Embed Size (px)
Citation preview

Management of Well Differentiated Thyroid Cancer
Vivek Ramarathnam, M.D.
SIU- Otolaryngology
Grand Rounds
9/1/2005

Thyroid Nodules
Between 4-7% of individuals in US have palpable thyroid nodules
More common in women Increase in frequency with age Fewer than 10% of solitary nodules are
malignant- Papillary (75%)- Follicular (15%)

Thyroid Carcinoma
1.5% of all newly diagnosed cancers Number increasing over last 25 years;
4.8 to 8.0 cases per 100,000 Female predominance (11.7 female to 4.2
male cases/100,000 Death rate 0.5 cases per 100,000

Nodules and Carcinoma Rates
Rates of carcinoma in a single nodule: 5-17%
Rates of carcinoma in multinodular patients: 5-13%

Risk Factors for Malignancy
Prior irradiation Family history Male sex Nodules in individuals <15, >45 Symptoms of invasiveness: development of
hoarseness, progressive dyshagia, or dyspnea

Physical Examination
Pulse rate, Blood Pressure Neck Lymphadenopathy Deviation of Trachea Palpation of Thyroid gland(Size, consistency, mobility, presence or
absence of tenderness, multinodularity) Attention of thyroid mass to surrounding
anatomy

Preoperative Evaluation
Individuals with symptoms potentially of invasive carcinoma- dysphonia, dysphagia, or stridor
Flexible laryngoscopy MRI allows soft tissue evaluation (cervical
esophageal invasion) CT, readily available, iodinated contrast used can
delay the use of RAI postoperatively 4-6 weeks Selected patients, panendoscopy

Thyroid Picture

Thyroid Anatomy
Arteries- Paired arteries, superior, inferior arteries
Venous drainage- parallels arterial drainage, superior thyroid veins drain into internal jugular vein, inferior thyroid veins to brachiocephalics
Lymphatics- intraglandular lymphatic network, paratracheal, upper, mid, and lower jugular nodes

Thyroid Hormone Physiology
Growth- hormones work in bone formation CNS- brain maturation Basal metabolic rate Cardiovascular and respiratory systems Metabolic effects

Thyroid Histology

Thyroid Hormone Regulation
TSH stimulates both
iodine uptake and its organification

Management steps with a Thyroid Nodule
1. TSH level
- 95% of all nodules are hypofunctional (cold)
2. If TSH normal, obtain a ultrasound and perform FNA
- if firm and palpable FNA can be performed without image guidance

Ultrasound Imaging and Nodules
US reports thyroid size and appearance, 3D description of specific nodules, presence of paratracheal nodes, and evidence of invasive qualities.
Useful in individuals undergoing FNA and have difficult lesions to palpate.
Also beneficial in complex cysts, and nodules with questionable multinodularity

Management steps with a Thyroid Nodule
If TSH high, treat with thyroid hormone replacement and FNA when patient is euthyroid
TSH level low; may have hyperfunctioning nodule and should be evaluated with thyroid scan. Low likelihood of malignancy

Evaluation of solitary nodule
FNA (fine needle aspiration)
4 types of interpretations:
1) Benign
2) Malignant
3) Suspicious for follicular or Hurthle cell tumor
4) Insufficient for diagnosis

Overview of Nodule workup

Case Presentation
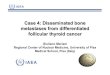
22 female referred for enlarging thyroid mass Right lobe of thyroid. Last year 2.8 cm and now 3.4 cm in greatest diameter. Complex mass described per US report. Otherwise asymptomatic. Mother- hyperthyroid. Medications: Effexor XR, Ortho patch
FNA- Cellular follicular lesion

Papillary Carcinoma

Follicular Carcinoma

Fine needle aspiration
Procedure requires skill by operator, as well as by cytopathologist
Even in skilled hands, approximately 10% of biopsy findings nondiagnostic
Sensitivity 92%, Specificity- 91-97.5%

Findings on FNA
Benign finding- Followed serially by US
If nodule has increased in size ~15%, repeat FNA should be performed
Follicular neoplasm- 80% of these nodules are benign, 20% represent thyroid carcinoma
Papillary carcinoma- accuracy of FNA approaches 100%

Fine needle aspiration
Suspicious for follicular or Hurthle cell tumor
Diagnosis of follicular of Hurthle cell tumor from follicular carcinoma or Hurthle cell carcinoma requires presence or absence of capsular or vascular invasion seen on histologic examination of surgical specimens
Follicular and Hurthle cell tumors diagnosed by FNA have malignancy rate of 10-20%

Case Presentation
Pt underwent Right lobectomy with isthmusectomy
Frozen section- Follicular neoplasm Final pathology- Follicular adenoma

Management of FNA results
Follicular neoplasm- Thyroid lobectomy, allow histiopathologic
diagnosis to dictate need for total- Serial US, TSH suppression, repeat FNA- Plan for lobectomy with frozen section, if
reveals follicular variant of papillary, perform total - Perform total thyroidectomy

Staging

Staging

5 year survival rates
Papillary Cancer Follicular Cancer
Stage 1 100% 100%
Stage 2 100% 100%
Stage 3 95.8% 79.4%
Stage 4 45.3% 47.1%

Risk Analysis
AGES (age, grade, extent, size) AMES (age, metastases (distant), extent,
size) MACIS (metastasis, patient age,
completeness of resection, local invasion, and tumor size)

AGES
Hay ID, et al. 61st American Thyroid Association Annual Meeting 1986
Papillary CAN= 860Age= 0.5 x ageGrade2 = 1Grade3-4 =3Extrathyroidal=1E(distant)= 3Size= 0.2 x cm

Hay ID, et al.

