Embed Size (px)
Citation preview

TRENDS IN DENTAL CARIES OVER THE LAST 5 YEARS
CHAITANYA.P
III MDS
Dept of Public Health Dentistry
Contents:-
• Prevalence of dental caries.
• FDI world dental federation report on dental caries.
• Spatial distribution of dental caries in the world.
• Global burden of dental caries among the countries.
• Distribution of dental caries among the world countries.
• Risk of dental caries among WHO regional countries.
2

• Studies related to prevalence of dental caries in various countries.
• Annual dental caries cases in Asian countries.
• Dental caries burden throughout India.
• Retrospective analysis of dental caries studies till 2015.
• References.
3

Definitions
Dental caries is an irreversible microbial disease of the
calcified tissues of the teeth, characterized by
demineralization of the inorganic portion and destruction of
the organic substance of the tooth, which often leads to
cavitations.
4Shafer’s text book of Oral pathology, 2012, pg.no.455-498, 7th edition.
Dental caries is an infectious
microbiologic disease of the teeth that results
in localized dissolution and destruction of the
calcified tissues.
5
Sturdevant’s Art and Science of Operative Dentistry. 2012 Pg.no.428, 6th edition

• Ostronn (1980)
Dental caries is a process of enamel or dentin dissolution
that is caused by microbial action at the tooth surface and is
mediated by physicochemical flow of water dissolved ions.
Hume (1993)
Caries is essentially a progressive loss by acid
dissolution of the apatite (mineral) component of the enamel
than the dentin or of cementum.
(Shobha Tandon)
6Shobha Tandon. Text book of Pedodontics. 2008, pg.no. 312, 2nd edition
• Muthusivakumar
Dental caries is a microbial disease of the
calcified tissues of the teeth characterized by
demineralization of the inorganic portion and
destruction of the organic substance of the tooth.
(Damle)
7Muthu Sivakumar. Pediatric dentistry : Principles and Practice. 2011, Pg.no.120; 2nd edition
• Ole Fejerskov and Edwina kidd
Black defined caries the following way in the German
translation of the text from 1914.
Caries in its simplest expression consists in a chemical
dissolution of the calcium salts of the tooth by lactic acid,
followed by the decomposition of the organic matrix, or
gelatinuous body, which in the dentin is left after the solution of
the calcium salts. In caries of the enamel, the whole substance
of the tissue is removed by dissolving out the calcium salts.
8

• Dental caries currently represents the most common chronic disease among children; it is
five times more common than
asthma, and seven times more
common than seasonal allergies
-(U.S. Department of Health and Human Services, 2014).
9

FDI World Dental Federation
ORAL CONDITIONS ARE THE MOST COMMON CONDITIONS OF HUMANKIND As part of the recent international collaborative Global Burden of Disease Study (1990-
2010), untreated tooth decay was identified as the most common condition among 291 diseases studied
WORLDWIDE, BETWEEN 60 - 90% OF SCHOOL CHILDREN HAVE DENTAL CARIES
10

30% OF PEOPLE WORLDWIDE AGED 65–74 YEARS HAVE LOST ALL THEIR NATURAL TEETH
THE BURDEN OF ORAL DISEASES IS HIGHER AMONG POOR AND DISADVANTAGED POPULATION GROUPS
11

The greatest burden of caries occurs in adult life and the greatestcost of treating caries is in adults. This issue does not receivesufficient attention from dentists and most policies, programmesand surveys of dental caries have focused on children.
(Sheiham & James 2014)
For most countries, irrespective of the DMFT levels in 12-year-olds, the percentagedifference in levels of DMFT between 12-year-olds and 35-44-year-olds was above500% and the relative difference was 5 or more. Caries levels were also very muchhigher in adults than in children in all countries with high percentages of theirpopulation drinking fluoridated water.
(Bernabe 2014) 12
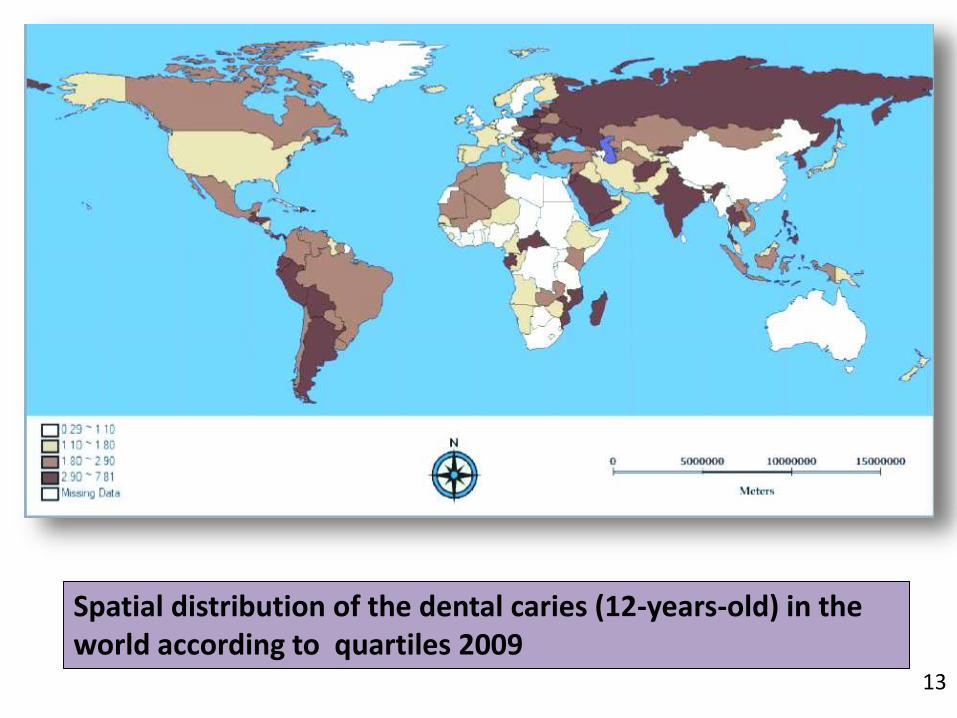
Spatial distribution of the dental caries (12-years-old) in the world according to quartiles 2009
13

A disease that is caused specifically by free sugars and affecting 3.9 billionpeople worldwide means that untreated caries is the most prevalent of all291 conditions assessed in the recent Global Burden of Disease study
(Marcenes et al 2013).
Early 21st century, a significant bulk of evidence allows us toassume that social, economic, cultural, environmental andhealth-system-related determinants are part of a web ofpossible causes of dental caries.
14

Dental caries is the fourthmost expensive disease totreat.
For children of most low-income countries, treatingdental caries is estimated atUS $3513 per 1000children, which wouldexceed the country’s totalhealth budget.
15

• It affects about 60-90% of school children, and almost 100% of adults through out the world.
source:-World Health Organization. Oral health. Available from:http://www.who.int/mediacentre/factsheets/fs318/en/. [Last accessed on 2017 Jan 30].
-
60-90% 100%
16

WHY IS IT INCREASING IN DEVELOPING COUNTRIES
Diets rich in sugars
Neglected oral hygiene
Less or no use of fluorides
Limited health services
No preventive measures
Lack of awareness
Reason for urbanized population having more caries in developing
countries:
* Consumption of refined sugar comparatively more than the rural
population.
17

