Embed Size (px)
DESCRIPTION
Citation preview
PTQ Injections for Faecal Incontinence
Michelle Tan Su Wei
Faecal IncontinenceFaecal Incontinence
DefinitionDefinition Continuous or recurrent Continuous or recurrent
uncontrolled passage of faecal uncontrolled passage of faecal material (>10mL) for at least one material (>10mL) for at least one month in an individual older than 3 month in an individual older than 3 years of ageyears of age
Faecal IncontinenceFaecal Incontinence
Minor incontinenceMinor incontinenceInadvertent escape of flatus or partial Inadvertent escape of flatus or partial
soilingsoiling
of undergarmentsof undergarments
Major incontinenceMajor incontinenceInvoluntary excretion of faecesInvoluntary excretion of faeces
Causes of Faecal IncontinenceCauses of Faecal Incontinence
OverflowOverflowReduced storage capacityReduced storage capacityWeakness of internal anal sphincterWeakness of internal anal sphincterWeakness of external anal sphincter onlyWeakness of external anal sphincter onlyWeakness of puborectalis muscleWeakness of puborectalis muscleDecreased perception of rectal sensationDecreased perception of rectal sensation

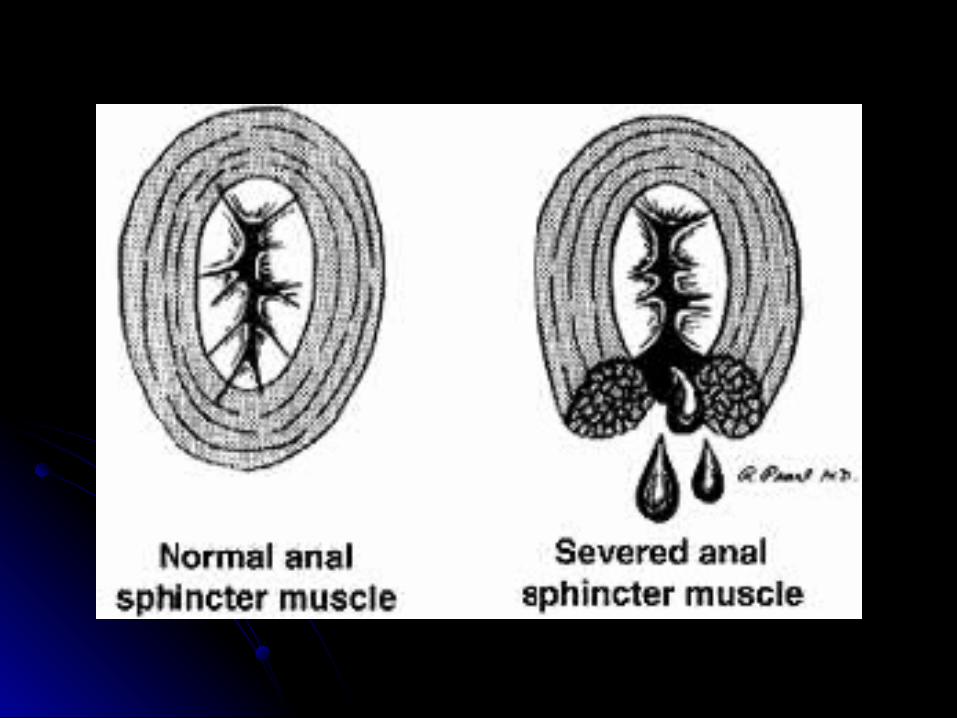
Internal anal sphincterInternal anal sphincter
Provides most of the resting anal tone Provides most of the resting anal tone Main muscle to prevent faecal leakageMain muscle to prevent faecal leakageCauses of IAS damageCauses of IAS damage
- primary idiopathic degeneration- primary idiopathic degeneration- at childbirth - at childbirth - during anal surgery- during anal surgery- secondary to other tissue disorders such - secondary to other tissue disorders such as sclerodermaas scleroderma
Treatment options for damaged IASTreatment options for damaged IAS Direct surgical repair of IAS (normal IAS: 2.4-Direct surgical repair of IAS (normal IAS: 2.4-
3.4 mm thick) and held at constant basal 3.4 mm thick) and held at constant basal tension (not beneficial in long term)tension (not beneficial in long term)
Dynamic graciloplasty/implantation of artificial Dynamic graciloplasty/implantation of artificial bowel sphincter (good results but high bowel sphincter (good results but high complication and failure rate)complication and failure rate)
