What changes in health behaviour might nurseslogically expect from their health education work?’ of anthropologists. In its original usage, the ethnography
554 © 1997 Blackwell Science Ltd
![Page 2: [318 eth]](https://reader038.pdfslide.us/reader038/viewer/2022102813/5464124baf79598f6d8b49b5/html5/thumbnails/2.jpg)
Ethnography
technique in the then emerging discipline of anthropology supervised practice and a rigorous scholarly backgroundagainst which the trainee ethnographer, on return from thein the 19th century, the village or tribe, was its most
common level of application for studying people who field, can be debriefed and systematically assisted to con-struct the ethnography as an academic monograph so thatshared many similar and cultural characteristics (Geetz
1973). In contemporary health care matters, Kleinman reliability and validity of its method in practice can becritically appraised. Mackenzie (1994 p. 780) highlights(1992) reports ethnography as a method of enquiry, fast
becoming a fashionable choice where specific health the importance of this need by stating:care settings are considered to be the analogy of the village
There is no justification for ethnographers to ignore the generalor tribe. In this study, five family groups who had a coron-
rules of research reporting which include reliability and validity,ary sufferer in their midst were investigated in their own
and that no research in practice-based professions is worth thehomes where access to their health beliefs system, behav-
practitioners attention if threats to these key aspects have not beeniours and lifestyles that are normally obscured and dis-
addressed as rigorously as possible.torted by standard biomedical and epidemiological studies(see Maclean 1988, Beattie 1991, Bunton et al. 1991, If this type of research method is to be used appropri-
ately by the medical and nursing professions, and not withKelly et al. 1991), could be explored more effectively. Assuggested by Wilms & Best (1990 p. 392). the development of yet another ‘methodological fad’,
Kleinman (1992 p. 134) argues for the novice ethnographerIn contrast to the construct-driven studies of behavioural medi-
to be aware of the many difficulties of conducting a self-cine and behavioural science, this approach permits research to
anthropological study of this nature in practice. Hansonbe data-driven, particularly with regard to bodily and health
(1994) has also critically appraised this problem and sug-related experience and to the natural history of illness, health and
gests that the ethnographer requires an appreciation ofdisease experience.
insider bias when being an observer in their own culturalsetting. There is also a need to consider the effect of theUnfortunately though, some important research into
heart disease and health behaviour practices as identified researcher on the informants being studied, and the taking,recording, and analysis of field notes, with its inherentby Oliver (1992), have tended to take a reductionist
approach which focus on a limited number of practices problem of the interpreters bias at source. However, carry-ing out ethnography in your own culture has severallike smoking and eating fatty foods. Bunton et al. (1991)
and Caplan & Holland (1990) have both argued that this advantages which addresses the issue of access and famili-arity of the cultural setting which are inherently difficulthas given rise to a criticism of bias in health promotion
theory as a field of practice and enquiry. From an anthro- for the ethnographer to achieve when entering a ‘foreign’culture.pological perspective, it would appear that such criticisms
are not unfounded, and in many ways can be seen to rep-resent a disillusion with the medical model approach that
Ethics commitee approvalfocus on prescribed lifestyle changes without consideringthe mindful components that influence its fate. One of the hardest aspects posed for the ethnographer in
this study was gaining approval from the local ‘EthicsBunton et al. (1991) and other health behaviour re-searchers such as Hunt & Macleod (1987) have been critical Committee’ who were initially concerned with the intrus-
ive nature of the research methodology. It had to be arguedin their observations of methods used in health promotion,accusing them of holding a rather simplistic notion of how that, for the ethnography to be successful and deemed
credible, there was a need to develop an on-going relation-health knowledge is transmitted to the lay public. Tate &Cade (1990) confirm this underlying issue in health pro- ship with the informants for the flow of their lived experi-
ences to assist the contextual framework of analysis. Beingmotion strategy by discovering whilst lay health knowl-edge is high, misunderstandings concerning how, and to with the coronary families almost everday in their own
homes, and being involved in their daily activities, includ-what extent, health knowledge is being translated intoeveryday behaviour does occur. ing social occasions over an eight-week period, enabled a
description of the particular social context from which theIn this context, therefore, Maclean (1988), supports aproper appreciation of researching health behaviour data emerged, and an interpretation within it, of places,
people and other meaningful things; a form of datamatters through the use of an ethnographic approach.However, Kleinman (1992) draws our attention to concerns gathering that cannot be gained in isolated visits or in one
interview setting.about how health care professionals in particular are to betrained to practice competent ethnography in their own However, this posed a daunting prospect for the
researcher who conducted this study, and which requiredcultural health care settings. The classical ethnographerbeing viewed as someone who has to experience a trans- time, patience, and a good sense of humour, with a con-