18
Oral health a report by FDI World Federation 2016. pg.no.14 &15

19
20
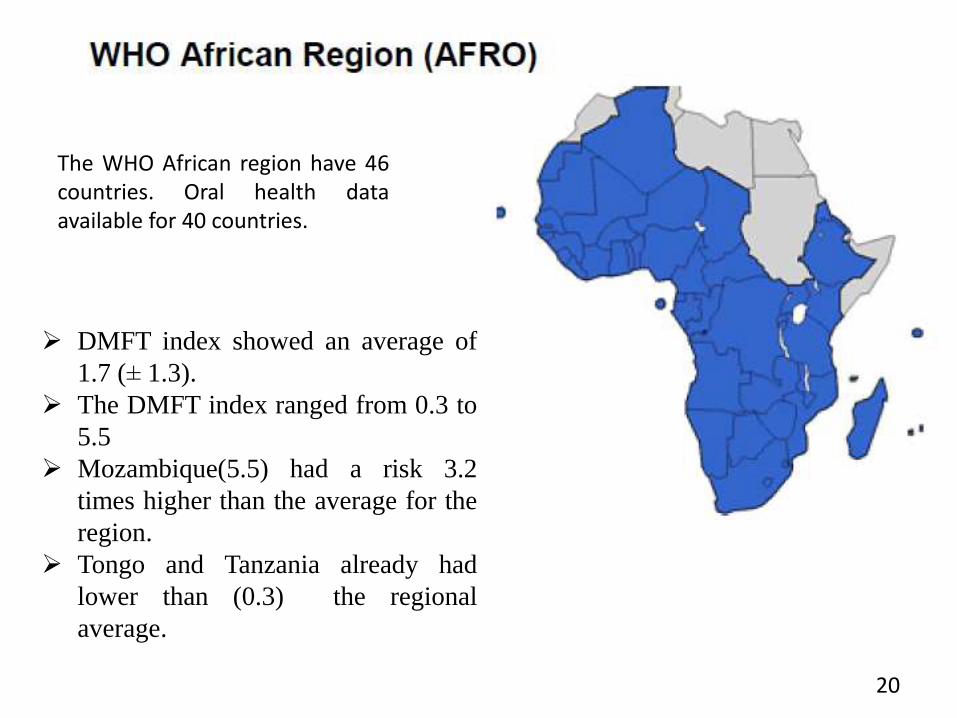
The WHO African region have 46countries. Oral health dataavailable for 40 countries.
DMFT index showed an average of
1.7 (± 1.3).
The DMFT index ranged from 0.3 to
5.5
Mozambique(5.5) had a risk 3.2
times higher than the average for the
region.
Tongo and Tanzania already had
lower than (0.3) the regional
average.

21Distribution of DMFT according to the countries of the African region

22
The Americas have 47
countries. However, only 40
countries had data on caries
at 12 years-old.
The DMFT index showed an
average of 2.4 (± 1.4).
The DMFT index ranged from 0.63
to 6.3
The highest levels found in Ecuador
and Martinique (6.3 and 5.2,
respectively). Belize and Haiti had
low (0.60 and 0.65 respectively).

23Distribution of DMFT according to the countries of the Americas
24
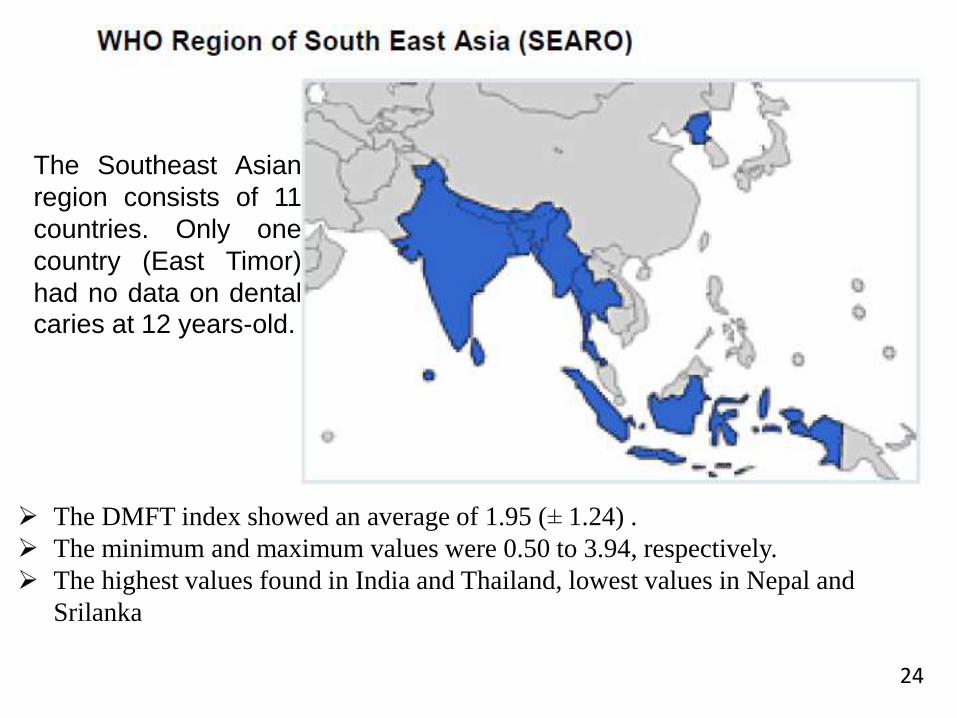
The Southeast Asian
region consists of 11
countries. Only one
country (East Timor)
had no data on dentalcaries at 12 years-old.
The DMFT index showed an average of 1.95 (± 1.24) .
The minimum and maximum values were 0.50 to 3.94, respectively.
The highest values found in India and Thailand, lowest values in Nepal and
Srilanka
25
WHO European Region (EURO)
The European region comprises 53 countries.
Data from 51 countries on dental caries in schoolchildren 12 years-old were
available
The mean DMFT index was
2.3 (± 1.3).
The index ranged from 0.7 to
7.8.
The highest values found in
Serbia and Montenegro,
lowest values in Germany
and UK

