Embed Size (px)
Citation preview

“Introduction of Volumetric Capnography
One Hospital’s Experience”
Presented By: Michael Powers, MS, RRT
Director, Lung CenterUniversity of Tennessee Medical Center
Knoxville, Tennessee

Agenda:
VCO2 ManagementClinical ApplicationsUniversity of Tennessee Medical Center’s
Experience and DataOther Hospital’s Outcome Data

VCO2 Management
1. Why to use
2. How to use

Monitoring CO2 Elimination • VCO2 provides continuous feedback regarding
ventilation and perfusion Relationship between PaCO2 and VCO2 is
inverse and consistent Instant feedback when making ventilator
setting changes:• Did perfusion change?• Did ventilation change?• With PaCO2 from an ABG, you can answer the
question, “Did Vd/Vt change?”

Metabolism(CO2 Production)
CO2 Elimination(VCO2)
PaCO2
VCO2 - A Few Basics
Things that affectCO2 elimination
Circulation
Diffusion
Ventilation
1 2

CO2 Elimination(VCO2)
Why Measure VCO2?
Very Sensitive Indicator of
PATIENT STATUS CHANGE Early Indicator Future Changes in
PaCO2
Another Tool to Assist in
Determining When to Draw a Blood
Gas Reduces the # of ABGs
VCO2 - A Few Basics
3

Volumetric Capnography
Integration of Flow & CO2

The integration of CO2 and Flow provides an easy method to obtain previously difficult to obtain parameters VCO2 = CO2 Elimination Airway Deadspace, Physiologic VD/VT Alveolar Ventilation Cardiac Output
Integration of Flow & CO2
EtCO2 CapnogramRespiratory Rate
Capnography Volumetric CO2
CO2 EliminationAirway DeadspaceAlveolar VentilationPhysiologic Vd/Vt

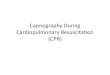
Phase I – Airway Gas
The waveform is divided into three phases:The waveform begins at the onset of expiration. Imagine that you are the sensor sitting in the proximal airway. The first gas past the sensor at onset of expiration does not contain any CO2 but does have volume. The graph shows movement along the X-axis (exhaled volume) but no gain in CO2 (Y-axis).
This volume is entirely from the conducting airways - no gas exchange has taken place.
Phase I represents pure airway gas.

Phase II – Transitional Gas
Phase II represents gas that is composed partially of airway volume and partially from early emptying alveoli (fast time constant).
At about generation 17 of the airway tree we find alveolar units that communicate directly with the conducting airway and are considered fast time constant units.
It is considered transitional gas (from airway to alveoli). An assumption is made here:50% of phase II gas belongs to the airway and 50% belongs to the alveoli. Further research is needed to determine if this holds true in all clinical conditions (such as dramatically increasing PEEP).

Phase III – Alveolar Gas
Phase III gas is entirely from the alveolar bed where gas exchange takes place.

Single Breath CO2 Waveform
EtCO2
Exhaled Tidal Volume
VD VALV
Z
Y
X


Clinical Application

Ventilation Management
Customize ventilator settings: VCO2 (CO2 elimination) reflects any changes in ventilation
and/or perfusion; it indicates instantly how patient gas exchange responds to ventilator
setting changes
Customize ventilator settings: VCO2 (CO2 elimination) reflects any changes in ventilation
and/or perfusion; it indicates instantly how patient gas exchange responds to ventilator
setting changes
VCO2
Vd/Vt
MValv
“Noninvasively monitored VCO2 provides an instantaneous indication of the change in alveolar ventilation in mechanically ventilated patients. It
allows instant, cheap and noninvasive determination of effective gas exchange.”
Dynamics of Carbon Dioxide Elimination Following Ventilator Resetting. Varsha Taskar, MD ; Joseph John, MD ; Anders Larsson, MD,PhD ; Torbjörn Wetterberg, MD, PhD ; Björn Jonson, MD, PhD – Chest 108/1/July 1995
.
.

