Embed Size (px)
Citation preview
Genetic Marker (s) Of MI – One, One Hundred, or One Thousand?!
Provided by:
M. Bidya Sagar, Ph.D.Structural Biology and Drug Discovery Laboratory
Center for Vulnerable Plaque ResearchTexas Heart Institute
Editorial Slides VP Watch – December 26, 2002 - Volume 2, Issue 51

Rupture prone vulnerable plaques are the predominant underlying process in the pathogenesis of acute coronary syndromes.
Although the morphology of these vulnerable plaques has been studied extensively, the underlying genetic markers of these plaques and patients in whom vulnerable plaque develop, suffer a fatal cardiovascular event, are largely unknown.

• Genomic and Proteomic research may shed light on the way to discover these markers of plaque/patient vulnerability.
• Human Genome studies are underway to identify:
– differential expression of up- and down-regulated genes in plaque vs normal arterial walls, and comparison of the mRNA expression at different stages of plaque development.
– single nucleotide polymorphism (SNP) among cardiovascular disease patients vs. normal subjects.
– loci on chromosomes through linkage studies

Several studies compared the gene expression of :
• activated human umbilical vein endothelial cells
• vascular smooth muscle cells
• cholesterol-loaded macrophages with that of nonactivated cells.1-3
1-Gene Expression Studies in Plaque

Studies in cell lines revealed differential regulation of genes involved in leukocyte trafficking, cell-cycle control, and apoptosis.
Differences in gene expression have been observed among fatty streaks and advanced lesions 4 and intima and media of human atherosclerotic plaques. 5
1- Gene Expression Studies in Plaque

Tyson et al studied heterogeneity of gene expression in human atheroma using cDNA analysis. 6
Faber et al have suggested perilipine, as well as other genes potentially involved in rupture of human atherosclerotic plaques.7-8
1- Gene Expression Studies in Plaque
Genetic-linkage studies 11 and candidate gene analyses 12-16 have implicated a locus and several genes related to predisposition to myocardial infraction.
A linkage analysis for myocardial infarction and its related risk factors was carried out by Broecke et al. 11
2- Genetic Linkage Studies
They have scanned the whole genome in 513 families to identify chromosomal regions linked to MI
They showed the risk of MI maps to a single region on chromosome 14 with a significant lod score of 3.9 (pointwise P=0.00015, genome-wide P<0.05).
2- Genetic Linkage Studies
Human Genome mapping has led to a massive search for clinically relevant genomic information: including (SNPs), which consist of substitutions of one nucleotide for another in a DNA sequence.
Human genomes are 99.9% identical with only 0.1% of the genome showing polymorphisms.9-10
3- Gene Polymorphism (SNP) Studies
About 2-3 million SNPs have been found in exonic, intronic, regulatory, and intergenic regions.9-10
Though almost all genes contain SNPs, only a minority of SNPs result in amino acid variation in proteins. 9-10
3- Gene Polymorphism (SNP) Studies

Myocardial infarction is a complex multifactorial and polygenic disorder; and therefore, it may not be possible to find an specific genetic make-up predicting the disease.
Genetic polymorphisms have been associated with myocardial infarction and angina pectoris. 20
3- Gene Polymorphism (SNP) Studies

Fu L et al., investigated the association between gene polymorphism of the plasminogen activator inhibitor-1 (PAI-1) and MI in a Chinese population.17
The 5A/6A polymorphism in the promoter of the stromelysin gene has been identified as a novel pathogenetic risk factor for MI. 18
Polymorphisms of the P-selectin gene and risk of MI in men and women has been reported.19
Gene Polymorphism (SNP) Studies

As reported in VP Watch of this week, Yamada et al., published in the New England Journal of Medicine, discovery of new polymorphisms in candidate genes that confer susceptibility to myocardial infarction. 20

Method:
A fluorescence- or colorimetry-based allele- specific DNA-primer-probe assay
To determine Genotypes of 112 polymorphisms of 71 candidate genes in 2819 unrelated Japanese patients with MI (2003 men and 816 women) and 2242 unrelated Japanese controls (1306 men and 936 women).

