Embed Size (px)
Citation preview

Control of BreathingControl of Breathing
RESPIRATORYCENTRE (Medulla)
MEDULLARY &CAROTID
CHEMORECEPTORS
Higher Control Centres
RESPIRATORYREFLEXES
DRUG EFFECTS e.g.OPIATES & CAFFEINE
CRANIAL & SPINALMOTOR NEURONES
STRETCH & PROPRIOCEPTORSLUNGS & CHEST WALL
INSPIRATION

ChemoreceptorsChemoreceptors
Medulla Oblongata and Carotid BodyMedulla Oblongata and Carotid BodyRespond to changes in pH, CORespond to changes in pH, CO22 and O and O22
Resetting of carotid chemoreceptors Resetting of carotid chemoreceptors occurs at birth in response to oxygenationoccurs at birth in response to oxygenation
Not essential at initiation of respiration but Not essential at initiation of respiration but used for control of breathing used for control of breathing
Responses are weak in the immediate Responses are weak in the immediate newborn period and in preterm babiesnewborn period and in preterm babies

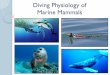
Response to HypoxiaResponse to Hypoxia
Breathing Efforts
+
-
Time in Minutes
Older Infant
Fetus
Preterm baby
Term baby
5 mins

Respiratory ReflexesRespiratory ReflexesHering-Breuer reflexesHering-Breuer reflexes
Lung inflation Lung inflation → inhibition of breathing→ inhibition of breathingProlonged inhalation → expiratory muscle contractionProlonged inhalation → expiratory muscle contractionRapid deflation → prolonged inspiratory responseRapid deflation → prolonged inspiratory response
Head’s paradoxical reflexHead’s paradoxical reflexRapid inflation Rapid inflation → diaphragmatic contraction (sigh)→ diaphragmatic contraction (sigh)
Intercostal phrenic inhibitory reflexIntercostal phrenic inhibitory reflexChest wall distortion Chest wall distortion → shallow inspiratory efforts→ shallow inspiratory efforts
Irritant reflexesIrritant reflexesUpper airway reflexesUpper airway reflexes
Nasal irritation/ suction Nasal irritation/ suction → apnoea→ apnoeaLiquid in larynx → apnoeaLiquid in larynx → apnoea

Lung MechanicsLung Mechanics
Total lung capacityTotal lung capacity Tidal volumeTidal volume Functional residual Functional residual
capacitycapacity Vital capacityVital capacity Inspiratory & expiratory Inspiratory & expiratory
reserve volumesreserve volumes Residual volume Residual volume

DefinitionsDefinitionsTidal volume = volume of gas each breathTidal volume = volume of gas each breath
5 - 7 mL/Kg in babies 5 - 7 mL/Kg in babies Minute volume = vol. of gas each minuteMinute volume = vol. of gas each minute
200 – 400 mL/kg/min200 – 400 mL/kg/min
Minute volume = Tidal volume x resp. rateMinute volume = Tidal volume x resp. ratePaCO2 inversely PaCO2 inversely MV MV
PaCO2 PaCO2 ↓↓ by by ↑ tidal volume or ↑ resp. rate↑ tidal volume or ↑ resp. rateDead Space = Vol. of lung not involved in Dead Space = Vol. of lung not involved in
ventilation (eg, airways and ET tubes)ventilation (eg, airways and ET tubes)

ComplianceCompliance Compliance is a measure of the distensibility of Compliance is a measure of the distensibility of
the lungthe lung
Compliance = Compliance = Change in Volume (L)Change in Volume (L)
Change in Pressure (cm HChange in Pressure (cm H22O)O)
Lung disease decreases complianceLung disease decreases compliance RDSRDS (Alveolar collapse)(Alveolar collapse) TTNTTN (Fluid in insterstitium)(Fluid in insterstitium) BPDBPD (Lung fibrosis)(Lung fibrosis) Pneumothorax (Lung compression)Pneumothorax (Lung compression)
Surfactant improves compliance Surfactant improves compliance (beware over distension)