Sacral nerve stimulationSacral nerve stimulation- electrical stimulation of sacral nerve roots - electrical stimulation of sacral nerve roots can restore continence in patients with can restore continence in patients with structurally intact musclesstructurally intact muscles- less invasive but experience still limited- less invasive but experience still limited
Silicone injection (PTQ ™ implant)Silicone injection (PTQ ™ implant)
PTQ ™PTQ ™ PTQPTQ1,10-phenanthroline-5,6-dione1,10-phenanthroline-5,6-dione Silicone implant comprises medical-grade vulcanized Silicone implant comprises medical-grade vulcanized
silicone particles which are ductile and of irregular silicone particles which are ductile and of irregular texturetexture
These are suspended in hydrogel low molecular weight, These are suspended in hydrogel low molecular weight, water soluble polyvinylpyrrolidone (povidone, PVP) water soluble polyvinylpyrrolidone (povidone, PVP) carrier vehicle which is eliminated by the carrier vehicle which is eliminated by the reticuloendothelial system and excreted through the reticuloendothelial system and excreted through the kidney unchangedkidney unchanged
Mechanism of action of PTQ ™ still unclearMechanism of action of PTQ ™ still unclear It is presumed to exert a “padding effect” in the It is presumed to exert a “padding effect” in the
submucosal plane to promote anal closuresubmucosal plane to promote anal closure May be the next choice of treatment as numerous May be the next choice of treatment as numerous
studies have demonstrated studies have demonstrated
Contraindications of PTQ ™Contraindications of PTQ ™ Rectal prolapseRectal prolapse Faecal impactionFaecal impaction Symptomatic Symptomatic
haemorrhoidshaemorrhoids Perianal and anal Perianal and anal
scarringscarring Perianal sepsisPerianal sepsis Parasitic infection Parasitic infection
(threadworms)(threadworms) Congenital anal sphincter Congenital anal sphincter
defectdefect
Uncontrolled diabetesUncontrolled diabetes ImmunosuppressionImmunosuppression Acute inflammation, Acute inflammation,