scious effort not to approach these informants as a nurse,formation of being thrown into a new cultural setting, tobecome emersed in its ethos. This approach requires but as an anthropologist. Baillie (1995 p. 11) acknowledges
555© 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 554–561
![Page 3: [318 eth]](https://reader038.pdfslide.us/reader038/viewer/2022102813/5464124baf79598f6d8b49b5/html5/thumbnails/3.jpg)
R.M. Preston
the question of role conflict that nurses may encounter Using a grounded-theory approach (Glaser & Strauss1967) to data analysis, enabled coding of themes in thewhen conducting ethnography in this context, and
Hughes (1992 p. 444) critically appraises this dilemma by first round of interviews which could then be pursued inthe second and subsequent rounds. Through the use of anexplaining,ethnographic design, this data describes and interprets the
The ethnographer uses the senses of hearing, vision, smell andindividuals understanding of having heart disease in their
taste as much as cognition to characterize important physical andfamily and explores the mindful components that influ-
social features of a given field of human behaviour. Where phys-enced the fate of the prescribed lifestyle changes they had
icians, nurses and social workers centre their enquiring gaze onreceived.
the individual and his or her pathology, the ethnographer
describes and interprets the suffering of individuals as part of the
Mindful body conceptlived flow of interpersonal experiences and within the context of
the local moral worlds that encircle them.The ongoing contextual analysis utilized the heuristic con-cept of the ‘mindful body’ (Scheper-Hughes & Lock 1987Ethnographic studies are always difficult to conduct and
report on, and Mackenzie (1994 p. 775) correctly confirms p. 7) as a framework for understanding the relationshipbetween the physical, social and political body, and ofthe obscure nature of ethnography in research reporting.
This can cause difficulty for those practitioners who wish heart disease causation and prevention in coronary familygroups. The three bodies represent three separate and over-to assess the potential of ethnographic research for their
own practice, thereby restricting its value to the field of lapping units of analysis which considers phenomenology(lived-self, physical body), structuralism and symbolismnursing practice. However, as a methodology it provides
flexibility of method, allowing data to be collected from (the social body), and post-structuralism (the body politic).Drawing on data using this framework for analysis enableddifferent perspectives and by different methods.the fate of health promotion in these family groups to beexamined at both the macro and micro-level of analysis.
STUDYDouglas (1966) has argued convincingly that the body is
a complex structure which provides an opportunity to seeThis paper draws on data collected in extensive taped-field interviews in the informants own homes, including in the body a symbol of society and the powers and dangers
credited to social structure reproduced on the humanparticipant and non-participant observation of family lifeas and when it happened. Each family had a coronary body. Scheper-Hughes & Lock (1987) have extended these
arguments and challenge western assumptions about thesufferer in their midst and involved a total of 12 adults infive family homes. mind and body which may be detrimental to how health
care is planned for, and received, by its individual mem-bers in society. By proposing this framework, the body can
Studying families as cultural groupsbe examined from three separate but integrated perspec-tives that may help to increase our knowledge and under-As proposed by Helman (1991 p. 376), each family can be
regarded as unique small-scale society, with its own standing of the cultural aspects of health behaviourmatters.internal organization and view of the world. A crucial
aspect of each family culture involves those beliefs, behav-iours, habits, and lifestyles that are either protective of
THE PHYSICAL BODYhealth or pathogenic. The three primary informants wereselected at random from records held by the community The ways in which the body self is both received and
experienced in health and sickness is highly variable andcardiac support nurse who was responsible for facilitatingthe families awareness (see kinship chart), of heart disease an analysis of how the coronary sufferer and his family
experienced the notion of heart disease in their midstprevention and management in the weeks surroundingpreparation and recovery from coronary artery bypass sur- offers intriguing insight into the perceived conceptions of
the nature of their universe. This has implications for thegery. This approach to health promotion managementinvolved a structured programme which followed the concept of health promotion itself because how health
messages are received and experienced will determine its‘Active Heart’ type campaigns as indentified by Saunders(1989 p. 62). This campaign was a local initiative in the fate. Observations drawn from the data in this context,
highlight the informants dilemma in trying to achieve aSouth Buckinghamshire Hospital Trust area and followeda pattern of local news media coverage, information balance between their perceived health needs and enjoy-
ment of their lived daily experience. As Scheper-Hughesleaflets, individual/group counselling in their own homes,and a heart club for the coronary sufferer, where stress & Lock (1987) argue, an approach to health care which is
representative of the cartesian legacy reflects a mechanisticreducing workshops and participatory group exercisefacilitated positive health awareness. conception of how the individual body-self lives and
556 © 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 554–561
![Page 4: [318 eth]](https://reader038.pdfslide.us/reader038/viewer/2022102813/5464124baf79598f6d8b49b5/html5/thumbnails/4.jpg)
Ethnography
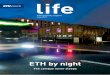
Figure 1 Chart showingkinship links of the threefamilies studied.