Airways ResistanceAirways ResistanceMeasure of the pressure gradient needed Measure of the pressure gradient needed
for gas to flow through a tubefor gas to flow through a tubeAirway resistance = Airway resistance = Pressure differencePressure difference
(R(RAWAW)) Gas flowGas flow
• Poiseuilles’ equationPoiseuilles’ equation• RRAWAW airway length airway length
• RRAWAW 1/ radius 1/ radius44
• Small & long ET tubesSmall & long ET tubes• Subglottic stenosisSubglottic stenosis

Work of BreathingWork of BreathingEnergy required to produce change in lung Energy required to produce change in lung
volumevolume Increases with decreased complianceIncreases with decreased compliance Increases with increased resistanceIncreases with increased resistance
If energy required to breath exceeds If energy required to breath exceeds capacity to supply oxygen to provide that capacity to supply oxygen to provide that energy then respiratory failure develops energy then respiratory failure develops requiring mechanical ventilationrequiring mechanical ventilation

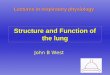
Pressure Volume CurvesPressure Volume Curves(Lung hysteresis loops)(Lung hysteresis loops)
PRESSURE
VOLUME
INSP
EXP

Pressure Volume CurvesPressure Volume Curves(Lung hysteresis loops)(Lung hysteresis loops)
PRESSURE
VOLUME
LOW COMPLIANCE
HIGH COMPLIANCE

Pressure Volume CurvesPressure Volume Curves(Lung hysteresis loops)(Lung hysteresis loops)
PRESSURE
VOLUME
LOWERRESISTANCE
HIGHERRESISTANCE

Questions on Anatomy Questions on Anatomy & Physiology& Physiology
??

Neonatal respiratory diseaseNeonatal respiratory diseaseAims:-Aims:-
Overview of neonatal respiratory diseaseOverview of neonatal respiratory diseasePathophysiologyPathophysiologyClinical presentationClinical presentationAetiologyAetiologyX-ray appearancesX-ray appearancesTreatmentsTreatments

Hyaline membrane diseaseHyaline membrane diseaseClinical:-Clinical:-
Usually pretermUsually pretermTachypnoea > 60Tachypnoea > 60 Indrawing/ retraction/ recessionIndrawing/ retraction/ recessionGruntingGruntingNasal flaringNasal flaringCyanosis in airCyanosis in airPresents within a few hours of lifePresents within a few hours of life


HMD - AetiologyHMD - Aetiology
Surfactant deficiencySurfactant deficiencyStructurally immature lungsStructurally immature lungs

HMD - TreatmentHMD - Treatment
OxygenOxygenCPAPCPAPMechanical ventilationMechanical ventilationSurfactant replacementSurfactant replacement

TTNTTNClinical:-Clinical:-
Usually close to termUsually close to termTachypnoea 100-120/minTachypnoea 100-120/minOverinflated chestOverinflated chestNo grunting/ retractionNo grunting/ retractionSettles within 24-48 hoursSettles within 24-48 hours

TTN - AetiologyTTN - Aetiology
Delayed fetal lung fluid clearanceDelayed fetal lung fluid clearanceCaesarean section - no squeeze of thorax Caesarean section - no squeeze of thorax
at birthat birthMum not in labour - no catecholamine Mum not in labour - no catecholamine
surge to promote absorption of fetal lung surge to promote absorption of fetal lung fluidfluid


TTN - treatmentTTN - treatment
Prevention - avoid early elective Prevention - avoid early elective caesarean sections at termcaesarean sections at term
Oxygen supplementation and IV fluids until Oxygen supplementation and IV fluids until resolutionresolution

Airleak SyndromesAirleak Syndromes
PneumothoraxPneumothoraxPneumomediatinumPneumomediatinumPneumopericardiumPneumopericardiumPulmonary interstitial emphysemaPulmonary interstitial emphysema