26
Distribution of DMFT according to
the countries of the Euro Region

27
The EMRO region 21
countries. Data on
caries was available for
20 countries
The average DMFT index found in the region was 2 (± 1.3).
The values ranged from 0.4 to 5.9.
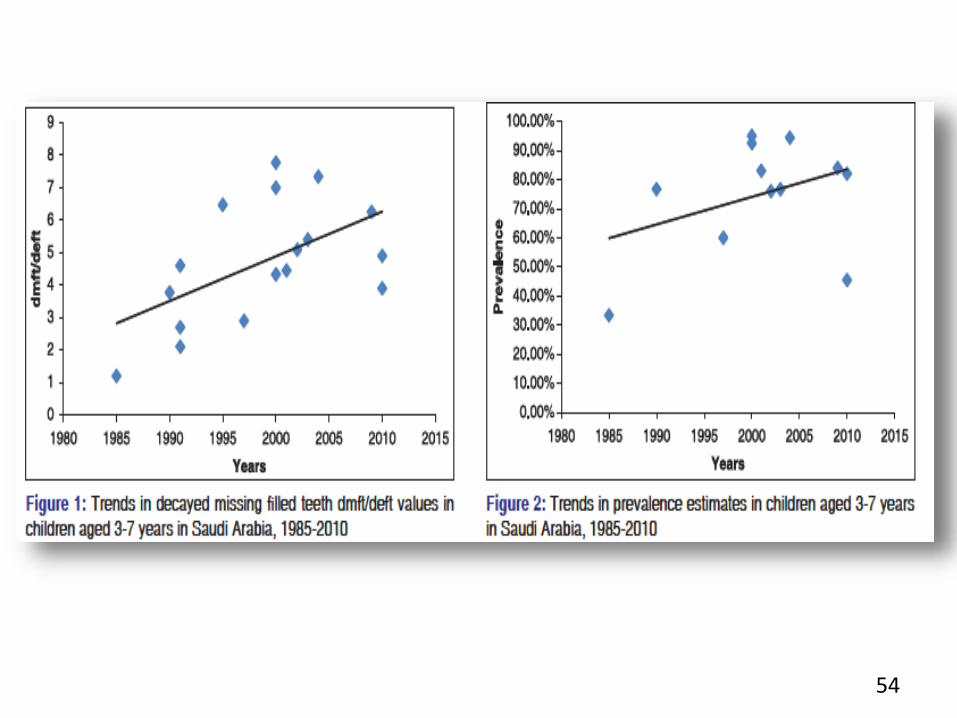
Saudi Arabia(5.90) had a risk 3 times higher than the average for the region
followed by Lebanon, Jordan and Yemen.
Lowest values in Sudan(0.25) and Egypt(0.20)
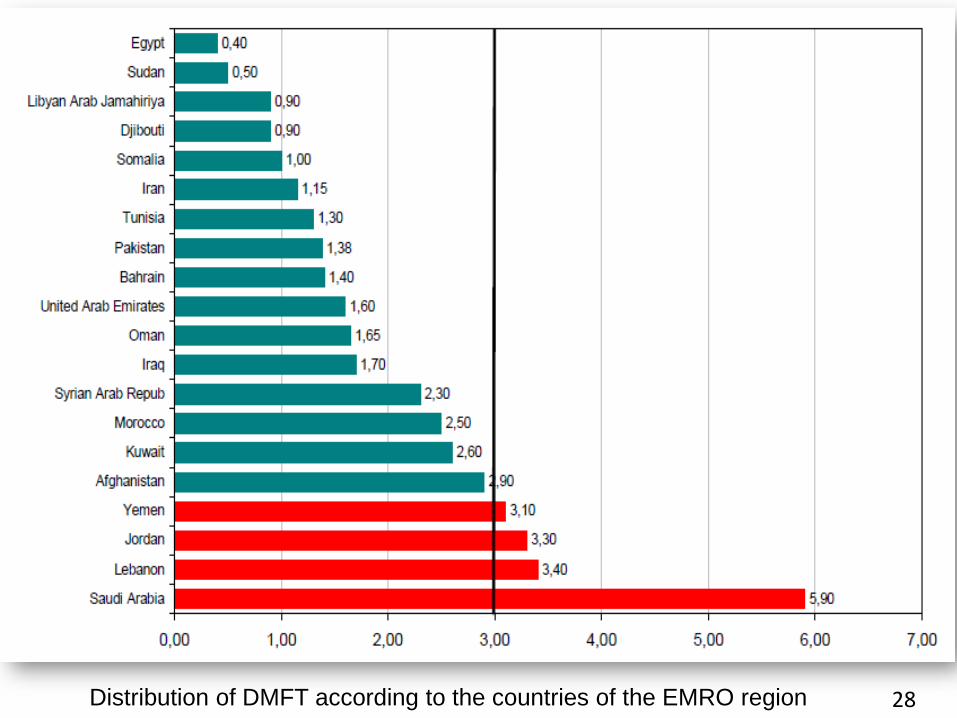
28Distribution of DMFT according to the countries of the EMRO region

29
The WPRO comprises 27 countries. Data
on caries was available for 24 countries in
the region.
The average DMFT index for the region was 1.93 (± 0.9).
DMFT values ranged from 1 to 5.
The highest values found in Brunei Darussalam followed by the
Republic of Korea and Tonga, Philippines, Solomon Islands and
Samoa.
Singapore, Kiribati, China and Australia showed a 52% lower risk.
30
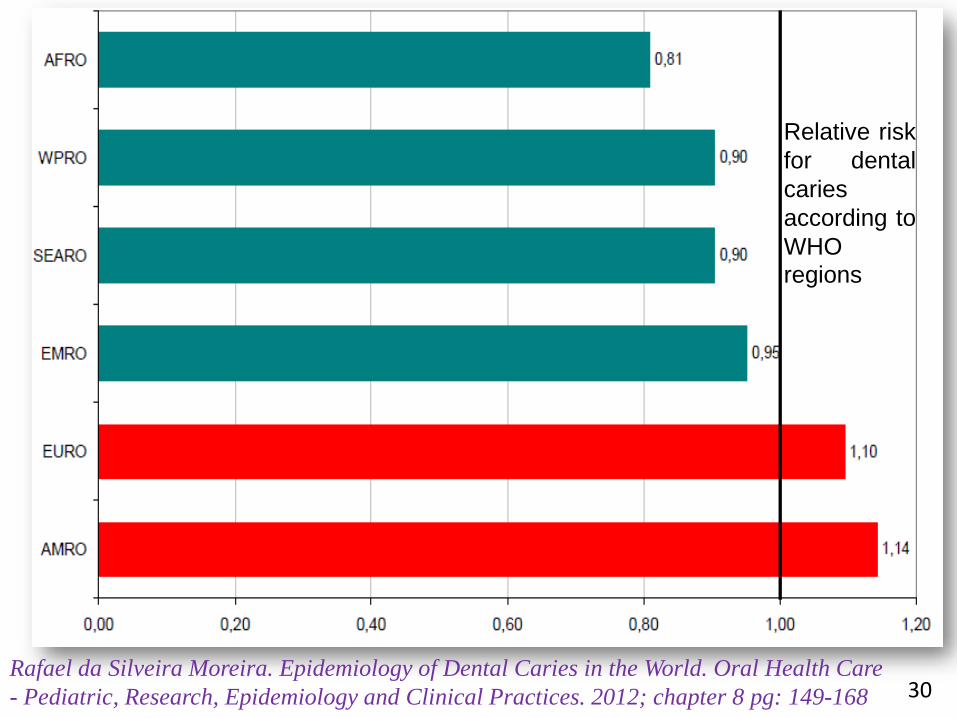
Relative risk
for dental
caries
according to
WHO
regions
Rafael da Silveira Moreira. Epidemiology of Dental Caries in the World. Oral Health Care
- Pediatric, Research, Epidemiology and Clinical Practices. 2012; chapter 8 pg: 149-168