FAMILY A
Father (deceased–heart attack/52 y)Mother (deceased–stroke/80 y)
Brother (48 y)Brother (52 y)
Patient (58 y) and wife (52 y)(x 4 MIbypass surgery)
FAMILY B
Father (deceased–heart attack/84 y)Mother (deceased–heart attack/82 y)
Sister (56 y)and husband (61 y)+2 children aged40 y and 38 y Patient (65 y) and wife (58 y)
(x 2 MI andbypass surgery)
FAMILY C
Father (deceased–heart attack/42 y)Mother (deceased–heart attack/65 y)
Twin sister (32 y)Brother (29 y)
Sister (42 y) andhusband (41 y)+ 4 children aged16 y/12 y/11 y/3 y
Patient (32 y) and live-in partner (24 y)(x 4 MI andbypass surgery)
Son (22 y) Son (26 y)and wife (22 y)+ 2 childrenaged 2 y/8mths
Daughter (30 y)and husband (28 y)+ 3 childrenaged 10 y/8 y/2 y
Daughter (32 y)
Daughter (32 y)and husband (47 y)+ 3 children aged 12 y/8 y/2 y
Son (3 y)
functions. Thereby, a focus on so many of the physical for you than having regular meals... but,... don’t tell my dad that...he’ll go nuts!aspects of their previously preferred lifestyle when life-
style changes were prescribed, whilst ignoring the mindfulDaughter (family B): I try to do what’s right for my children, you
components of their beliefs as a separate and insignificantknow... make sure they get plenty of exercise... [pause]... but, I’m
problem, seemingly caused unnecessary anxieties.not sure that’ll be enough to protect them in the future. Me, well,
um, I’ve only recently started to look after myself. You see beingSon (family A): I don’t like to give it much thought. Since dad
had his operation he’s been fanatical with his diet and going to raised on the farm has meant I’ve always enjoyed my food, and
being a dairy farm you can guess what my diet consisted. Eventhe health club. He’s always joking with us that it gives him a
new lease on life and we should try it, but,... [pause]... um, I never when I married I still cooked the same way my mother had....
Since my husband had his last physical he’s been told to reducehave time. My wife can’t see any problems with what we do and
our friends feel the same way. None of us are overweight, we keep his cholesterol and its meant I’ve had to make a lot of changes to
how and what I cook. We’ve thought about becoming vegetarians,fit and we enjoy our lifestyle. The kids are happy enough, theyare allowed to eat when and what they want. I believe that’s better it’s something my eldest daughter wants to do, but I’m not sure
557© 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 554–561
![Page 5: [318 eth]](https://reader038.pdfslide.us/reader038/viewer/2022102813/5464124baf79598f6d8b49b5/html5/thumbnails/5.jpg)
R.M. Preston
that’s the answer. I’ve started to go swimming every week and I that balance which was often due to the many contradic-tions that life presented them with. This was frequentlytry not to use the car everyday, you know, walk to work instead.
But, that’s quite hard to do... [pause]... never enough time in the demonstrated by their understanding of their universebeing tense, fast, and full of chaos.day....