infection or malignancyinfection or malignancy Pregnancy or within one Pregnancy or within one
year postpartumyear postpartum Within 12 weeks of Within 12 weeks of
another PTQ implant another PTQ implant treatmenttreatment
Standard PTQ treatment includes three 2.5 ml PTQ implants and one implantation needle to provide product for trans-dermal augmentation at multiple sites within the internal anal sphincter
Before the procedureBefore the procedure
Antiplatelet therapy ceased for minimum of Antiplatelet therapy ceased for minimum of 7 days before injection7 days before injection
Patient administered with Fleet enema 2 Patient administered with Fleet enema 2 hours before procedurehours before procedure
All patients receive IV prophylactic All patients receive IV prophylactic antibiotics (Gentamicin 160 mg and antibiotics (Gentamicin 160 mg and Metronidazole 500 mg)Metronidazole 500 mg)
During the procedureDuring the procedure Injection performed under local anaesthesia as an Injection performed under local anaesthesia as an
outpatient procedureoutpatient procedure Patient is placed in the prone jack-knife position and Patient is placed in the prone jack-knife position and
the area cleaned, including anal canal irrigation with the area cleaned, including anal canal irrigation with betadine solutionbetadine solution
18 gauge 2.5 inch needle introduced through the 18 gauge 2.5 inch needle introduced through the skin approximately 2 cm from anal marginskin approximately 2 cm from anal margin
Needle is advanced above the dentate line guided Needle is advanced above the dentate line guided by a finger anal canalby a finger anal canal
Care taken not to penetrate mucosaCare taken not to penetrate mucosa 3 injections into submucosal plane of 2.5mL at 3, 7 3 injections into submucosal plane of 2.5mL at 3, 7
and 11 o’clock positions without endosonographic and 11 o’clock positions without endosonographic surveillancesurveillance
Duration of procedure takes around half an hourDuration of procedure takes around half an hour
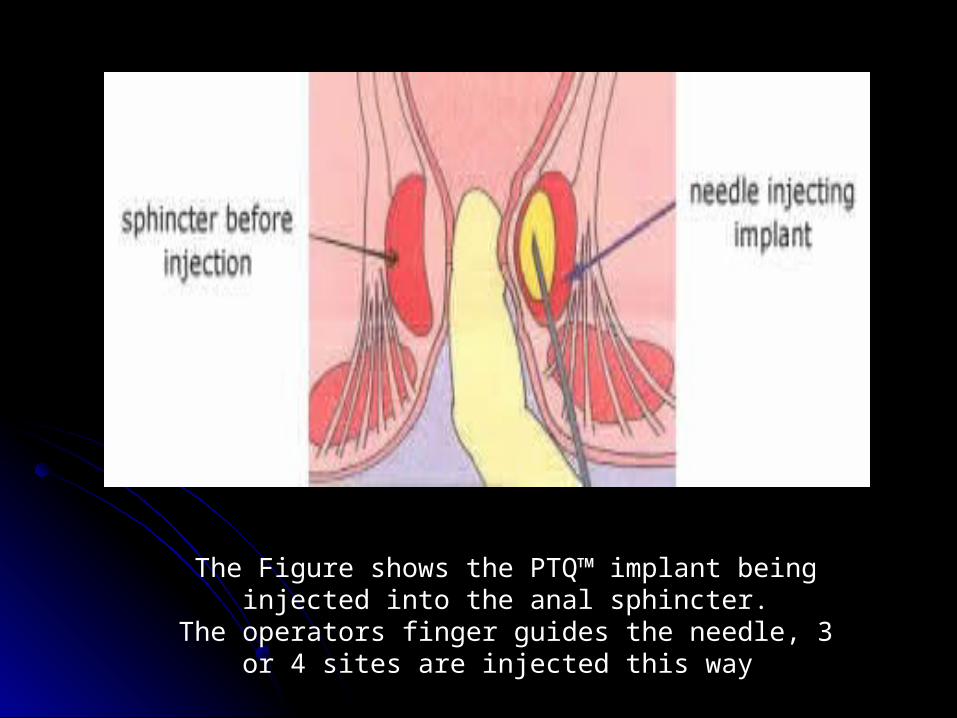
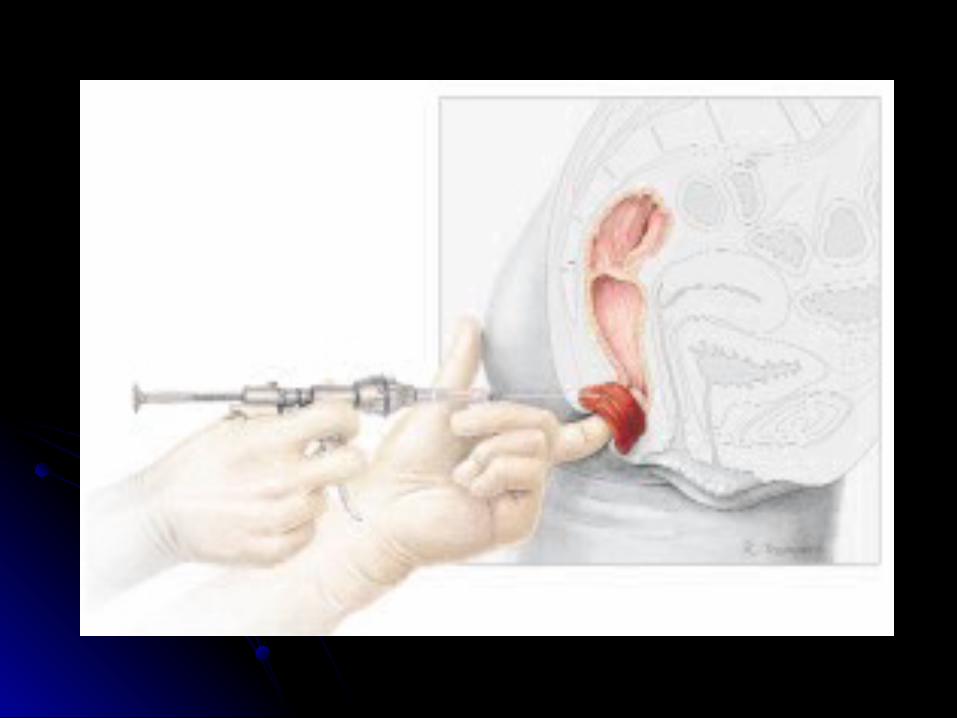
The Figure shows the PTQ™ implant being injected into the anal sphincter.