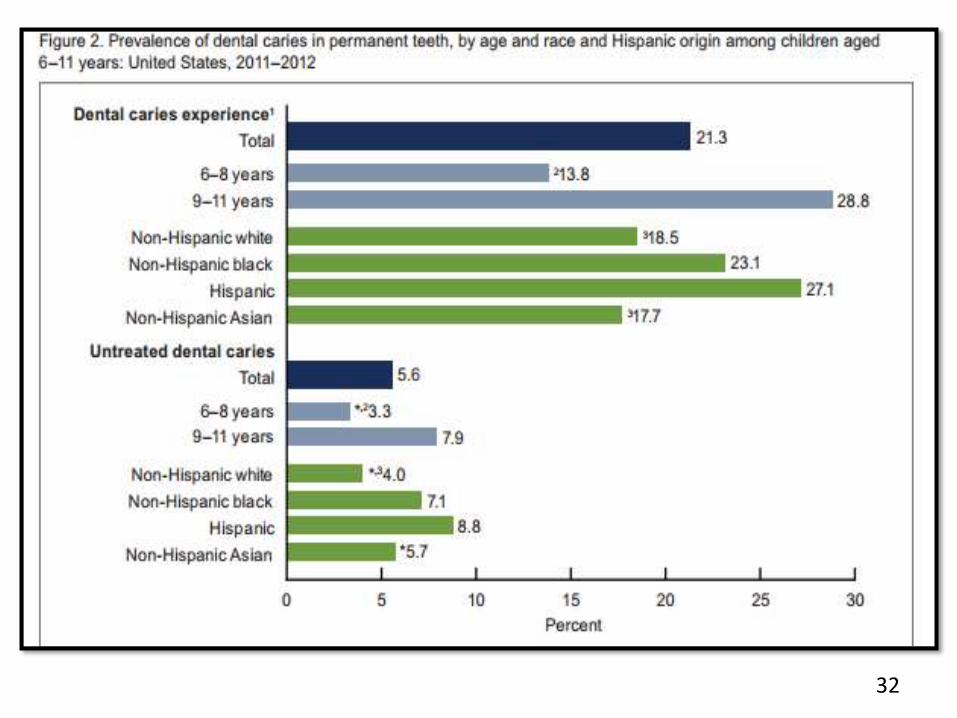
Bruce A. Dye et al
31
32
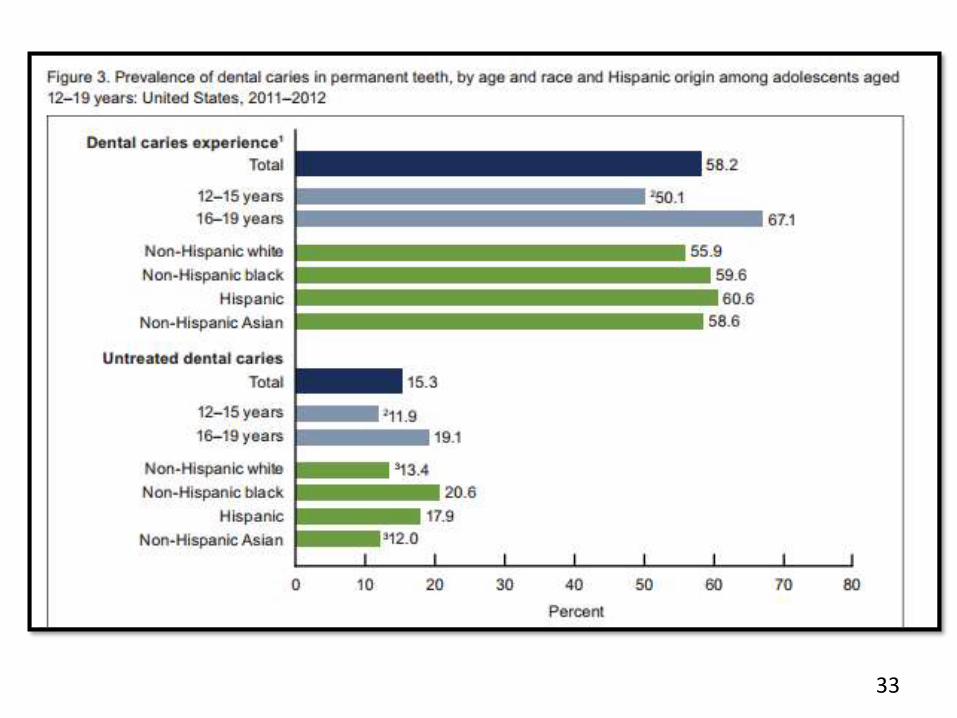
33

34

Laura Emma et al 2012,
3-year longitudinal analysis
35

The lower caries incidence in children, The relatively greater effect of fluorides in preventing caries on proximal surfacesThe slower rate of progression of caries, The increased risk of primary caries in adults, The increased use of fissure sealants.
36

According to the third national epidemiological investigation on oral diseases conducted in 2005, the caries prevalence rate of children aged between 5–6 years old remains high, people of 35–44 and 65–74 years experience high caries prevalence rate and low filling rate
37
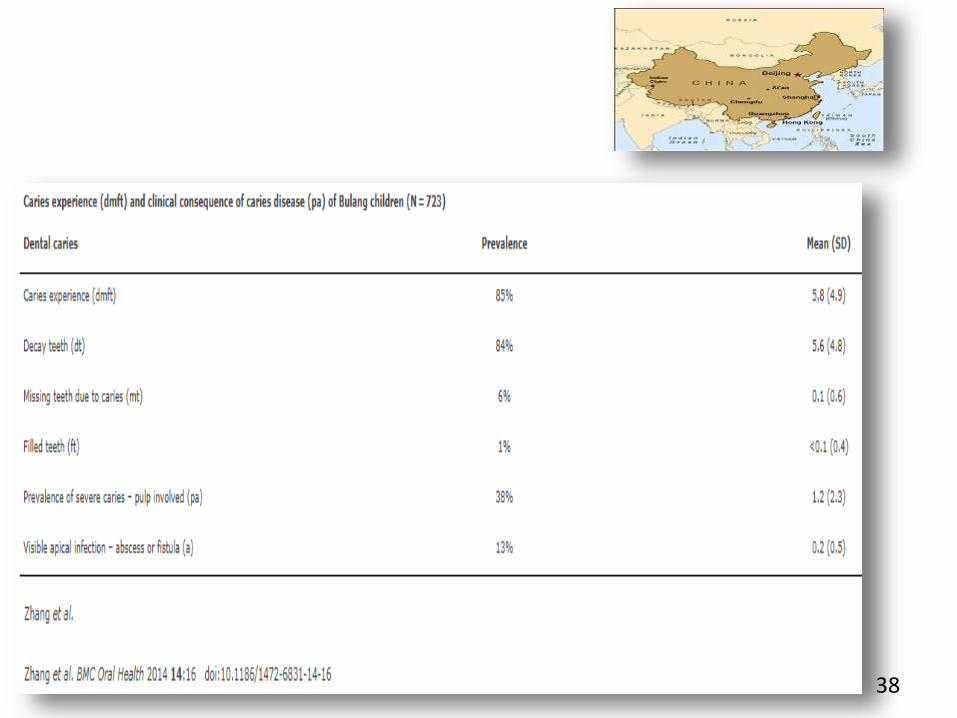
38

