Embed Size (px)
Citation preview
ROLE OF ANODYNE THERAPY
MONOCHROMATIC INFRARED PHOTOENERGY IN DIABETIC PERIPHERAL NEUROPATHY
DR GHANSHYAM GOYAL, DR A K JAIN, DR REKHA SRIVASTAVA
S.K.DIABETES RESEARCH AND EDUCATION CENTRE118, R.R.Sarani, Kolkata -9
Distal polyneuropathy is the most common complication affecting the lower extremities of patients with dm
Upto 60% of patients with long standing dm, had dpn
Neuropathy, a major etiological component of diabetic foot ulcer
Is present in more than 82% of diabetics with foot wounds
Is a leading cause of amputations and high mortality rates among diabetics.
SYMPTOMS Burning
Tingling
Stabbing & pins & needles sensation in a stocking & gloves distribution
Patient may often display muscle weakness, incoordination and ataxia
The association between neuropathic pain and
decreased quality of life in patients with DPN is well
documented.
PATHOGENISIS OF DPN Poorly understood
Multifactorial
Hyperglycemia - being the prime risk factor
Ischaemic
THEORIES Abnormalities of protien glycation Sorbitol accumalation Polyol pathway flux Protein kinase activation Advanced glycation end product Decrease in neuronal nitric oxide
synthaetase protein Microvascular hypoxia
One of the causative factors is
decreased endoneural blood flow
MANAGEMENT OF DN Disease modification Symptomatic treatment DISEASE MODIFICATION Glycaemic control Association of vascular risk factors with DN Aldolase reductase inhibitors(ARIS) Alpha Lipoic acid Carnitine Neurotrophic therapy
SYMPTOMATIC TREATMENT Tricyclic Antidepressants Anticonvulsants ( Phenytoin,