The operators finger guides the needle, 3 or 4 sites are injected this way
After the procedureAfter the procedure
Patients observed over 6 hour period to Patients observed over 6 hour period to exclude any complication of pain or exclude any complication of pain or bleedingbleeding
Discharged with oral antibiotics Discharged with oral antibiotics (Cephalexin 500 mg QDS and (Cephalexin 500 mg QDS and Metronidazole 400 mg TDS), laxatives Metronidazole 400 mg TDS), laxatives (oral lactulose 15 mL) and oral analgesia (oral lactulose 15 mL) and oral analgesia (Paracetamol 500 mg) for 1 week(Paracetamol 500 mg) for 1 week
Follow-upFollow-up Patients who showed improvement:Patients who showed improvement:
Endoanal ultrasound scans showed PTQ ™ implants within Endoanal ultrasound scans showed PTQ ™ implants within the upper part of anal canal extending up to, and partly the upper part of anal canal extending up to, and partly beyond, the level of the puborectalis ringbeyond, the level of the puborectalis ring
Patients who did not show improvement:Patients who did not show improvement:Endoanal ultrasound showed residual PTQ ™ had Endoanal ultrasound showed residual PTQ ™ had migrated to lie above the puborectalis muscle so that migrated to lie above the puborectalis muscle so that there was no material remaining within the anal canalthere was no material remaining within the anal canal
There were no episodes of leakage or There were no episodes of leakage or infectioninfection
Some patients complained of pruritus ani Some patients complained of pruritus ani during the first weeks after the during the first weeks after the procedureprocedure
Constipation not encounteredConstipation not encountered
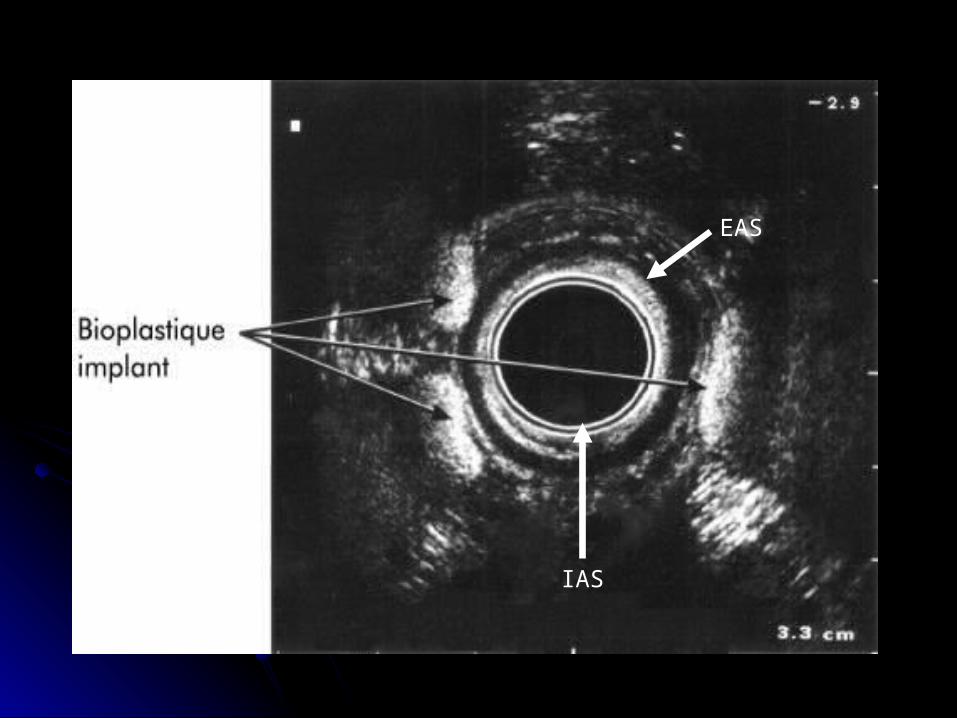
EAS
IAS
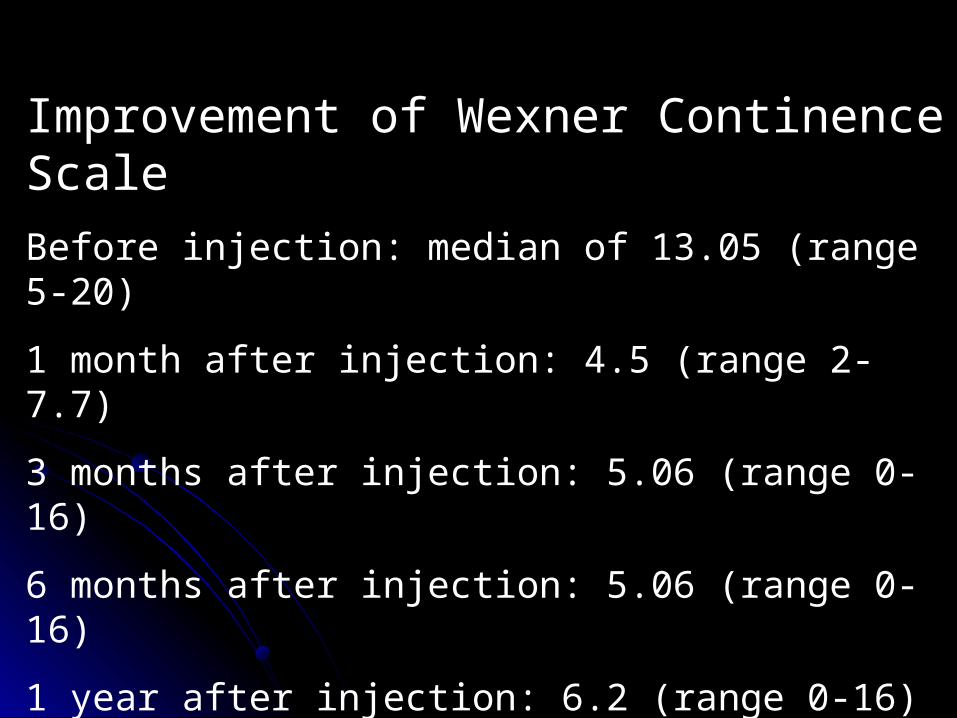
Improvement of Wexner Continence Scale
Before injection: median of 13.05 (range 5-20)
1 month after injection: 4.5 (range 2-7.7)
3 months after injection: 5.06 (range 0-16)
6 months after injection: 5.06 (range 0-16)