39
Lu Liu, Ying Zhang, Wei Wu, Min Cheng, Yan Li, Ruibo Cheng Prevalence and Correlates of Dental Caries in an Elderly Population in Northeast China PLoS One. 2013; 8(11): e78723.
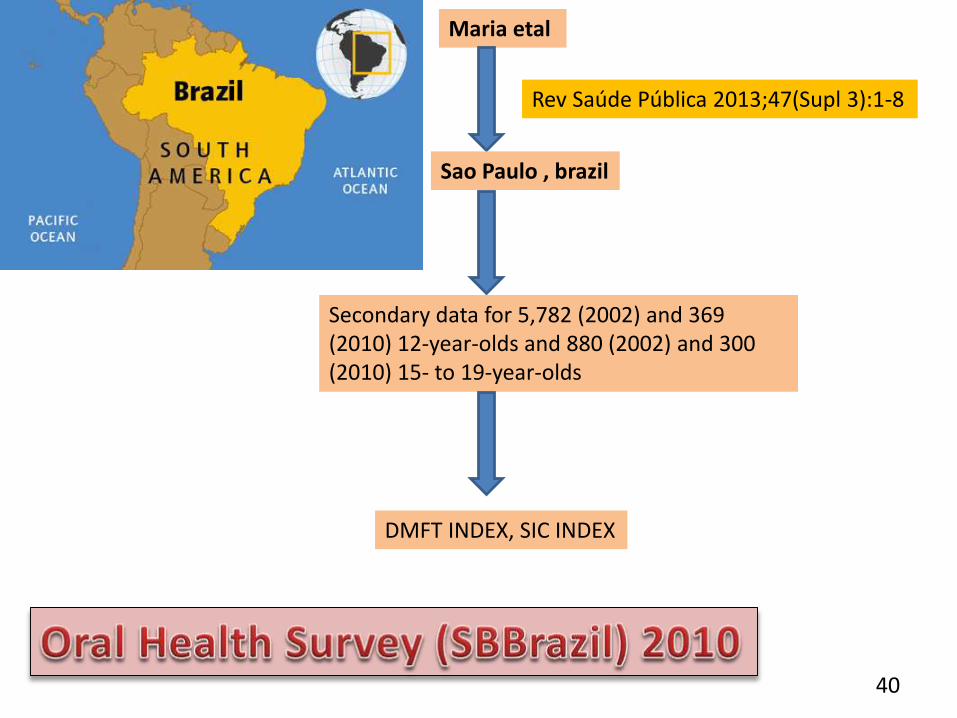
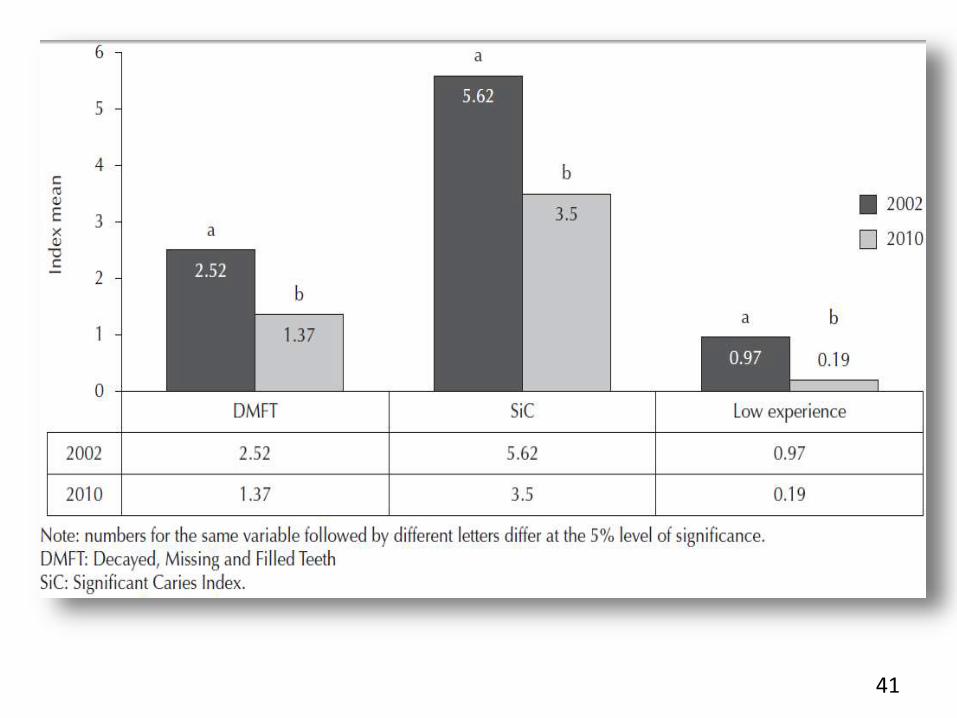
Maria etal
Sao Paulo , brazil
Secondary data for 5,782 (2002) and 369(2010) 12-year-olds and 880 (2002) and 300 (2010) 15- to 19-year-olds
Rev Saúde Pública 2013;47(Supl 3):1-8
DMFT INDEX, SIC INDEX
40
41

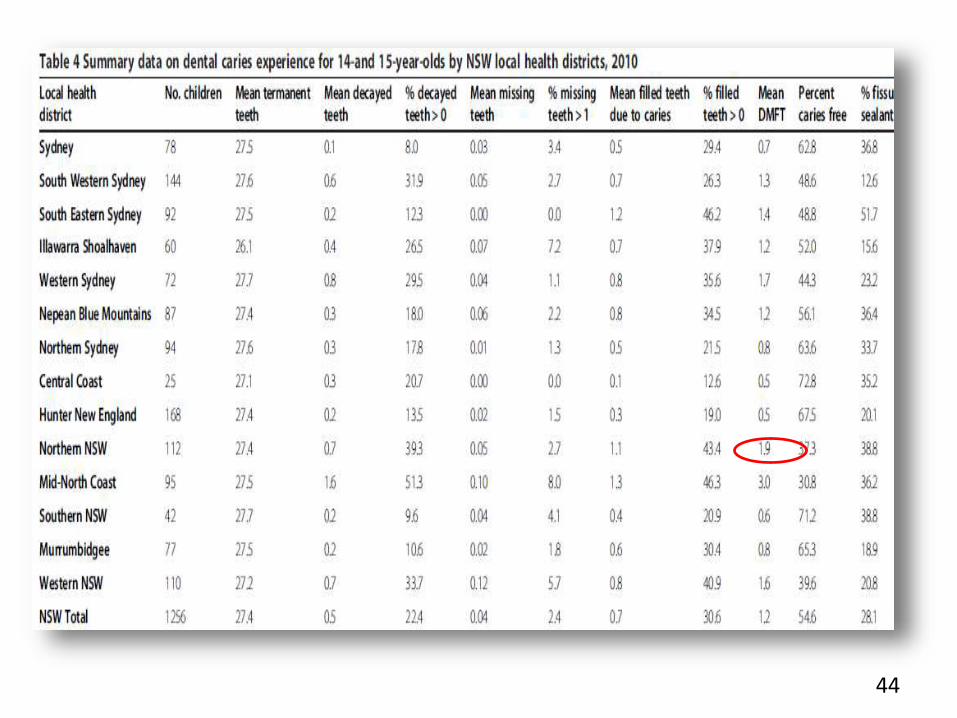
The New South Wales (NSW) TeenDental Survey 2010 is the majorsurvey undertaken by the Centrefor Oral Health Strategy.
42

19 calibrated examiners
1269 clinical examinations
14-15 years age
metropolitan and non-metropolitan schools
NSW Teen Dental Survey
2010 84 secondary schools
43
44

45

A survey of the dental health of children in England, Wales and Northern Ireland takes place every ten years. – NHS 2012
46,500 children and young people under 19 were admitted to hospital for aprimary diagnosis of dental caries. These numbers were highest in the five- tonine-year-old age group, which showed a 14 per cent increase between 2010–11
The second highest admissions in 2013–14 were for tonsillitis, with approximately 11,500 cases, making dental caries by far the most common reason for children aged between five and nine to be admitted to hospital.
46