Vd/Vt
• Ratio of Total Deadspace (Vd or Vdphys) to Tidal
Volume (Vt)• Total Deadspace = Airway + Alveolar Deadspace
• Normal = 0.25 to 0.30
• Estimates the Overall (In)efficiency of the
CardioRespiratory System
Why Measure Vd/Vt ? • Helps Understand what is Happening at the Alveolar Capillary Interface
• Measures Effectiveness of Ventilation
• Get Baseline Vd/Vt Defines Severity of Insult

Decrease in Perfusion
Baseline Perfusion
Decreased Perfusion

Monitoring trends allows for detection of sudden and rapid in VCO2, without change in Alveolar Minute Volume or Tidal Volumes. Drop in VCO2 suggests change in blood flow to the lungs. VCO2 may be due to in C.O. or blood loss. VCO2 may be due to in C.O. or malignant hyperthermia. Coupled with Alveolar Ventilation and Deadspace measurements, this allows for quick patient assessment.
Monitoring trend screens

Optimization of PEEP using VCO2/NICO
CASE STUDY:Profile: 60 Yr. Male, History of COPD and cardiac problems, Admitted to ED with severe respiratory distress, elevated temperature and semi-comatose. Patient intubated and placed on control ventilation and monitored with NICO. Tidal Volume (6ml/kg)= 600 ml, Respiratory Rate=10, I:E=1:2, PEEP= 8 FiO2 = 40%.
Baseline CO = 4 L/min, Over time SpO2 decreases from 94 to 88%. Flow/Volume loop and capnogram exhibit severe airway obstruction and increased work of breathing. Bronchodilator treatment administered and PEEP increased to 15 CmH2O. SpO2 = 95%. Observed a decrease in VCO2 (150 mL/m) and CO (2.5 L/m) due to increased intrathoracic pressure and decreased venous return. PEEP reduced to 8 cmH2O. Both cardiac output (3.4 L/m) and VCO2 (225 mL/m) returns to baseline levels.
Discussion: Use of NICO provided immediate and continuous feedback on the appropriateness of the ventilator strategy, and also allowed expeditious optimization of cardiac performance.
PEEP=0 PEEP lowered to 4
cmH2OPEEP
increased to 8 cmH2O

Alveolar Ventilation
MValv
• Alveolar Ventilation per Minute
• Amount of Vt that Reaches the Alveoli and is Available for Gas Exchange (Effective Ventilation)
Why Measure MValv ?
To provides the Most Effective CO2 Removal
To manage alveolar ventilation and not Vt

Successful Weaning Trial
Shows in spontaneous alveolar ventilation & corresponding decrease in ventilator support. VCO2 suggests metabolic activity due to additional task of breathing by the patient. Delivered mechanical tidal volume has not changed & spontaneous tidal volume is increasing (SIMV rate ). Shows PATIENT RESPONSE to the trial allowing for better management of the weaning process.

Unsuccessful Weaning Trial
SIMV and patient started to take over ventilation. But patient shows signs of fatigue at early stage ( VCO2 followed by in spontaneous tidal volume). Leads to in PaCO2 & EtCO2. Return to mechanical ventilation. Assists clinicians in determining PATIENT RESPONSE. When used effectively, these utilities may help reduce costly ventilator days.

Successful SBT
Here the patient’s ability to maintain Alveolar Ventilation sufficient for CO2 removal during a T-Piece Trial is proven.
Spontaneous Tidal Volumes have remained constant and have even shown slight increases over time.
Trends also show that the patient has been off mechanical support throughout the trial (no Vte MECH trend bars).

Unsuccessful SBT Initially, patient had a small amount of ventilatory support, but then was placed on a T-piece. The entire task of breathing was placed on the patient. Within minutes trends showed that the patient was unable to support the required level of ventilation (VCO2 decreasing since total Alveolar Ventilation is decreasing). Spontaneous Tidal Volume trend also shows inadequate ventilation. Removal of mechanical support, increased Vd/Vt, reducing ventilatory efficiency and the patient’s ability to remove CO2. This resulted in a pattern of rapid shallow breaths requiring the patient to be placed back on full mechanical support.