1 year after injection: 6.2 (range 0-16)
2 years after injection: 9.4 (range 1-20)
Portilla et al
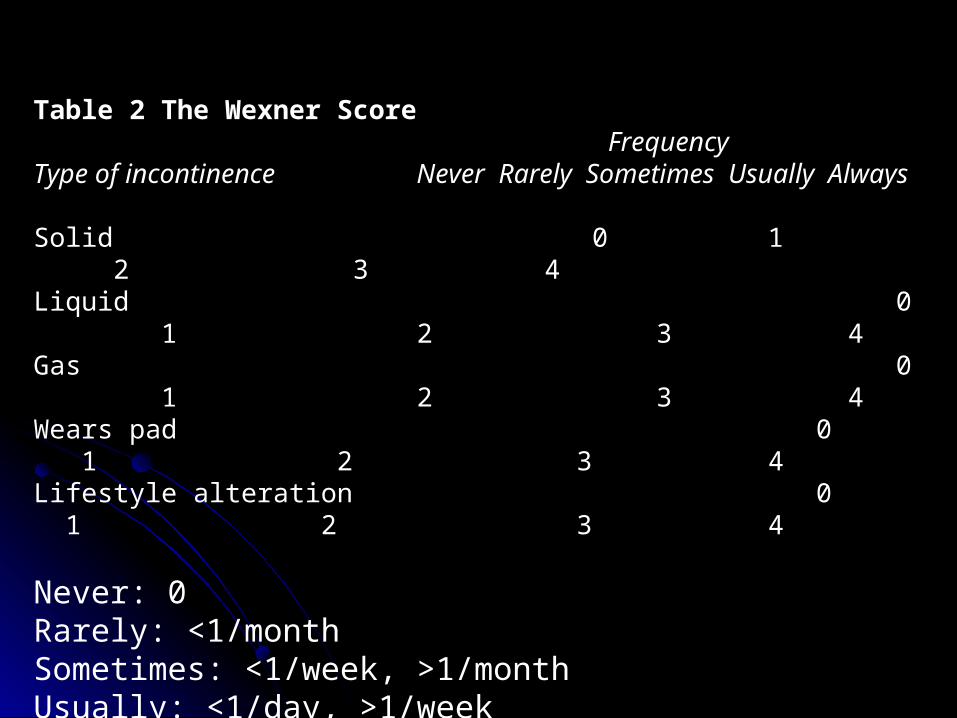
Table 2 The Wexner ScoreFrequency
Type of incontinence Never Rarely Sometimes Usually Always
Solid 0 1 2 3 4Liquid 0 1 2 3 4Gas 0 1 2 3 4Wears pad 0 1 2 3 4Lifestyle alteration 0 1 2 3 4
Never: 0Rarely: <1/monthSometimes: <1/week, >1/monthUsually: <1/day, >1/weekAlways: >1/day0Perfect20Complete incontinence
Changes in anal manometry after PTQ ™ Changes in anal manometry after PTQ ™ injectioninjection
Kenefick, Vaizey, Malouf et alKenefick, Vaizey, Malouf et alo Resting anal pressure: increase to a median of 63%Resting anal pressure: increase to a median of 63%o Vascular filling of anal cushions normally contribute Vascular filling of anal cushions normally contribute
15-20% of resting anal pressure15-20% of resting anal pressureprovides a provides a watertight seal at the anal marginwatertight seal at the anal margin
o Bulking effect of silicone injections may be Bulking effect of silicone injections may be enhancing the action of the naturally occurring anal enhancing the action of the naturally occurring anal cushions which provide closure in the gap inside the cushions which provide closure in the gap inside the IAS ringIAS ring
Effect of PTQ ™ on EASEffect of PTQ ™ on EAS
Squeeze pressure rose to a median of Squeeze pressure rose to a median of 45% (not significant) 45% (not significant)
However, it represented an improvement However, it represented an improvement in EAS functionin EAS function
Increase in pressure was probably due to Increase in pressure was probably due to physical bulking effect of the 3 injectionsphysical bulking effect of the 3 injections
Why PTQ ™ not associated with Why PTQ ™ not associated with absorptive or migration problemsabsorptive or migration problems