47
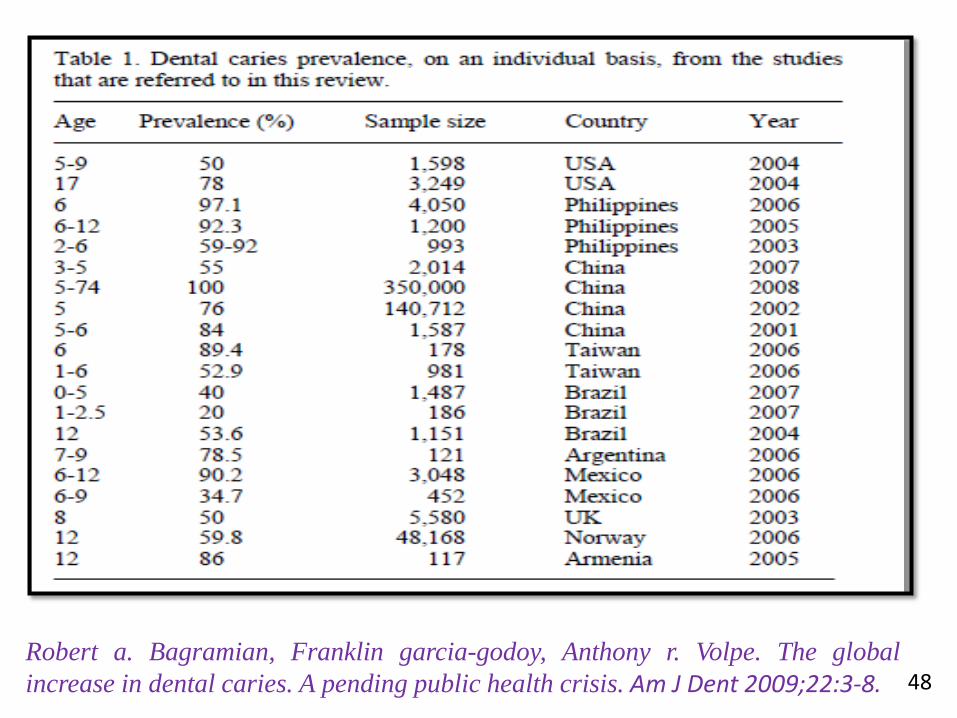
48Robert a. Bagramian, Franklin garcia-godoy, Anthony r. Volpe. The global
increase in dental caries. A pending public health crisis. Am J Dent 2009;22:3-8.

SHAMSHER ALI et al 2012
Sixteen hundred and seventy three poor locality school children aged 5-14 years; 1113, 5-11 years old and 560, 12-14 years old were examined for dental caries
49

WHO global data of 2003
DMFT of 12 years old Pakistani children from 0.9 to 1.38
2012
DMFT among 12-14 years 3.70
INCREASE IN CARIES PREVALENCE IS NOTICED.
50
51

Ambrina Qureshi et al ( 2014)
12-15 years attending government schools of Moradabad and Karachi cities of India and Pakistan
809 school children, 409 from India and 400 from Pakistan
Mean DMFT of India was found to be 1.9 ± 1.46 Pakistan was 1.00 ± 1.57.
An increase in decayed component in comparison to the overall DMFT in both the countries indicate the need of care, less utilization of available care, unavailability of care and ignorance
52
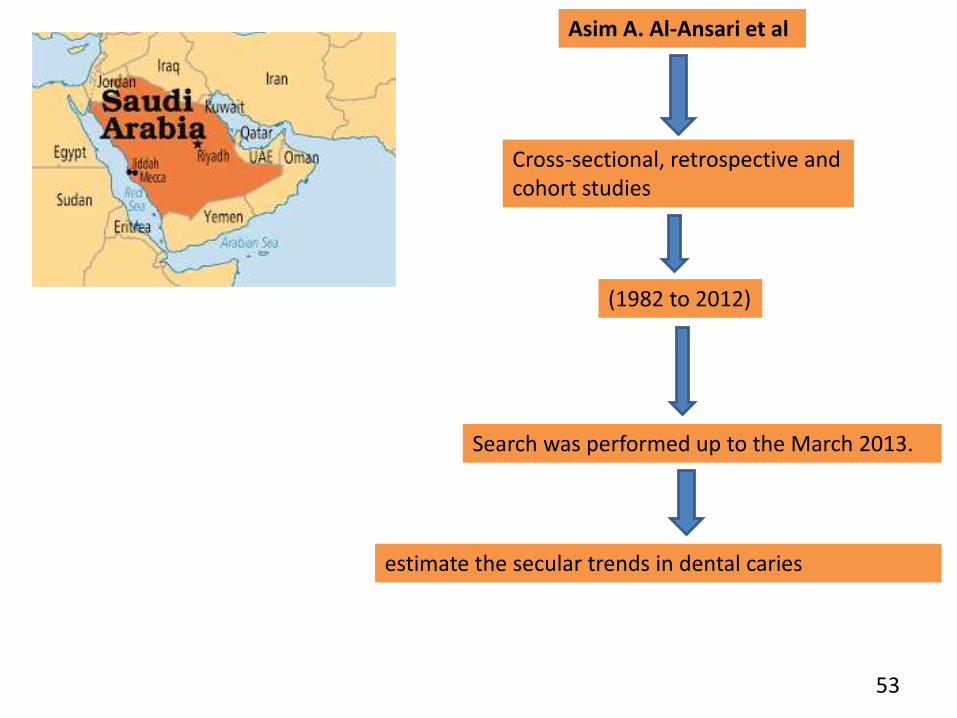
Cross-sectional, retrospective and cohort studies
Asim A. Al-Ansari et al
(1982 to 2012)
Search was performed up to the March 2013.
estimate the secular trends in dental caries
53
54

55

56

57
24th International Conference on
Dentistry & Oral Care
April 17-19, 2017 Dubai, UAE
Theme: Dentistry & Oral Care: A
vision for Excellence
$ 1400 Academic
$450 student with poster
International Dental Conference on
“Caries Control throughout Life in Asia”
November 20-22, 2013, Krabi, Thailand
Annual dental caries cases

Dental caries of 12-year-olds has been decreased more than 40% during the past decade.
58

Decreased birth rate and increased concern and care for children with their caregivers.
Increased access to dental care by increased number of dentists and dental clinics also may be a possible reason.
Korean professionals agree that the most important impact came from active oral health programs.
What made this caries reduction possible?
59

Harpreet Grewal,et al (2015)
three educational zones of urban Delhi, India
Central, South and North- West) of urban Delhi
520 children were surveyed comprising of 333 boys and 187 girls
60