Data of this nature recurred many times in other inter- Sister (family C): If you’re asking me if I believe this is the resultviews and was also supported through observing how the of being stressed, I suppose I would have to say yes. You onlyfamilies interacted at mealtimes and other social gather- have to look around you to see how life is speeding up to realizeings. Often feelings of guilt were conveyed in their conver- that stress is a constant factor in our lives. Take my daughter forsations like, ‘Don’t you know coffee is bad for you’, or, ‘Go example. I don’t want her to get pregnant whilst she is still aton have another, it won’t do any harm’. Observations of school... but, um, the pressures on her are quite frightening. Ifamily interactions like these support a tendency for health worry she’ll become a victim and...messages to incur an artificial level of imposed anxiety
Sufferer (family A): I’ve managed to give up smoking but my wifewhich leads to a separation of their lived-self from the flowhasn’t. We’ve come to an agreement she doesn’t light up whenof their daily routine and from the social context in whichI’m in the same room but she’s often anxious about one thing orthey would normally function. How food was cooked wasanother and then forgets,... what can you say?another area where this was highlighted and often when
explored with the informants, rationale was given to the Scheper-Hughes & Lock (1987) note these contradictionseffect, ‘Well we’ve always done it this way or, I was told and tensions as being an integral part of Western cos-to stop frying food so now I cook in the oven’ (despite the mology. How an individual self entertains notions aboutobserver noting the food was still cooked in a high amount his body in its relationship to the environment, includingof fat). external and internal perceptions, memories, affects, cog-
The following is an extract from the researchers own nitions, and actions, is an important contribution to howdiary: his lay health knowledge, beliefs and behaviours are con-
structed. Body image is one important component of theWe had had a good discussion virtually all morning. Wife (familylived-body-self experience, as it confirms to the individualA) had been most illuminating about how she had made a con-the social and cultural meanings of what it is to be human,scious effort to change her style of cooking from frying to grillingand provides a framework for them to base their lay epi-or cooking in the oven following a chat she had had with thedemiology that explains their sickness or health status.cardiac support nurse. There were tales about what her cookingDavison et al. (1991 p. 7) draws our attention to the notionwas like when they first got married with her husband chippingof ‘coronary candidacy’ as belonging to the area of lay epi-in every so often when he wasn’t being distracted by his energeticdemiology related to body image perception. In this study,grandson. I found myself being coerced into staying for lunch. Itinformants held specific images of the person they thoughthad not been my intention, but I was cold and felt quite hungrymost likely to suffer from heart trouble.and the smells coming from the kitchen had been too inviting.
Although we had spent most of the morning in the conservatoryWife (family A): I’ve always known Dave to be a fit man. [laughs]
because of the rain, wife A had flitted in and out of the kitchenYes much fitter than me. I’ve always been too tubby for my own
to prepare the lunch and I was only too willing to set the tablegood and I know I smoke too much.
for the four of us as she prepared to dish-up. The oven door
opened and I was surpised to see fish steaks covered in a bubbly Sister (family C): Being a postman I thought would be the fittest
job he could have. All that walking with the postal rounds well,...batter, floating in boiling oil on one shelf and a tray of noisette
potatoes also floating in oil on the other shelf. Peas were drained um, who’d have thought he’d get so sick. Now me yes. As you
can see, I smoke too much and I eat too much. It’s what I do toand a knob of Flora margarine was dropped onto its pile anddespite my initial surprise I eagerly tucked into this satisfying get by [shrugs her shoulders].
meal. Somehow though, this observation contradicted with what
I had heard all morning... interesting!Conflict
Such imagery is a seemingly collective activity which isMessages chosen
facilitated by mass media and official bodies, as well asfriends, family and work colleagues. The informants inSuch observations imply that whilst health knowledge is
high, the coronary families choose which health messages this study often referred to their own observations in thiscontext and often cited celebrities (Michael Heseltinethey can comfortably identify with and disregard the rest.