Continuous clinical trials and physiological benefit Continuous clinical trials and physiological benefit combined with persistent findings in endoanal US combined with persistent findings in endoanal US suggest the use of PTQ ™ as a bulking agent will not be suggest the use of PTQ ™ as a bulking agent will not be associated with problems of migration or absorption associated with problems of migration or absorption experienced with previous bulking techniquesexperienced with previous bulking techniques
Animal studiesAnimal studies: PVP is excreted over a period of 3 days, : PVP is excreted over a period of 3 days, leaving non-absorbable non-biodegradable silicone leaving non-absorbable non-biodegradable silicone particles. The gel is slowly replaced by a fibrin and particles. The gel is slowly replaced by a fibrin and protocollagen matrix that surrounds silicone particles protocollagen matrix that surrounds silicone particles which at 6 weeks becomes stabilised with collagen which at 6 weeks becomes stabilised with collagen fibres. This forms permanent bulking agent that fibres. This forms permanent bulking agent that augments IASaugments IAS
PTQ ™ in patients post PTQ ™ in patients post haemorrhoidectomyhaemorrhoidectomy
Chan and TjandraChan and Tjandra Carried out PTQ ™ injection for patients with passive faecal Carried out PTQ ™ injection for patients with passive faecal
incontinence post haemorrhoidectomyincontinence post haemorrhoidectomy Procedure similar except it was carried out under endoanal Procedure similar except it was carried out under endoanal
ultrasound guidance with 25 gauge hypodermic needles ultrasound guidance with 25 gauge hypodermic needles inserted into the intersphincteric space and IAS defects in inserted into the intersphincteric space and IAS defects in the upper anal canal just below puborectalis ringthe upper anal canal just below puborectalis ring
Then, an 18 gauge, 2.5 inch needle with a ratchet gun was Then, an 18 gauge, 2.5 inch needle with a ratchet gun was inserted through the perianal skin at a position inserted through the perianal skin at a position predetermined by the in situ hypodermic needle.predetermined by the in situ hypodermic needle.