61

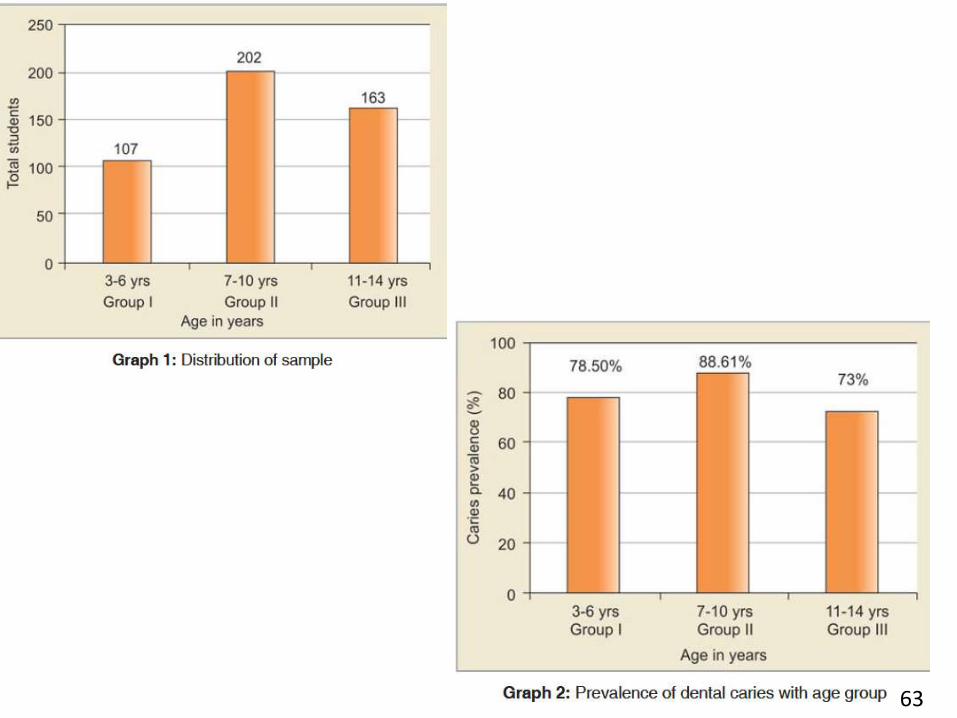
Poonam shingare et al ( 2012)
472 children of 3-14 yrs.
WHO CRITERIA – DENTAL CARIES
62
63

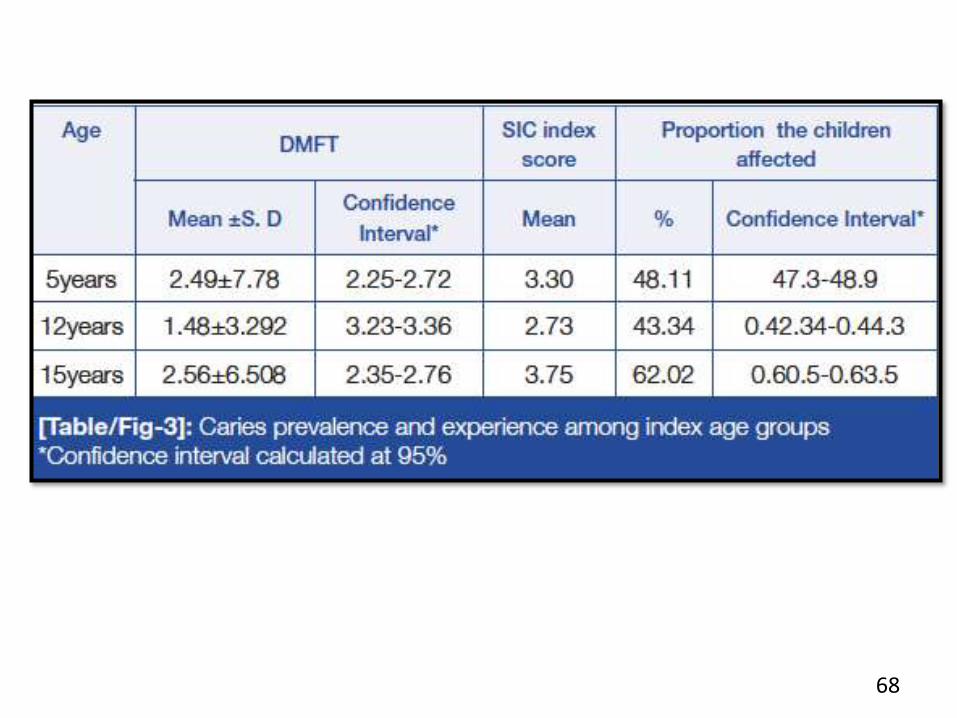
Articles from the past 15years reporting on dentalcaries prevalence andexperience in India weresearched and this onlinesearching strategy collectedand listed 781 articles.
Hansa kunduet al (2015)
64
Dental Caries ScenarioAmong 5, 12 and 15-Year-old Children in India- ARetrospective Analysis

65

66

67
68

69

70

Northern area was found to have more prevalence of dental caries as compared to the Southern region in all the index age groups.
The likely cause behind this could be attributed to the changing lifestyle and eating habits of population in Northern India
71

Most industrialized countries and countries of Latin America shows high DMFT
values(14 teeth or more), where as levels of dental caries experiences are
much lower in developing countries.
This pattern was the result of a no. of public health measures, including
effective use of fluorides, together with changing living conditions, lifestyles
and improved self care practices.
However, dental caries has not been eradicated, but only controlled to a
certain degree.
72

73
IMPLICATIONS FOR PREVENTION AND TREATMENT
The main conclusions that can be drawn from the different trends in industrialized
and underdeveloped countries are:
1. Sugars are implicated as the principal cause of dental caries. To achieve further
improvements in dental health in industrialized countries and prevent the increase in
caries in underdeveloped countries, a food policy directed at achieving an annual
per capita sugar intake of 10 kg or less in areas without water fluoride or fluoride
toothpastes is needed. In areas with fluoride, 15 kg of sugar/person/year will ensure
a low prevalence of dental caries.
2. Water fluoridation should be encouraged. Where this is not feasible for practical
or political reasons, salt fluoridation should be considered. In areas with optimal and
sub-optimal levels of fluoride in the drinking water, toothpastes should contain
fluoride. Other topical applications are not recommended when large percentages of
children are using fluoride toothpaste.
74
3. Because the rate of progression of dental caries is generally very slow and the
rate is even slower at the levels of caries being experienced in most industrialized
and underdeveloped countries, the intervals between dental check-ups should be
increased to two years for teenagers and to even longer intervals for adults. There
is no scientific basis for six monthly intervals between dental examinations.
4. Many fewer dentists than exist at present will be needed in industrialized
countries in future. Dental caries which do occur can easily be treated by dental
therapists. In future more therapists and fewer dentists, to deal with the more
complicated problems, will be required.

75
5. There are about 1500 million children in the world under the age of 15 years; 80%
of them are in underdeveloped countries. Every increase of 1.0 in the DMF would
require about 200 dental operators per million children. Even if the trend in dental
caries is halted, there will be a need for 1000000 dental personnel compared to the
present 200000. If the trend is not arrested, the need for dental personnel will be
much greater. The cost of training and employing such a dental workforce is beyond
the educational or financial capabilities of most underdeveloped countries.
Therefore, primary prevention aimed at controlling the availability of refined sugars
and sugar containing foods, drinks and sweets is needed.
6. The effectiveness of dental health education will be greatly enhanced if sugar
control, sensible use of fluoride and oral cleanliness to reduce periodontal disease,
are encouraged by all primary health care workers.
Aubrey Sheiham. Changing trends in dental caries. International Journal of Epidemiology.1984;13(2):142-147.