University of Tennessee Medical Center Data
• 600 Bed Hospital
• Designated Level 1 Trauma Center for Adults and Pediatrics
• Associated with University of Tennessee Graduate School of Medicine
• 50+ Bed Level 3 NICU
• 70+ Bed Adult Critical Care
• Operate Aggressive Therapist Driven Protocols on All Modalities of RC

Hospital Constraints
Step Down Units created (sub-acute care)
Step Down Units created (sub-acute care)
More severe ICU patient population
More severe ICU patient population
PreferNoninvasive technologies
PreferNoninvasive technologies
Pressure on hospital budgets
Human resources limited
Pressure on hospital budgets
Human resources limited
Need to keep ventilator-
time as minimal as
possible
Need to keep ventilator-
time as minimal as
possible
Need to be efficient and costsNeed to be efficient and costs

University of TN Medical Center
Implementation of Ventilation Management Protocol
3.3
12.5
2.0
11.0
0
5
10
15
VLOS HLOS
Pre-Protocol (585 pts)
Post-Protocol (643 pts)
Decrease of 39% Decrease of 12%

Re-intubation Rates
Extubation/Reintubation Rates
97939395
0
20
40
60
80
100
120
1st Qtr 2nd Qtr 3rd Qtr 4th Qtr
% N
ot
Re-
intu
bat
ed
Extubation/Reintubation Goal *Less than 6%

Quickly specific patient population became clear…
Patients in ALI/ARDS: requiring monitoring for optimization of PEEP and other ventilator settings
Patients with ventilator dysynchrony or other respiratory pattern issues that require differentiation of etiologies, prevention of exhaustive failures, etc.– Patients with failures to get to SBT, or appearances
of failures, such as RSBI, GCS, etc.– Differentiating Tachypnea vs Dyspnea– Early detection of exhaustion prior to
signs/symptoms

University of TN Medical Center
Difficult to Wean Patients(Five Months Retrospective)
30.7
1712
24.7
0
10
20
30
40
VLOS HLOS
Pre NICO (43 pts)
Post NICO (25 pts)
Decrease of 29% Decrease of 20%

Comparison Data

Reduction of Mechanical Ventilation Hours Using a Working Protocol with
the Cardiopulmonary Management System
Mikel W. O'Klock RRT, Dennis Harker RRT, Aksay Mahadevia MD, FCCP
Genesis Medical Center, Davenport, IA.
Reference: Respiratory Care, Dec 2005, Vol 50, Number 12, Page 95
Genesis Medical Center, Davenport, IA.

Background: Genesis Medical Center (GMC) is a 500 bed hospitalwith three adult Intensive Care units (ICUs) totaling45 lCU beds. Mechanical Ventilation Hours (MVH)for fiscal year 2003 totaled 84,000 with an average of123 hours per patient. We adopted a MechanicalVentilation Management Strategy Protocolincorporating the Respironics CardiopulmonaryManagement System (NICO) in an attempt to effectively reduce MVH.
Genesis Medical Center (cont).

Methods:
We retrospectively measured our MVH for
2003-2004. Next a protocol was
implemented using data from the NICO
monitor (SBCO2, VCO2, EtCO2, CO and
Vd/Vt) and a decision template. After 12
months of managing patients using the
protocol, MVH were again measured.
Genesis Medical Center (cont).

Results:By incorporating the ventilation management protocol, the decision process was simplified for both physician and therapist. This resulted in a significant reduction (p=0.001) in mechanical ventilation hours per patient.Ventilator Hours Statistical Analysis
Year Number of Patients
Total MVH MVH/pt
2003 612 72,492 118
2004 598 41,144 69
Genesis Medical Center (cont).

Conclusion:
By implementing a care protocol
incorporating the Respironics NICO we
observed a decrease of 43.2% in the total
number of ventilator hours, and a 42%
decrease in the number of hours per patient.
Genesis Medical Center (cont).

Implementation of Care Protocol Incorporating NICO
Total MVH
72,492
41,144
10,000
30,000
50,000
70,000
90,000
2003 (612 pts) 2004 (598 pts)
Decrease of 42.2%
Pre-NICO Post-NICO
Genesis Medical Center (cont).

