Embed Size (px)
Citation preview
THE PROCESS OF HEALTH REFORM IN PERU
JOSÉ CARLOS DEL CARMEN SARA

Why a Health Reform?
We want to eliminate restrictions that keep people from excercising their
RIGHT TO HEALTH
Establishes the path towards a health system
that is UNIVERSAL, EQUITABLE AND SOLIDARY
The Reform answers to an
ACCUMULATION PROCESS
The Reform PROMOTES
CORRESPONSABILITY
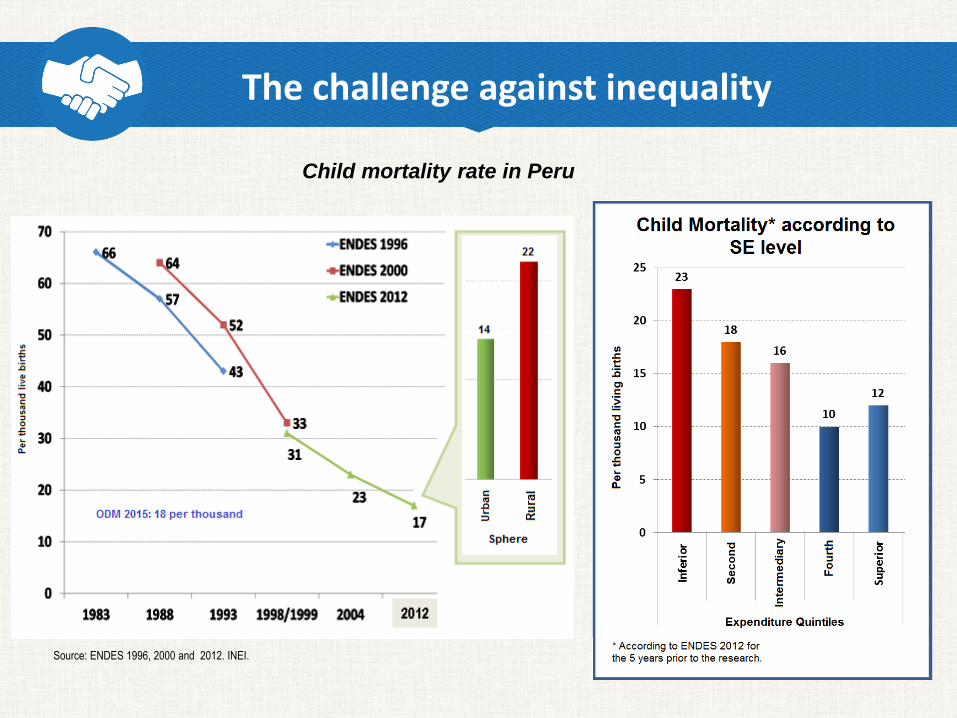
The challenge against inequality
Source: ENDES 1996, 2000 and 2012. INEI.
Child mortality rate in Peru
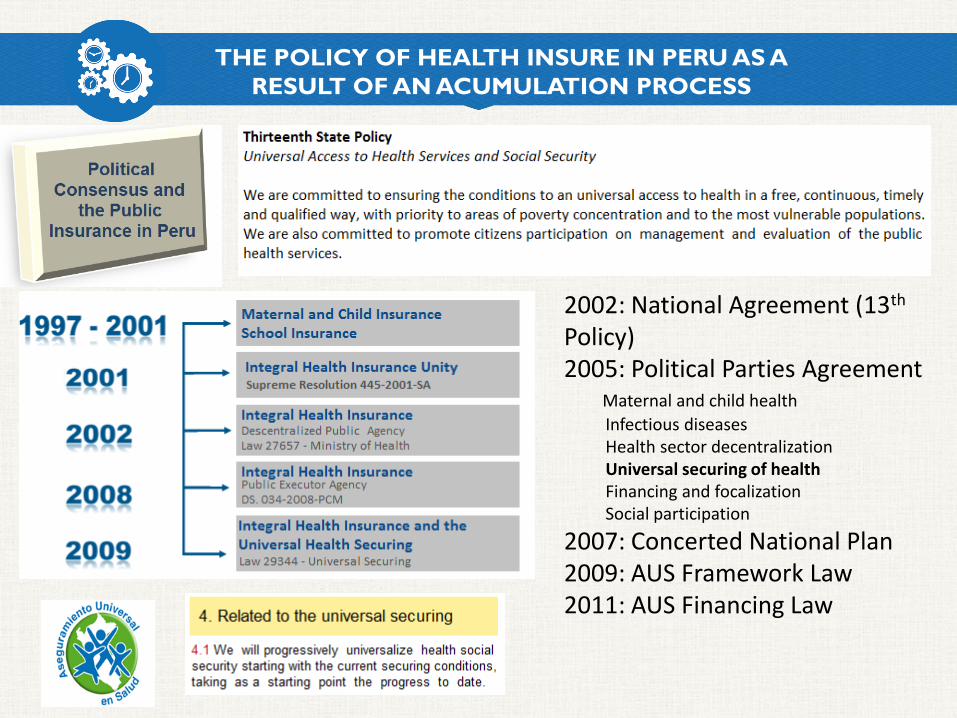
THE POLICY OF HEALTH INSURE IN PERU AS A
RESULT OF AN ACUMULATION PROCESS
2002: National Agreement (13th
Policy)2005: Political Parties Agreement
Maternal and child health
Infectious diseasesHealth sector decentralizationUniversal securing of healthFinancing and focalizationSocial participation
2007: Concerted National Plan2009: AUS Framework Law2011: AUS Financing Law

MOREprotected
people