76
Harris et al. (2004) identified 106 factors which were significantly related to the
prevalence or incidence of caries. Among these factors, the ones that are more
important for planning caries prevention programs include reduction in the
frequency of sugary food/drink intake, good or supervised brushing/cleaning of
teeth, and less use of feeding bottle especially when going to bed at night. The
above should be included in the key messages in ORAL HEALTH EDUCATION
programs for parents and caretakers of young children.
restriction of sugars consumption and increasing consumption of staple starchy
foods, fresh fruit and vegetables will decrease risk of dental caries.
(1) Use iodized salt. Do not consume too much salt;
(2) Eat less sugar. Children and adults should not eat cake, candy, soft drinks
before a meal. One person should consume only 500g sugar per month on
average;
(3) Drink soy milk. Increase consumption of the calcium-rich foods such as
milk, dairy products, and small fish.
VIETNAM

77
SEARO published In Thailand, sugar consumption increasing intake from 150 to
200 grams per day, and in India, from 50 to 100 grams per day.
WHO 2012
The per capita consumption of sugar in India is 20.2kg. This is lower than the global average is 24.8 kgBut in the last 50 years sugar consumption in India has gone up from 5% to 13% .
Global Agricultural Information Network, 2016
• Northern area was found to have more prevalence of dental caries as compared tothe Southern region in all the index age groups (5,12, 15, 35-44, 65-74).
* The likely cause behind this could be attributed to the changing lifestyle andeating habits of population in Northern India .
Hansa kundu et al (2015)

References:-
78
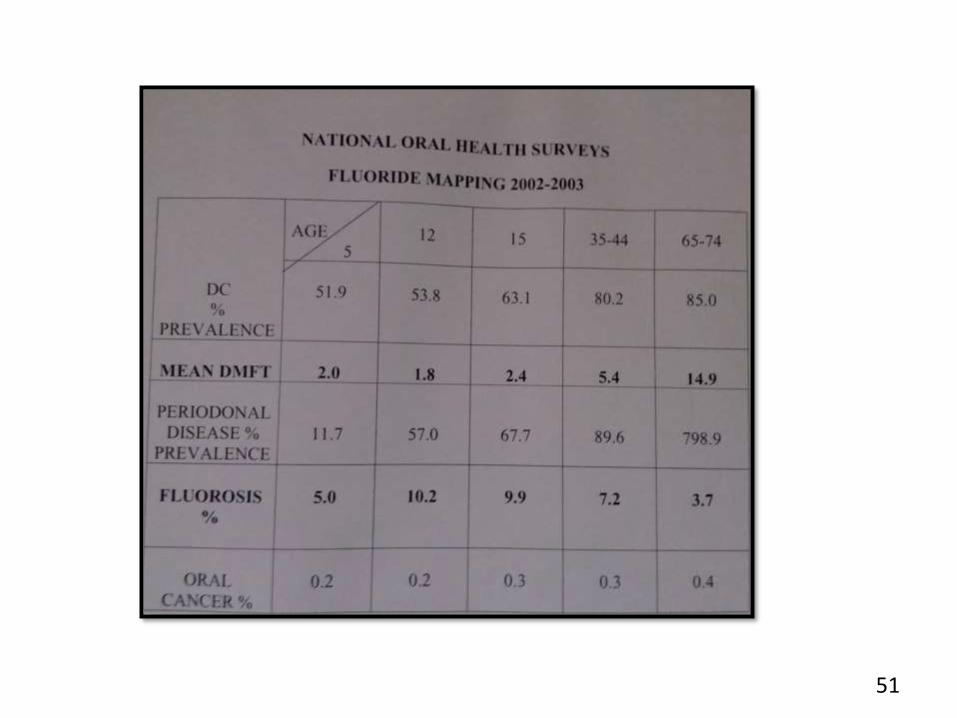
1. Bali RK, Mathur VB, Talwar PP, Chanana HB. National oral health survey and
fluoride mapping 2002-03 India.
2. Robert a. Bagramian, Franklin garcia-godoy, Anthony r. Volpe. The global
increase in dental caries. A pending public health crisis. Am J Dent
2009;22:3-8.
3. Harpreet Grewal, Mahesh Verma, Ashok Kumar. Prevalence of dental caries
and treatment needs amongst the school children of three educational
zones of urban Delhi, India Indian J Dent Res. 2011; 22(4); 517-519.
4. Poonam shingare et al dental caries prevalence among 3 to 14 years old
school children ,Uran, Raigad District, Maharastra. J Contemp Dent. May –
August 2012;2(2):11-14.
5. World Health Organization. Oral Health. Fact sheet no 318. April 2012.
Available at: www.who.int/mediacentre/ factsheets/fs318/en/index.htm.
6. Shamsher ali et al prevalence of dental caries among 5-14 years old poor
locality school children of Lahore. Pakistan oral & dental
journal.2012;32(2);279-282.
7. Rafael da Silveira Moreira. Epidemiology of Dental Caries in the World. Oral
Health Care - Pediatric, Research, Epidemiology and Clinical Practices.
2012; chapter 8 pg: 149-168
8. Marcenes W, Kassebaum NJ, Bernabe E, Flaxman A, Naghavi M, Lopez
A, Murray CJ. Global burden of oral conditions in 1990-2010: a systematic
analysis. J Dent Res. 2013 Jul;92(7):592-7.
9. Public Health England. National Dental Epidemiology Programme for
England: oral health survey of five-year-old children 2012. A report on the
prevalence and severity of dental decay. London: PHE; 2013.
79
10. Lu Liu, Ying Zhang, Wei Wu, Min Cheng, Yan Li, Ruibo Cheng Prevalence and
Correlates of Dental Caries in an Elderly Population in Northeast China PLoS
One. 2013; 8(11): e78723.
11. Maria da et al Dental caries and treatment needs in adolescents from the
state of Sao Paulo, Brazil Rev Saúde Pública 2013;47(Supl 3):1-8.
12. Shinan Zhang, Juan Liu, Edward CM Lo, and Chun-Hung Chu Dental caries
status of Bulang preschool children in Southwest China .BMC Oral Health.
2014; 14: 16.
13. Aubrey Sheiham et al A reappraisal of the quantitative relationship between
sugar intake and dental caries: the need for new criteria for developing goals
for sugar intake. BMC Public Health,2014; 14:863
14. Eduardo Bernabé et al Extent of differences in dental caries in permanent
teeth between childhood and adulthood in 26 countries. Int Dent J.
2014;64(5); 241–245. 80
81
15. Ambrina Qureshi et al Oral Health Disparities Among 12- 15 Years
Children Of India And Pakistan – A Cross Border Comparison. JPDA;
2014: 23(4).
16. Asim A. Al-Ansari et al (2015) Prevalence, severity, and secular trends of
dental caries among various saudi populations: A literature review.saudi
journal of medicine and medical sciences. 2014; 2(3): 142-150
17. Hansa kundu et al Dental Caries Scenario Among 5, 12 and 15-Year-old
Children in India- A Retrospective Analysis.Journal Of Clinical And
Diagnostic Research 2015 Jul, Vol-9(7): ZE01-ZE05.
18. http://www.health.nsw.gov.au/oralhealth/Pages/teen-dental-survey.aspx.
Last accessed on 19 Jan 2017
19. FDI World Dental Federation [email protected]
www.fdiworldental.org Last accessed on Jan 30 2017

82