Results:
Screening of the 112 polymorphisms for an association with MI in 909 subjects.
19 polymorphisms were selected in men and 18 in women by means of logistic-regression analysis, after adjustment for age, BMI, the prevalence of smoking, etc.
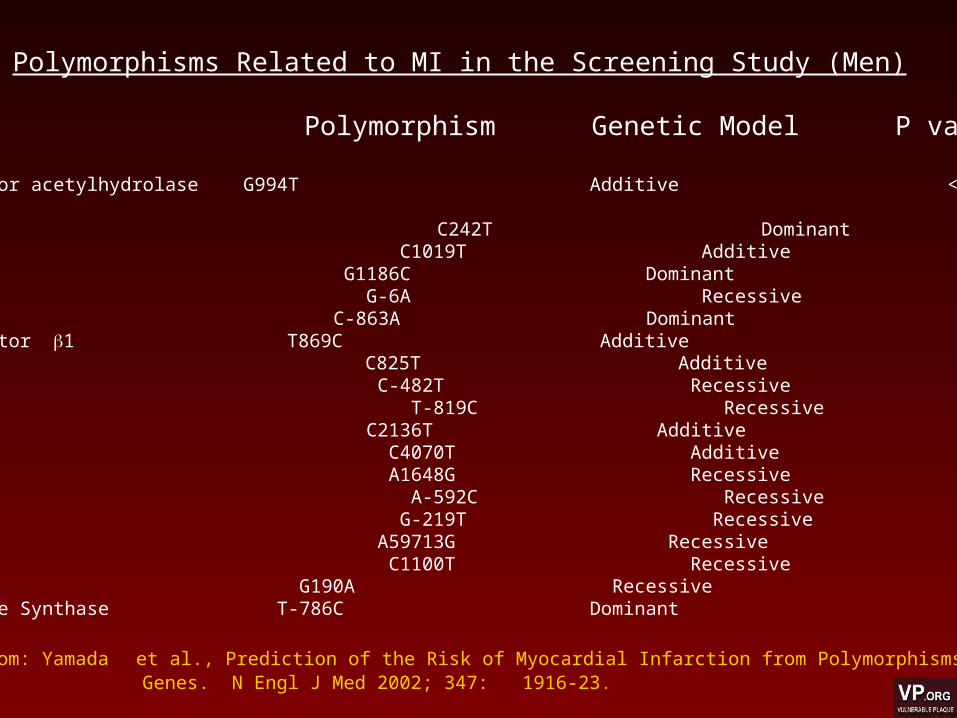
Polymorphisms Related to MI in the Screening Study (Men)
Gene Polymorphism Genetic Model P value Platelet-activating factor acetylhydrolase G994T Additive < 0.001
p22phex C242T Dominant 0.006 Connexin 37 C1019T Additive 0.007 Thrombospondin 4 G1186C Dominant 0.013 Angiotensinogen G-6A Recessive 0.019 Tumor necrosis factor C-863A Dominant 0.045 Transforming growth factor 1 T869C Additive 0.049 G protein 3 subunit C825T Additive 0.051 Apolipoprotein C-III C-482T Recessive 0.057 Interleukin-10 T-819C Recessive 0.061 Thrombomodulin C2136T Additive 0.065 Apolipoprotein E C4070T Additive 0.074 Glycoprotein 1a A1648G Recessive 0.080 Interleukin-10 A-592C Recessive 0.088 Apolipoprotein G-219T Recessive 0.092 Thrombopoietin A59713G Recessive 0.094 Apolipoprotein C-III C1100T Recessive 0.095 CC Chemokine receptor 2 G190A Recessive 0.097 Endothelial Nitric Oxide Synthase T-786C Dominant 0.098
Adopted from: Yamada et al., Prediction of the Risk of Myocardial Infarction from Polymorphisms in Candidate Genes. N Engl J Med 2002; 347: 1916-23.
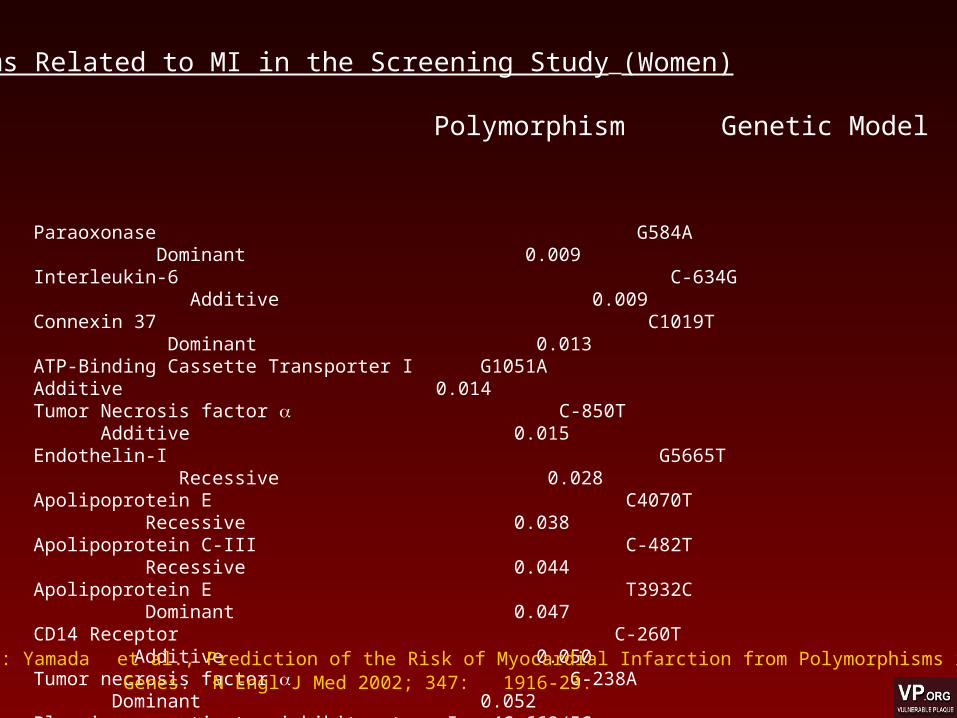
Paraoxonase G584A Dominant 0.009Interleukin-6 C-634G Additive 0.009Connexin 37 C1019T Dominant 0.013ATP-Binding Cassette Transporter I G1051A Additive 0.014Tumor Necrosis factor C-850T Additive 0.015 Endothelin-I G5665T Recessive 0.028Apolipoprotein E C4070T Recessive 0.038Apolipoprotein C-III C-482T Recessive 0.044Apolipoprotein E T3932C Dominant 0.047CD14 Receptor C-260T Additive 0.050Tumor necrosis factor G-238A Dominant 0.052Plasminogen-activator inhibitor type I 4G-668/5G Recessive 0.055Fatty-acid-binding protein 2 G2445A Additive 0.057Insulin receptor substrate-I G3494A Dominant 0.058Stromelysin-I 5A-1171/6A Additive 0.072Glycoprotein Ib C1018T Additive 0.072E-selection A561C Dominant 0.074
Polymorphisms Related to MI in the Screening Study (Women)
Gene Polymorphism Genetic Model P value
Adopted from: Yamada et al., Prediction of the Risk of Myocardial Infarction from Polymorphisms in Candidate Genes. N Engl J Med 2002; 347: 1916-23.