PneumothoraxPneumothoraxClinical:-Clinical:-
May be asymptomaticMay be asymptomaticMay be life threateningMay be life threateningSudden deterioration in gas exchangeSudden deterioration in gas exchangePoor colourPoor colourHypotension and tachycardiaHypotension and tachycardiaUnilateral overexpanded thoraxUnilateral overexpanded thorax


Pneumothorax - aetiologyPneumothorax - aetiology
Uneven alveolar ventilationUneven alveolar ventilationAir trapping and high pressure swingsAir trapping and high pressure swingsTracking of air from pulmonary interstitial Tracking of air from pulmonary interstitial
emphysemaemphysema

Pneumothorax - predisposing Pneumothorax - predisposing factorsfactors
Spontaneous in 1% of all babiesSpontaneous in 1% of all babies Increases with mechanical ventilationIncreases with mechanical ventilation Increased x 4 with HMDIncreased x 4 with HMD Increased x 16 with CPAPIncreased x 16 with CPAP Increased x 34 with IPPVIncreased x 34 with IPPV

Pneumothorax - preventionPneumothorax - preventionEarly surfactant therapyEarly surfactant therapyAvoid overdistensionAvoid overdistension
Volume guaranteeVolume guaranteeLow PIPLow PIP
Short inspiratory timeShort inspiratory timeFaster ventilation rates - entrainmentFaster ventilation rates - entrainmentHFOVHFOVTrigger ventilation - no proven benefitTrigger ventilation - no proven benefitParalysis - no proven benefitParalysis - no proven benefit

Pneumothorax - TreatmentPneumothorax - Treatment
None if asymptomaticNone if asymptomaticNitrogen washout technique - high FiO2 in Nitrogen washout technique - high FiO2 in
term babies onlyterm babies onlyChest drain if tension pneumothorax or on Chest drain if tension pneumothorax or on
mechanical ventilationmechanical ventilationEmergency needle thoracocentesisEmergency needle thoracocentesis

Pulmonary interstitial Pulmonary interstitial emphysemaemphysema
Mainly occurs in preterm babies ventilated Mainly occurs in preterm babies ventilated for HMDfor HMD
Gas trapping in perivascular sheathsGas trapping in perivascular sheaths Increased incidence at lower gestationsIncreased incidence at lower gestations


PIE - Clinical featuresPIE - Clinical features
Severe hypoxaemia and CO2 retentionSevere hypoxaemia and CO2 retentionDeteriorating clinical conditionDeteriorating clinical condition
X- RayX- RayOverinflation with gross cystic changesOverinflation with gross cystic changes

PIE - TreatmentPIE - Treatment
Lower PEEP and PIPLower PEEP and PIPParalysisParalysisHigh rate low pressure ventilationHigh rate low pressure ventilation? HFOV? HFOV? Selective bronchial intubation? Selective bronchial intubation

Persistent pulmonary Persistent pulmonary hypertension of the newbornhypertension of the newborn
Clinical featuresClinical features
Severe hypoxaemia (cyanosed in 100% O2)Severe hypoxaemia (cyanosed in 100% O2)No severe lung diseaseNo severe lung diseaseEvidence of R to L shunt (pre vs. postductal)Evidence of R to L shunt (pre vs. postductal)Structurally normal heartStructurally normal heart

PPHN - Aetiology and PPHN - Aetiology and predisposing factorspredisposing factors
Failure of NO synthaseFailure of NO synthaseAsphyxia/ acidosisAsphyxia/ acidosis InfectionInfectionDiaphragmatic herniaDiaphragmatic herniaAlveolar capillary dysplasiaAlveolar capillary dysplasiaMeconium aspiration syndromeMeconium aspiration syndrome