This has implications for health promotion strategies, (member of parliament) and James Hunt (racing driver))who had recently been afflicted, in their attempt to ration-because it seems achieving a balance in any lifestyle is
very important to the individual self. However, the data alize the image they had of a typical heart attack victim.However, it was clearly evident they encountered ahere highlights how individuals had difficulty in achieving
558 © 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 554–561
![Page 6: [318 eth]](https://reader038.pdfslide.us/reader038/viewer/2022102813/5464124baf79598f6d8b49b5/html5/thumbnails/6.jpg)
Ethnography
conflict in their understanding of heart disease causation within the cultural fields of luck, fate and destiny. A cogni-tive process which offers a rational way of incorporatingand often asked, ‘Why me?’ Certainly, the tensions and
contradictions presented by the coronary families’ under- potentially troublesome information and results in apotential barrier to the aims of health promotion strategy.standing of their cosmology and the constructed imagery
of the ‘coronary candidate’ emphasizes the real dilemma This part of the analysis, therefore, highlights the need forconducting assessment of health promotion strategyof a ‘prevention paradox’ occuring. Rose (1985 p. 37)
explains that this, as a preventative measure which brings within a broader cultural framework, if desired outcomesfor health disease prevention are to be achieved.much benefit to the population, offers little to each partici-
pating individual. Assuming heart disease causation to be When considering a cultural perspective within a nurs-ing assessment, as advocated by both Anderson (1987) andmultifactorial, but which in many ways, as Oliver (1992)
reminds us, must be considered unknown, there are no Leininger (1990), respectively, one should begin to addressboth the emic (insider) and etic (outsider) viewpoints ofguarantees that altering ones lifestyle will prevent heart
disease. That is assuming you were a candidate in the first both the clients and nurses own beliefs system in this con-text. The data suggests that the coronary families’ percep-place. The informants perception of what they consider to
be a ‘coronary candidate’ seriously undermines the success tion of heart disease causation is in direct contrast to theprevailing orthodoxy of contemporary health promotionpotential of any health promotion strategy if lay health
beliefs are not identified and explored individually in practice. This is important for nurses to acknowledgewhen considering their own role as health promotionthis context.strategists.
THE SOCIAL BODYTHE BODY POLITIC
The second level of analysis considers the representationaluses of the body as a natural symbol with which to think As argued by Scheper-Hughes & Lock (1987), the relation-
ship between the individual and social bodies concernabout the nature of health behaviour practices in coronaryfamilies. As Douglas (1970 p. 65) observes more than metaphors and collective representations of the
natural and collective order. It is also about power andThe body is a natural symbol supplying some of our richest control of threats and regulation of individual and groupsources of metaphor. These may be used as a cognitive map to boundaries. For example, the overall shape of health pro-represent the natural, supernatural, social and even spatial motion policies and the way they have been oper-relations that are experienced in everyday language and functions. ationalized, swinging from the most fundamental pole of
social theory and political action, between individualisticA symbolic anthropology takes the experiences of theand collectivist modes of intervention, between paternal-body as a representation of society itself. A failure to seekistic imposed and consultatory participatory forms of auth-out the individual’s true understanding of heart diseaseority, demonstrate the nature of these barriers. Certainlycausation as this study has attempted to do, ignores a natu-the ‘Active Heart’ campaign takes on the form of collectiveral and supernatural set of beliefs held by families in con-and consultative participatory approach to health pro-temporary Britain. In this respect, frequently quotedmotion strategy which involves the whole community notmetaphors such as, ‘he can’t unwind’ were noted in thejust the coronary sufferers themselves.context of everday language. Usage of the cultural fields
of luck, fate and destiny also figured prominently as super-natural metaphors which exemplified their inability to Threatidentify a causal link for the heart disease afflicting their
In this study, the informants believed that the issue offamily group.lifestyle causality factors was imposed as a threat to them
Wife (family A): It seems anyone can be at risk, um, I mean look (meaning their heart) by those seen to be in power andat us. Who’d have thought we’d have this problem.... No, I look control of their care, namely, the cardiac support nurseat my family and I think we’ve been unlucky. I just hope and pray and the cardiac consultant.my kids will be alright.
Sufferer (family A): I just can’t accept I’m sick and [pause] well,Daughter (family B): Having heart disease in the family is quite I’ve always been a keep-fit fanatic, even if I have been naughtyscary you know, but [pause]... um, I don’t believe you can do with the booze and other things sometimes, but it don’t seemmuch to prevent it happening. It’s the same with cancer. If it’s right. I’m told I have 10 years following this op but less if I don’tyour turn to get it then there’s not much you can do about it. change the way I live.... Some choice eh?
Sister (family C): My doctor says my cholesterol is normal so IThis finding is very similar to Davison et al.’s (1991),who concluded that lay epidemiology readily accommo- don’t have to worry too much. What does he know? Having a
heart attack at 30 is something you don’t expect to happen. Fordates offical messages concerning health behaviour risks
559© 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 554–561
![Page 7: [318 eth]](https://reader038.pdfslide.us/reader038/viewer/2022102813/5464124baf79598f6d8b49b5/html5/thumbnails/7.jpg)
R.M. Preston
two years my brother kept saying he didn’t feel right, what didDISCUSSION
the doctor do? Nothing! Now he’s been told to change his lifestyle.