Distributions of Polymorphisms Associated with MI amongamong the 4152 Subjects in the Large-Scale Study
Gene and polymorphism Controls Patents with MI in %Men (n=2858)Connexin 37, C1019T at lp35.1 C/C 71.7 66.2 C/T 25.4 29.6 T/T 2.9 4.2 p22phex , C242T at 16q24 C/C 75.9 80.7 C/T 22.5 17.9 T/T 1.5 1.4Women (n=1294)Plasminogen-activator inhibitor type 1 4G-668/5G at 7q21.3-q22 4G/4G 44.8 36.5 4G/5G 44.9 50.9 5G/5G 10.3 12.6Stromelysin-1, 5A-1171/6A at 11q23 5A/5A 5.7 1.2 5A/6A 31.3 28.1 6A/6A 63.0 70.8
Adopted from: Yamada et al., Prediction of the Risk of Myocardial Infarction from Polymorphisms in Candidate Genes. N Engl J Med 2002; 347: 1916-23.
In men, MI was significantly associated with the C1019T polymorphism in the connexin 37 gene (P<0.001).
In women, the 4G-668/5G polymorphism in the plasminogen-activator inhibitor type 1 gene P<0.001) and the 5A-1171/6A polymorphism in the stromelysin-1 gene (P<0.001) were associated with MI.

Conclusions:
Determination of the genotypes of connexin 37,plasminogen-activator inhibitor type 1,and stromelysin-1 genes may prove reliable in predicting the genetic risk of MI.