Surgical Management
Wein, RO, Weber RS, Contemporary Management of Differentiated Thyroid Carcinoma. Otolaryngol Clin N Am 2005
“ Surgery therapy for the majority of well-differentiated thyroid carcinomas should be tailored to the eradication of macroscopic disease while preserving the patient’s capacity for functional speech and swallowing and parathyroid preservation.”

Lobectomy vs. Total Thyroidectomy
Shaha AR, Shah JP, Loree TR Ann Surg Oncol 1997
Low risk patients need selective treatment Retrospective review of 1038 patients, 465
patients in low risk group, 403 patients papillary and 62 patients follicular
Median follow-up 20 years. No statistical difference in overall failure rate or local recurrence rate between lobectomy vs. total thyroidectomy

Reasons for Total Thyroidectomy
Hay ID et al. Surgery 1987
Removes not only the primary tumor but also microscopic contralateral disease ~80%
Prevents local recurrence (5-24%) or anaplastic (<1%) transformation in the contralateral lobe
Decreased need for 2nd operation with increased risk Thyroglobulin surveillance for recurrence Radioactive iodine scanning/therapy

Complications of Total Thyroidectomy
Hypoparathyroidism ~ 10% Recurrent laryngeal nerve paralysis ~1%

Sites of Invasive Spread
McCaffrey, TV et al. Mayo Clinic, 50-year experience. Head Neck 1994
Trachea 37%
Esophagus 21%
Recurrent laryngeal nerve 47%
Strap musculature 53%
Larynx 12%
Other structures 30%

Surgical Considerations
Tracheal involvement
- Window and sleeve resections
- Larger defects, sternocleidomastoid and pectoralis major myoperiosteal flaps over T-tubes
- Tracheal resection with re-anastomosis

Esophageal Invasion
Tends to invade only the outer muscular layers
Limited resection without intraluminal entry is posssible
When intraluminal invasion encountered, primary closure vs. free tissue transfer for larger resections

Recurrent laryngeal nerve
Falk SA, McCaffrey TV. Otolaryngol Head Neck Surg 1995
Retrospectively compared patients and noted that complete resection of tumor and nerve sacrifice offered no survival benefit over potentially incomplete resection of tumor and nerve preservation

Laryngeal Involvement
Vertical partial laryngectomy, unilateral disease
Supracricoid partial laryngectomy, extensive anterior invasion
Total laryngectomy, extensive laryngeal spread

Regional metastasis
Intraglandular lymphatics First nodal drainage paralaryngeal,
paratracheal, prelaryngeal nodes VI Second level of drainage II, III, IV, V Elective neck dissection in setting of papillary
CA will detect occult spread in 50% of patients; reported no added benefit on survival

Regional metastasis
Radiologic imaging for regional spread include US, CT, and MRI
US- most accurate when combined with FNA, Serial tests can evaluate changes in nodal size
Imaging criteria for CT/MRI: recurrent disease, clinical lymph node metastases, vocal cord paralysis, fixation of mass to adjacent structures, symptoms of upper aerodigestive involvement
Type of neck dissection dictated by extent of disease

Neck dissection
Ferlito A., Pellitteri PK, Robbins KT et al. Review article. Acta Otolaryngol 2002
Selective dissection for extension of tumor noted, direct involvement of non-lymphatic structures
In high risk patients (male >45, with large 4cm cancer) recommend ipsilateral paratracheal node dissection given highest risk of containing metastases
Low risk, palpate region if no enlarged lymph nodes, elective neck dissection not carried out

Postoperative treatment
Radioactive iodine ablation decreases the local recurrence and mortality rates in patients with stage 2 and stage 3 well-differentiated thyroid carcinoma
Use of postoperative RAI and thyroid hormone supression has been advocated for patients with tumors > 1.5 cm

Long term potential complications of Thyrotropin (TSH) Suppression
Increased bone loss, particularly in postmenopausal women
Hyperthyroidism Cardiac hypertrophy Cardiac arrythmias

Radioactive Iodine Side Effects
Radiation thyroiditis (when large remnant present), sialoadenitis, taste dysfunction, nausea

Postoperative Treatments
Thyroglobulin levels in the absence of normal
thyroid tissue, is a sensitive and specific marker for the presence of thyroid cancer
Ideally this assay should be performed when the thyrotropin (TSH) level is elevated
Recombinant human TSH Ongoing clinical surveillance

Postoperative followup
Woodrum DT, Gauger PG Journal of Surgical Oncology 2005

Other Therapies
Not first line therapy, external beam radiation may have a role in treatment of non-RAI avid tumors, gross residual tumor, or unresectable disease
Also clinical trials involving gene therapy and tumor redifferentiation research

Conclusions
Strategy for Thyroid Nodules Understanding prognosis- low, intermediate,
high risk Total Thyroidectomy and Radioiodine
Ablation for High Risk In the future, have more effective screening
and therapies