Carbomazepine & Gabapentin) Tramadol Analgesics are not of much benefit
and narcotic should be avoided because of addiction potential.
TNS ANODYNE THERAPY
MIRE TECHNOLOGY
The anodyne therapy system delivers mire through therapy arrays, each containing 60 super-luminous
diodes ( 890 nanometers, near infrared wavelength). These diodes are attached to a control unit that
pulses the mire at 292 times/sec. The therapy arrays are placed in direct contact with the skin to temporarily increase local micro-circulation.

ANODYNE THERAPY
BASELINE CHARACTERISTIC OF PATIENTS
No of patients in study = 47
Mean age = 57.91 ( 38-81 yrs)
Mean duration of diabetes = 12.7 yrs
Mean biothesiometer Right - 35.6 v Left - 35.8 v
Male : female 33: 14
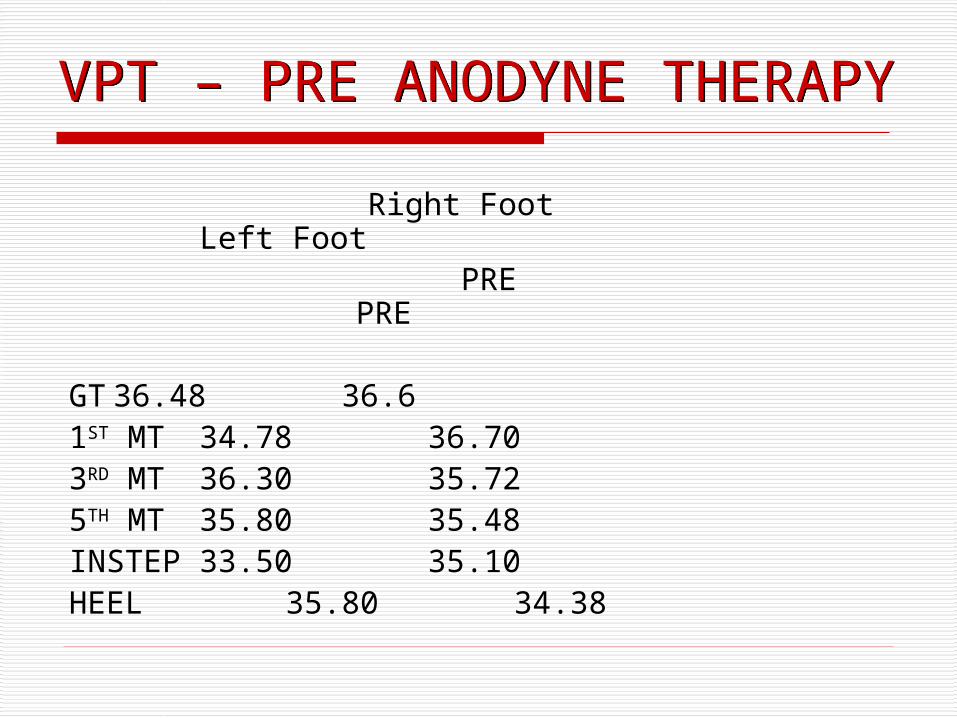
VPT – PRE ANODYNE THERAPY Right Foot Left Foot PRE PRE GT36.48 36.6 1ST MT 34.78 36.70 3RD MT 36.30 35.72 5TH MT 35.80 35.48 INSTEP 33.50 35.10 HEEL 35.80 34.38
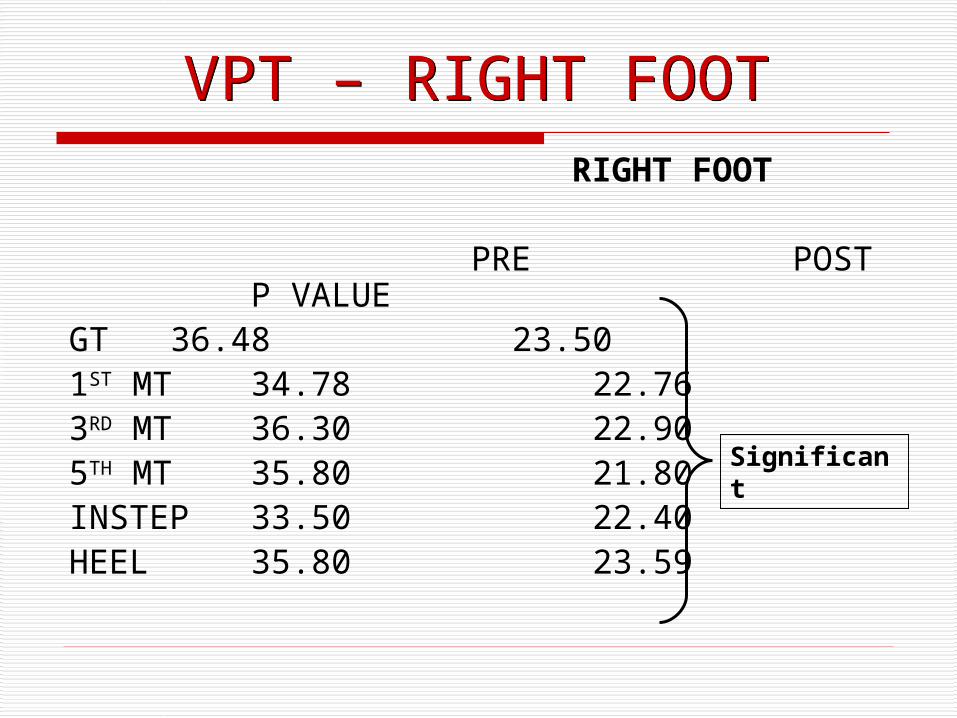
VPT – RIGHT FOOT RIGHT FOOT
PRE POST P VALUEGT 36.48 23.50 1ST MT 34.78 22.763RD MT 36.30 22.905TH MT 35.80 21.80 INSTEP 33.50 22.40HEEL 35.80 23.59
Significant
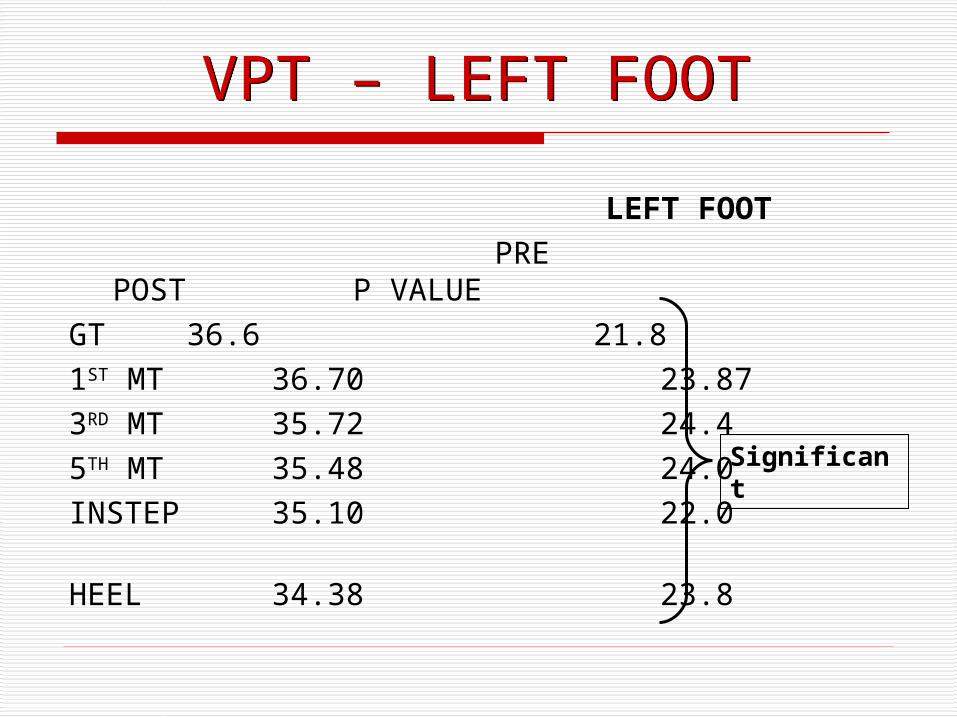
VPT – LEFT FOOT LEFT FOOT PRE POST P
VALUEGT 36.6 21.8 1ST MT 36.70 23.87 3RD MT 35.72 24.4 5TH MT 35.48 24.0 INSTEP 35.10 22.0 HEEL 34.38 23.8
Significant
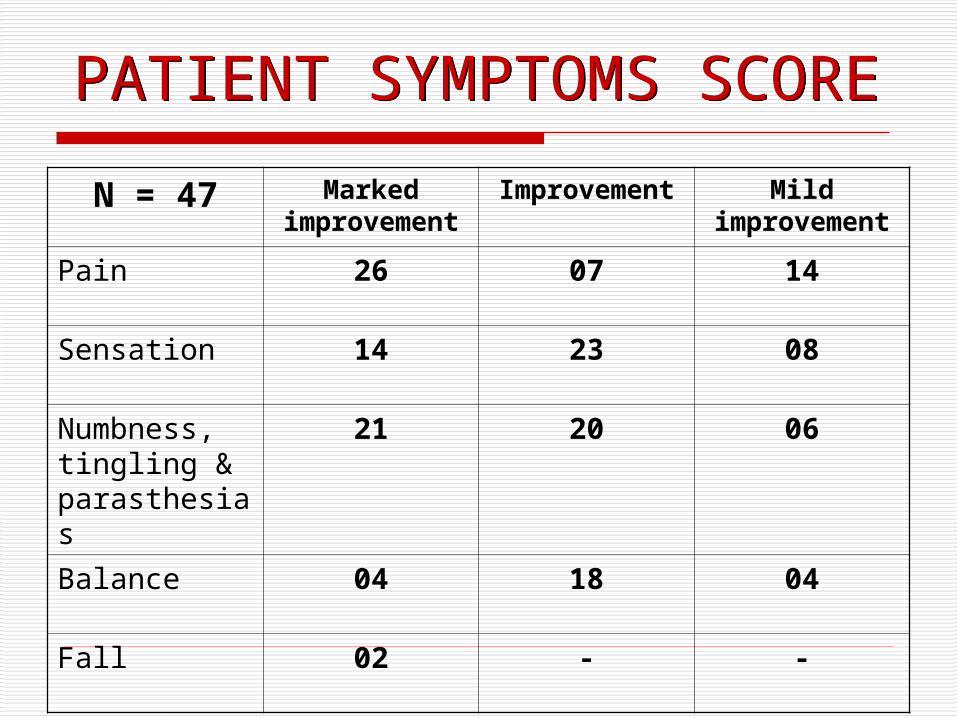
PATIENT SYMPTOMS SCORE
N = 47 Marked improvemen
t
Improvement
Mild improvemen
tPain 26 07 14
Sensation 14 23 08
Numbness, tingling & parasthesias