With a digit within the anal canal, injection of PTQ ™ is With a digit within the anal canal, injection of PTQ ™ is performedperformed
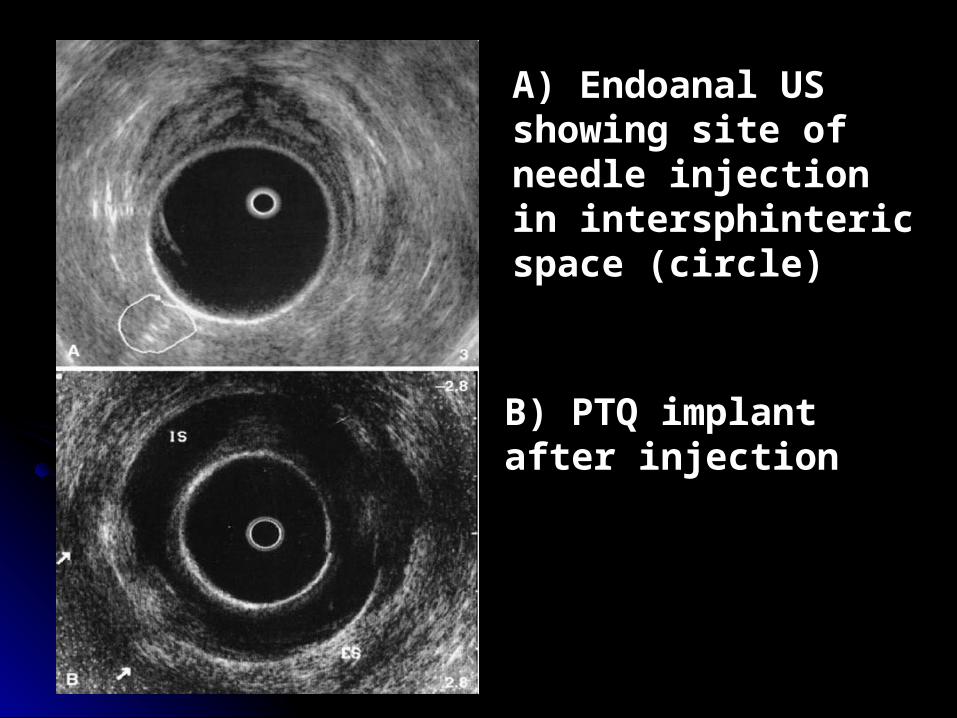
A) Endoanal US showing site of needle injection in intersphinteric space (circle)
B) PTQ implant after injection
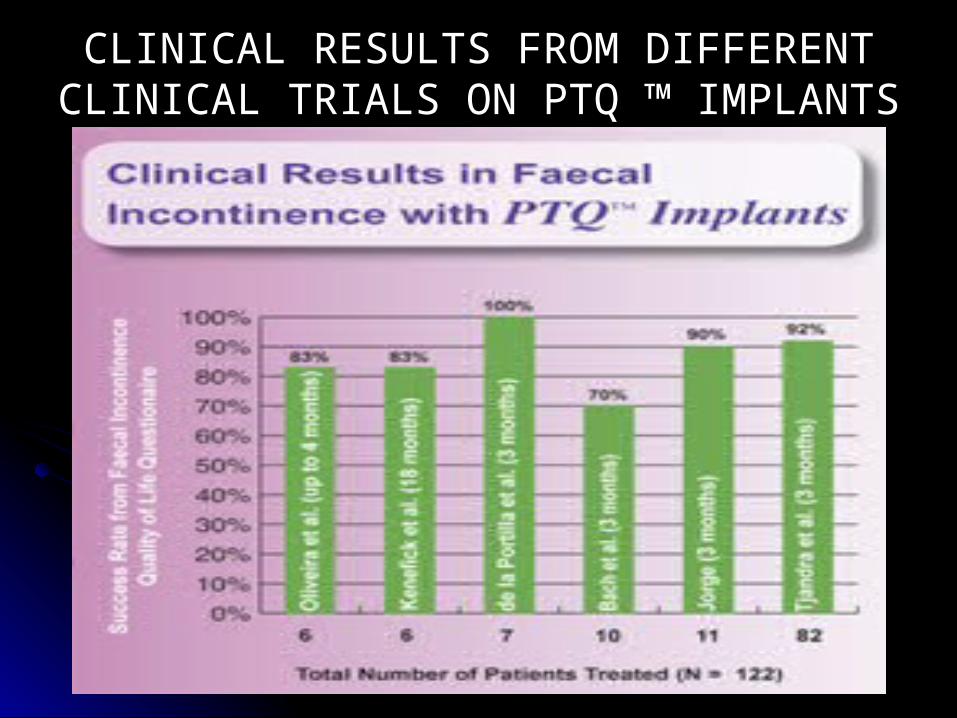
CLINICAL RESULTS FROM DIFFERENT CLINICAL TRIALS ON PTQ ™ IMPLANTS
Future research studies on PTQ ™Future research studies on PTQ ™
Results of perianal PTQ ™ injections for passive Results of perianal PTQ ™ injections for passive faecal incontinence are variable in the long termfaecal incontinence are variable in the long term
Further studies with longer follow-up and larger Further studies with longer follow-up and larger numbers are required numbers are required
Maeda, Vaizey, Kamm et al (2007)Maeda, Vaizey, Kamm et al (2007)Conducted their study on 6 patients and follow up of 61 Conducted their study on 6 patients and follow up of 61 monthsmonths small change in incontinence score from 13 to small change in incontinence score from 13 to 11 in 5 out of the 6 patients11 in 5 out of the 6 patients