PPHN - treatmentPPHN - treatment
Minimal handlingMinimal handling Inotropic supportInotropic supportVentilation - maintain low normal CO2Ventilation - maintain low normal CO2ParalysisParalysisHyperventilation - ? Risk of PVLHyperventilation - ? Risk of PVLHFOVHFOVNitric OxideNitric OxidePulmonary vasodilators Pulmonary vasodilators
Tolazoline/ Prostacyclin/ MgSO4Tolazoline/ Prostacyclin/ MgSO4

Meconium aspiration syndromeMeconium aspiration syndromeClinical:Clinical:
Meconium passage prior to deliveryMeconium passage prior to deliveryMeconium in pharynx and tracheaMeconium in pharynx and tracheaRespiratory distress post delivery with Respiratory distress post delivery with
typical X-ray changestypical X-ray changes



MAS - AetiologyMAS - Aetiology
Asphyxia and intrauterine stressAsphyxia and intrauterine stressPassage of meconium + gasping Passage of meconium + gasping
movementsmovements Inhalation usually prior to deliveryInhalation usually prior to delivery

MAS - effects of meconiumMAS - effects of meconium
Ball valve effect - air trappingBall valve effect - air trappingChemical irritation and pneumonitisChemical irritation and pneumonitisSuperinfection with bacteriaSuperinfection with bacteriaSurfactant inhibitionSurfactant inhibition

MAS - ManagementMAS - Management
Prevention in delivery suitePrevention in delivery suiteMinimal handlingMinimal handlingMaintain normoxaemiaMaintain normoxaemiaMay need ventilation + ? ParalysisMay need ventilation + ? ParalysisSurfactant lavageSurfactant lavageAntibioticsAntibiotics

Pulmonary haemorrhagePulmonary haemorrhageClinicalClinical
Sudden deteriorationSudden deteriorationCopious bloody secretions from airwayCopious bloody secretions from airwayHypotensionHypotensionPallorPallorHypoxaemiaHypoxaemia



Pulmonary haemorrhage -Pulmonary haemorrhage -AetiologyAetiology
Usually pretermUsually pretermHMD with PDAHMD with PDAPost surfactant therapyPost surfactant therapyCoagulopathyCoagulopathyCongestive cardiac failureCongestive cardiac failure

Pulmonary haemorrhage - Pulmonary haemorrhage - TreatmentTreatment
Ventilation with high PEEPVentilation with high PEEPSurfactantSurfactant Indomethacin for PDAIndomethacin for PDATreat coagulopathyTreat coagulopathy

Chronic lung diseaseChronic lung diseaseClinicalClinical
Protracted respiratory insufficiency and Protracted respiratory insufficiency and oxygen requirement beyond 28th day or oxygen requirement beyond 28th day or 36th week post conceptional age36th week post conceptional age
Very preterm with early ventilation for Very preterm with early ventilation for HMDHMD

CLD - AetiologyCLD - Aetiology
VentilationVentilationOxygen toxicityOxygen toxicityPROMPROMChorioamnionitisChorioamnionitis InflammationInflammationProteolytic enzymesProteolytic enzymes

CLD - preventionCLD - prevention
Minimise ventilation and oxygen exposureMinimise ventilation and oxygen exposureHFOVHFOVEarly surfactantEarly surfactantCorticosteroids Corticosteroids Early extubationEarly extubation

CLD treatmentCLD treatment
Minimise ongoing barotraumaMinimise ongoing barotraumaNutritionNutritionPermissive hypercapniaPermissive hypercapniaDiureticsDiureticsBronchodilatorsBronchodilatorsCorticosteroids - controversialCorticosteroids - controversialHome oxygen therapyHome oxygen therapy

SummarySummary Knowledge of respiratory anatomyKnowledge of respiratory anatomy Physiology of adaptation at birthPhysiology of adaptation at birth SurfactantSurfactant Gas exchangeGas exchange Gas transportGas transport Lung mechanicsLung mechanics
Application of knowledge to the clinical Application of knowledge to the clinical management of babies with respiratory diseasemanagement of babies with respiratory disease