21 20 06
Balance 04 18 04
Fall 02 - -
CONCLUSION Our knowledge regarding the
pathogenisis of DN has grown significantly in last two decades
But identifying effective treatment regime remains a challenge
Prevention remains the foundation of clinical intervention and the pre requisites of adequate treatment
Mire treatments are associated with increased foot sensation in patients with dpn
IMPROVED FOOT SENSITIVITY BASED ON THE USE OF MIRE MIGHT BE ASSOCIATED WITH A REDUCED INCIDENCE OF DIABETIC FOOT WOUNDS AND AMPUTATIONS
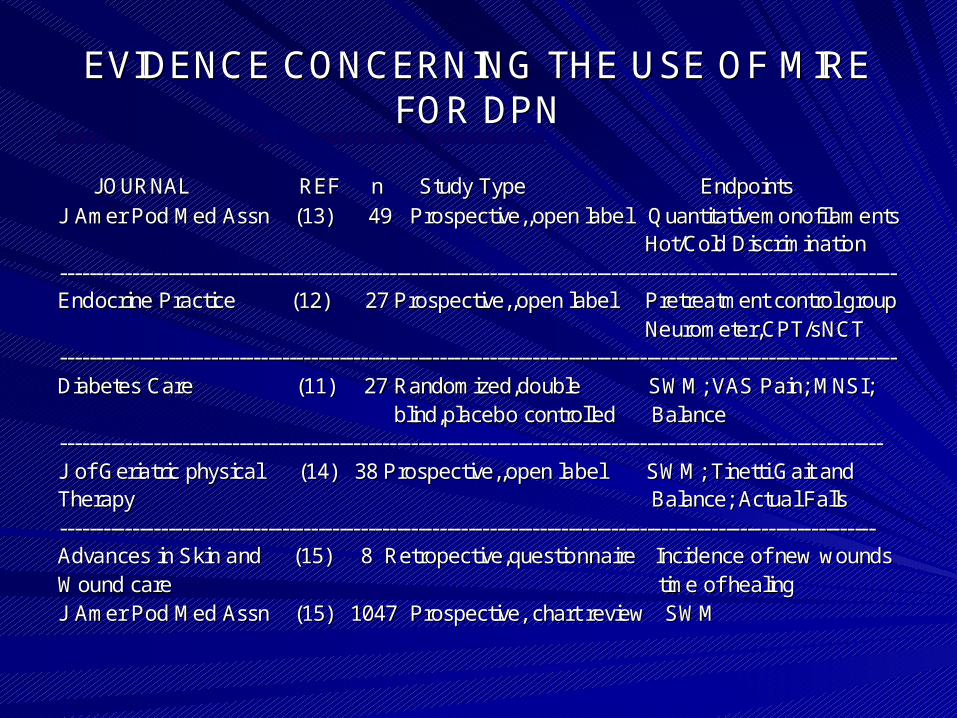
EVIDENCE CONCERNING THE USE OF MIRE EVIDENCE CONCERNING THE USE OF MIRE FOR DPNFOR DPN
JOURNAL REF n Study Type JOURNAL REF n Study Type EndpointsEndpointsJ J AmerAmer Pod Med Assn (13) 49 Pod Med Assn (13) 49 Prospective,,openProspective,,open label label QuantitativemonofilamentsQuantitativemonofilaments
Hot/Cold DiscriminationHot/Cold Discrimination-------------------------------------------------------------------------------------------------------------------------------- ----------------------------------------------------------------------------------------------------------Endocrine Practice (12) 27 Endocrine Practice (12) 27 Prospective,,openProspective,,open label Pretreatment control grouplabel Pretreatment control group
Neurometer,CPT/sNCTNeurometer,CPT/sNCT-------------------------------------------------------------------------------------------------------------------------------- ----------------------------------------------------------------------------------------------------------Diabetes Care (11) 27 Diabetes Care (11) 27 Randomized,doubleRandomized,double SWM; VAS Pain; MNSI;SWM; VAS Pain; MNSI;