Talk about calling the kettle black. Teaching others about health and lifestyle practices needsto involve an appreciation of the lay person’s current
When the sense of social order is threatened in this way, beliefs which are situated within the context of their dis-boundaries between the individual and body politic tinctive ways for dealing with sickness, disability and thebecome blurred and the symbols of self-control intensified danger of death. As this study has shown, consideringthrough an increased need for ritual and acts of purifi- heart disease and risk behaviour practice within the ana-cation (Scheper-Hughes & Lock 1987). For example, the lytical frame of the ‘mindful body’ offers intriguing insightActive Heart Club can be seen as a developing community- into the fate of health promotion in coronary familybased ritual which functions as a self-help group for coron- groups. Certainly, a confirmation of Davison et al.’s (1991)ary sufferers. This ritual appears to create social distance earlier findings of the operation of a lay epidemiology dem-and a sense of control and security for these informants. onstrates the difficulty all health promoters face whenSufferer B comments on his experiences when visiting engineering their strategies to the point where healththe club: knowledge can be translated successfully into the dom-
estic setting. This raises the interesting question of whySufferer (family B): We’re told to rest.... There are about eight of family beliefs systems persist despite an input of newus here this evening and we all sit in a circle and have a chat health knowledge being present?about anything and everything. It was certainly nice to feel relaxed Certainly, the phrase risk behaviour has gained promi-after our strenuous aerobic workout. Questions are raised and nence in the dialogue of health promotion to the point thattaken up by anyone who has had some experience of that problem. it has ruled the planning of health campaigns over theThere is a quiet feeling of reassurance, a sense of sharing and years. From a cultural perspective though, it can bebelonging. acknowledged that many people do endanger their lives
and are constantly exposed to health threats which theydeem beyond their immediate control. This is despite con-Ritual of family get togetherstemporary research highlighting health knowledge to be
Those individuals who did not attend the club preferred high in the general population (Tate & Cade 1990, Hartinstead to utilize rituals of family get togethers to control 1990). By drawing on a mini-ethnographic perspective,their bodies in times of crisis. this study has examined family culture in the domes-
tic setting with a view to identifying those patterns ofSufferer (family A): We’re all close as families go. As you know,
behaviour which are protective of health, or pathogenic.all my kids except one are married and live locally. We tend to
There is evidence here to suggest the operation of a ‘pre-live out of each others pockets. It seems right somehow. I’ve
vention paradox’, based on the informants professed opi-always kept us close. You see we never have individual problems
nion that heart disease was to some extent preventable oras such. If any of us are suffering, we all suffer.... It’s our way.
postponable — the idea that it could happen to anyone atYou saw us last time, sitting around the table for an evening meal
anytime was omnipresent. This has serious implicationstogether. We didn’t do that because we knew you were coming.
as to what changes in health behaviour nurses can logicallyNo, its something we do regular. We sit around and talk like about
expect from their health education work. For families, pat-anything and everything that’s bothering us.
terns of risk behaviour may, as this study has shown, behighly acceptable in the moral worlds that encircle theHow individuals and family groups utilize rituals tocoronary sufferers and their families. Developing assess-help control their bodies in crisis might offer the healthment strategies which include a cultural perspective to thepromotion strategist insight into planning a struct-problem of lifestyle adopted practices, may be one wayured framework of support when lifestyle changes areforward for the nurse health promoter of the future.prescribed. As Helman (1990 p. 192) explains,
All rituals are an important part of the way that any social group CONCLUSIONcelebrates, maintains or renews the world in which they live.
By studying family culture, as this study has attempted todo, the value of conducting an ethnography that providesCertainly, during the most difficult period of discovering
they had a coronary sufferer in their midst, and during the a detailed account of peoples lives and the ways they makesense of their world as part of the flow of their lived-bodytransition phase that encompassed their adoption of new
lifestyle practices, the rituals of the heart club and family experience has hopefully been highlighted. The appli-cation of this approach, as Baillie (1995) so rightly ident-get-togethers provided these individuals with a strong
sense of cultural order imposed on, and superior to, the ifies, is not without its problems. However, it can facilitatethe development of meaningful knowledge and a theorychaos that this situation had afflicted them with.