Questions:• Knowing that 2-3 million gene polymorphisms (SNP) exist, how many different SNPs do you expect to be identified as risk markers of arteriosclerosis and MI: >10 or >100 or >1000?
• Could there be certain polymorphisms that protect people against atherosclerosis? Or protect atherosclerotic subjects from developing myocardial infraction?
• Is it likely to find major gene polymorphisms that could be responsible for 50-70% of MI (like the 5 major traditional risk factors)?
• Is it likely that there are numerous polymorphisms, each statistically significant, in different populations?
• How closely do these genetic polymophisms
translate to functional proteomic variations?
Questions:

References
1.) Lu KP, Ramos KS. Identification of genes differentially expressed in vascular smooth muscle cells following benzo[a]pyrene challenge: impli-cations for chemical atherogenesis. Biochem Biophys Res Commun. 1998; 253:828 –833. 2.) de Vries CJ, van Achterberg TA, Horrevoets AJ, ten Cate JW, Pannekoek H. Differential display identification of 40 genes with altered expression in activated human smooth muscle cells. Local expression in athero-sclerotic lesions of smags, smooth muscle activation-specific genes. J Biol Chem. 2000;275:23939 –23947. 3.) Shiffman D, Mikita T, Tai JT, Wade DP, Porter JG, Seilhamer JJ, Somogyi R, Liang S, Lawn RM. Large scale gene expression analysis of cholesterol-loaded macrophages. J Biol Chem. 2000;275:37324 –37332. 4.) Hiltunen MO, Niemi M, Yla-Herttuala S. Functional genomics and DNA array techniques in atherosclerosis research. Curr Opin Lipidol. 1999;10: 515–519. 5.) McCaffrey TA, Fu C, Du B, Eksinar S, Kent KC, Bush H Jr, Kreiger K, Rosengart T, Cybulsky MI, Silverman ES, Collins T. High-level expression of Egr-1 and Egr-1-inducible genes in mouse and human atherosclerosis. J Clin Invest. 2000; 105:653– 662. 6.) Tyson k.L., et al., Heterogeneity of gene expression in human atheroma unmasked using cDNA representational difference analysis. Physiol Genomics. 2002: 9(2):121-30 7.) Faber BC et al., Identification of genes potentially involved in rupture of human atheroserotic plaques. Circ Res., 2001: Sept 14:89(6):547-54. 8.) Faber BC et al., Genes potentially involved in plaque rupture. Curr Opin Lipidod. 2002. Oct;13 (5):545-52. 9 ) Ross R. Atherosclerosis: an inflammatory disease N Engl J Med. 1999; 340:115–126. 10.) Libby P. Changing concepts of atherogenesis. J Intern Med. 2000;247: 349–358. 11.) Broeckel U, Hengstenberg C, Mayer B, et al. A comprehensive linkage analysis for myocardial infarction and its related risk factors. Nat Genet 2002;30:210-4. 12.) Cambien F, Poirier O, Lecerf L, et al. Deletion polymorphism in the gene for angiotensin-converting enzyme is a potent risk factor for myocardial infarction. Nature 1992;359:641-4. 13.) Weiss EJ, Bray PF, Tayback M, et al. A polymorphism of a platelet glycoprotein receptor as an inherited risk factor for coronary thrombosis.N Engl J Med 1996;334:1090-4. 14.) Iacoviello L, Di Castelnuovo A, de Knijff P, et al. Polymorphisms in the coagulation factor VII gene and the risk of myocardial infarction. N Engl J Med 1998;338:79-85. 15.) Kuivenhoven JA, Jukema JW, Zwinderman AH, et al. The role of a common variant of the cholesteryl ester transfer protein gene in the progression of coronary atherosclerosis. N Engl J Med 1998;338:86-93 16.) Ellsworth DL, Manolio TA. The emerging importance of genetics in epidemiologic research. II. Issues in study design and gene mapping. Ann Epidemiol 1999;9:75-90 17.) Fu L et al., Relationship between gene polymorphism of the PAI-1 promoter and myocardial infraction. Chin Med J (Engl) 2001. 1 Mar;114(3):266-9 18.) Tarashima M et al., Stromelysin promoter 5A/6A polymorphism is associated with acute myocardial infarction. Circulation 1999 Jun 1;99(21):2717-9 19.) Kee F et al., Polymorphisms of the P-selectin gene and risk of myocardial infarction in men and women in the ECTIM extension study. Etude cas-temoin de l'infarctus myocarde. Heart. 2000 Nov;84(5):548-52 20.) Yamada, Y et al., Prediction of the Risk of Myocardial Infarction from Polymorphisms in Candidate Genes. N Engl J Med 2002; 347: 1916-23.





