Implementation of Care Protocol Incorporating NICO
(MVH per Patient)
118
69
0
50
100
150
2003 (612 pts) 2004 (598 pts)
Decrease of 42%
Pre-NICO Post-NICO
Genesis Medical Center (cont).

Continuous Monitoring Of Volumetric Capnography Reduces Length Of Mechanical Ventilation In A Heterogeneous Group Of Pediatric ICU Patients
Donna Hamel,RRT, RCP,FAARC Ira Cheifetz, MD, FAARC; Pediatric Critical Care Medicine.
Duke Children's Hospital, Durham, North Carolina
Reference: Respiratory Care, Dec 2005, Vol 50, Number 12, Page 107
Duke Children's Hospital, Durham, North Carolina

Background: Complications result from mechanical ventilation evenunder the best of circumstances; therefore, careful consideration must be provided for optimal management strategies on a continual basis. Recentadvances in technology provide clinicians access tononinvasive monitoring devices with the ability to display measurable and consistent data, thus, allowing for a more objective approach to totalventilator management.
Duke Children's Hospital (cont).

Volumetric capnography displays breath-by-breathmeasurements of exhaled carbon dioxide during the entire respiratory cycle. Additionally, theintegration of flow and carbon dioxide elimination over time enables the capnograph to calculate anddisplay alveolar minute ventilation (MVALV) anddeadspace ventilation (Vd/Vt). Therefore, volumetriccapnography should be a better marker for monitoring dynamic changes in gas exchange during mechanical ventilation than standard time-based capnometry alone.
Duke Children's Hospital (cont).

Hypothesis:
We hypothesized that the management of
patients using continuous volumetric capnography,
including monitoring of the deadspace to tidal
volume ratio, alveolar minute ventilation, and carbon
dioxide elimination (VCO2) would reduce the length
of ventilation (LOV) in infants and children.
Duke Children's Hospital (cont).

Methods: All mechanically ventilated PICU patients (0-18years of age) were eligible for enrollment in thisprospective, randomized study. Interventionpatients were placed on a NICO Respiratory Profile Monitor (Respironics, Inc.) on initiation of mechanicalventilation in our Pediatric lCU. These patients remained on the NICO Monitor until extubation. Control patients received all standard care and monitoring including intermittent use of volumetriccapnography at the discretion of the PICU team.
Duke Children's Hospital (cont).

Results:Both the parametric t-test and the non-parametric Wilcoxon test reflect a statistically significant difference in average length of ventilation with LOVbeing significantly reduced for the NICO group. Patients managed with continuous volumetric capnography (n=99) had a significantly shorter LOV than control patients (n=99) (117.3 vs. 171.4 hrs; P = 0.002). Extubation failure rates were similar for both groups.
Duke Children's Hospital (cont).

Conclusion:Length of ventilation in a heterogeneous group of pediatric patients was decreased by 2.25 days, a clinically significant 32%, with the use of Vd/Vt, MVALV and VCO2 monitoring. Such a significant decrease in LOV should corre late with a reductionin length of lCU admission cost, complications andmorbidity as well as improved patient and family satisfaction.
Duke Children's Hospital (cont).

Length of Ventilator Hours (99 patients)
171.4
117.3
0
50
100
150
200
Pre NICO Post NICO
Duke Children's Hospital (cont).

THANK YOU!

Contact Information
Michael Powers, MS, RRTDirector, Lung CenterUniversity of Tennessee Medical Center1940 Alcoa Highway, Suite E-110Knoxville, TN 37920Phone: 865-544-9274Fax: 865-544-6607E-mail: [email protected]



![Volumetric Capnography – The Next Advance in CO … Capnography.pdf · Volumetric Capnography – The Next Advance in CO 2 Monitoring ment [21-23]. For example, ... papers, included](https://img.pdfslide.us/doc/110x75/5aab36407f8b9a693f8b9ad6/volumetric-capnography-the-next-advance-in-co-capnographypdfvolumetric.jpg)