560 © 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 554–561
![Page 8: [318 eth]](https://reader038.pdfslide.us/reader038/viewer/2022102813/5464124baf79598f6d8b49b5/html5/thumbnails/8.jpg)
Ethnography
Hughes C.C. (1992) Ethnography: what’s in a word — process?base for nursing practice, where an understanding of theproduct? promise? Qualitative Health Research 2(4), 439–450.lay epidemiology that operates in the cultural fields of
Hunt S.M. & McCleod M. (1987) Health and behaviour change:luck, fate, and destiny can be acknowledged to be a fac-some lay perspectives. Community Medicine 9(1), 68–76.tor influencing the fate of health promotion in the daily
Kelly R.B., Zyzanski S.J. & Alemagno S.A. (1991) Prediction ofdomestic setting.motivation and behaviour change following health promotion:role of health beliefs, social support and self-efficacy. SocialScience and Medicine 32(3), 311–320.References
King P.M. (1994) Health promotion: the emerging frontier inAnderson J.M. (1987) The cultural context of caring. Canadian nursing. Journal of Advanced Nursing 20, 209–218.
Critical Care Nursing Journal 4(4), 7–13. Kleinman A. (1992) Local worlds of suffering: an interpersonalBaillie L. (1995) Ethnography and nursing research: a critical focus for ethnographers. Qualitative Health Research 2(2),
appraisal. Nurse Researcher 3(2), 5–21. 127–134.Beattie A. (1991) Knowledge and control in health promotion: a Leininger M.M. (1990) Importance and uses of ethnomethods, eth-
test case for social policy and social theory. In The Sociology nography and ethnonursing research. In Recent Advances inof the Health Service (Gabe J. ed), Routledge, London. Nursing: Research Methodology (Cahoon M.C. ed), Churchill
Bunton R., Murphy S. & Bennett P. (1991) Theories of behavioural Livingstone, Edinburgh.change and their use in health promotion: some neglected areas. Mackenzie A.E. (1994) Evaluating ethnography: considerations forHealth Education Research 6(2), 153–162. analysis. Journal of Advanced Nursing 19, 774–781.
Caplan R. & Holland R. (1990) Rethinking health education theory. Maclean U. (1988) Ethnographic approaches to health. In HealthHealth Education Journal 49(1), 10–16. Behaviour Research and Health Promotion (Anderson J.M. ed.),
Davison C., Smith G.D. & Frankel S. (1991) Lay epidemiology and Oxford University Press, Oxford, pp. 41–45.the prevention paradox: the implications of coronary candidacy Oliver M.F. (1992) Doubts about preventing coronary heartfor health education. Sociology of Health and Illness 13(1), disease. British Medical Journal 304, 393–394.1–19. Preston R.M. (1993) Mindful Bodies and Diseased Hearts: the
Dines A. (1994) What changes in health behaviour might nurses Fate of Health Promotion in Coronary Families. MSc thesis,logically expect from their health education work? Journal of Department of Social Science, Brunel University, Uxbridge.Advanced Nursing 20, 219–226. Rose G. (1985) Sick individuals and sick populations.
Douglas M. (1970) Natural Symbols. Vintage, New York. International Journal of Epidemiology 14, 32–38.Douglas M. (1966) Purity and Danger. Praeger, New York. Saunders R. (1989) Look after your heart: heartbeat award scheme.Geetz C. (1973) The Interpretation of Cultures. Basic Books, Health Trends 2(21), 62.
New York. Scheper-Hughes N. & Lock M. (1987) The mindful body: a pro-Glaser B.G. & Strauss A.L. (1967) The Discovery of Grounded legomenon to future work in medical anthropology. Medical
Theory. Weidenfeld and Nicholson, London. Anthropology Quarterly 1(1), 6–41.Hanson E.J. (1994) Issues concerning the familiarity of researchers Tate J. & Cade J. (1990) Public knowledge of dietary fat and coron-
with the research setting. Journal of Advanced Nursing 20, ary heart disease. Health Education Journal 49(1), 32–35.940–942. Tones B.K. (1986) Health education and the ideology of health
Hart J.T. (1990) Coronary heart disease: preventable but not promotion: a review of alternative approaches. Healthprevented? British Journal of General Practice 40, 441–443. Education Research 1(1), 3–12.
Helman C. (1991) The family culture: a useful concept of family Wilms D.G. & Best J.A. (1990) A systematic approach for usingpractice. Family Medicine 23(5), 376–381. qualitative methods in primary prevention research. Medical
Helman C. (1990) Culture Health and Illness 2nd edn. Wright, Anthropology Quarterly 4(4), 391–409.Oxford.
561© 1997 Blackwell Science Ltd, Journal of Advanced Nursing, 25, 554–561