blind,placeboblind,placebo controlledcontrolled BalanceBalance-------------------------------------------------------------------------------------------------------------------------------- ------------------------------------------------------------------------------------------------------J of Geriatric physical (14) 38 J of Geriatric physical (14) 38 Prospective,,openProspective,,open label SWM; label SWM; TinettiTinetti Gait and Gait and TherapyTherapy Balance; Actual FallsBalance; Actual Falls-------------------------------------------------------------------------------------------------------------------------------- ----------------------------------------------------------------------------------------------------Advances in Skin and (15) 8 Advances in Skin and (15) 8 Retropective,questionnaireRetropective,questionnaire Incidence of new woundsIncidence of new woundsWound care Wound care time of healingtime of healingJ J AmerAmer Pod Med Assn (15) 1047 Prospective, chart review SWMPod Med Assn (15) 1047 Prospective, chart review SWM
![[XLS]eci.nic.ineci.nic.in/delim/paper1to7/TamilNadu.xls · Web viewRev. Dharmapuri & Kanniyakumari Paper 7 Paper 6 Paper 5 Paper 4 Paper 3 Paper 2 Paper 1 Index Tirunelveli (M.Corp.)](https://img.pdfslide.us/doc/110x75/5ad236e17f8b9a86158ce167/xlsecinicinecinicindelimpaper1to7-viewrev-dharmapuri-kanniyakumari-paper.jpg)