Precise technique for implantation and the best Precise technique for implantation and the best location of the implant need to be determined; location of the implant need to be determined; whether ultrasound guided or not OR whether ultrasound guided or not OR submucosal vs interspincteric injectionsubmucosal vs interspincteric injection
1. NJ Kenefick, CJ Vaizey, AJ Malouf, CS Norton, M Marshall and MA Kamm. Injectable silicone biomaterial for faecal incontinence due to internal anal sphincter dysfunction. Gut 2002; 51: 225-228
2. F. de la Portilla, A. Fernandez, E. Leon, R. Rada, N. Cisneros, VH Maldonado, J. Vega, E. Espinosa (2008) Evaluation of the use of PTQ ™ implants for the treatment of incontinent patients due to internal anal sphincter dysfunction. Colorectal Disease 10 (1), 89-04
3. UpToDate. Kristen Robson, Anthony J Lembo, Nicholas J Talley, Peter AL Bonis. Updated Feb 6, 2008
4. Chan, M.K., & Tjandra, J.J. (2006). Injectable silicone biomaterial (PTQ) to treat fecal incontinence after hemorrhoidectomy. Dis Colon Rectum, 49(4), 433-439.
5. Maeda, Y., Vaizey, C.J., & Kamm, M.A. (2007). Long-term results of perianal silicone injection for faecal incontinence. Colorectal Dis, 9(4), 357-361.
6. Uroplasty.com
References