MOREand better care
MOREproteccion of
rights
MOREstewardship and
governance of the system
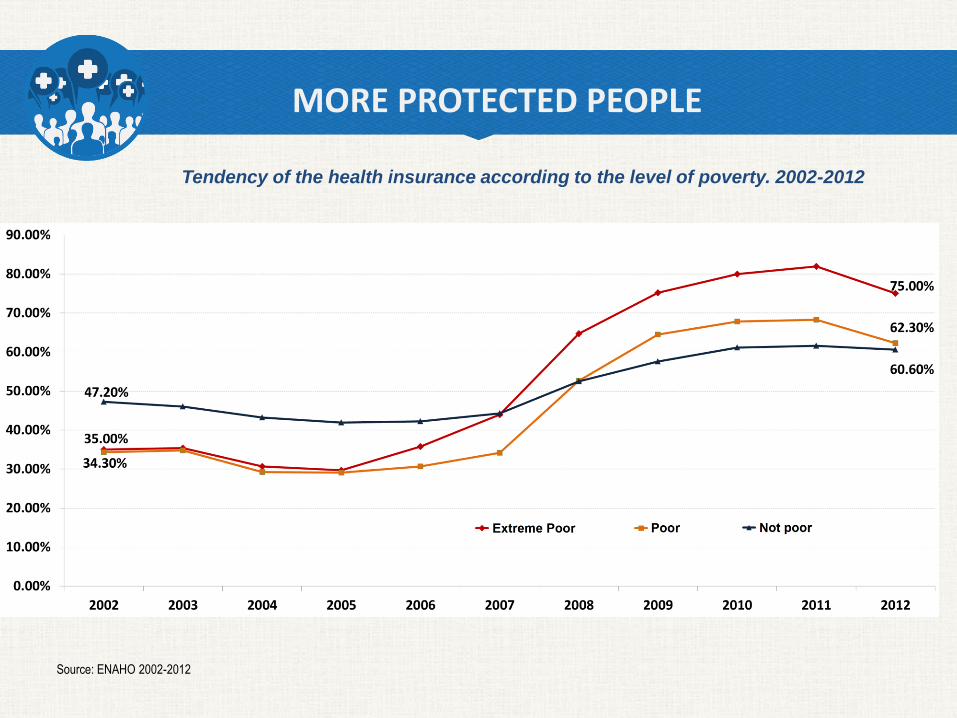
Source: ENAHO 2002-2012
Tendency of the health insurance according to the level of poverty. 2002-2012
MORE PROTECTED PEOPLE
MORE PROTECTED PEOPLE
Afiliation to SIS for poor people without coverage (inhabitants of remote areas, undocumented, residents of shelters, etc).
Afilliation to SIS for priority populations that do not have health protection: pregnant women, children from 0 to 5 years old, students of the initial and primary level in public schools.
Afilliation free of charge to the SIS for small independent contributors without health insurance.
On the path to establish a model of Social Protection in universal Health,,
we are increasing SIS insurance coverage
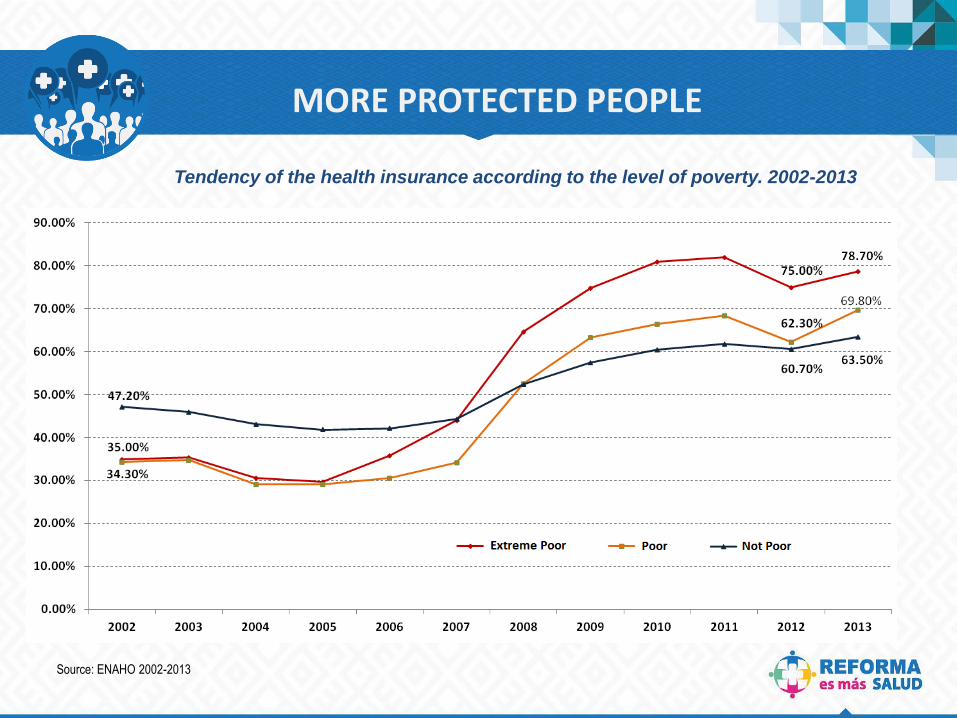
Source: ENAHO 2002-2013
Tendency of the health insurance according to the level of poverty. 2002-2013
MORE PROTECTED PEOPLE
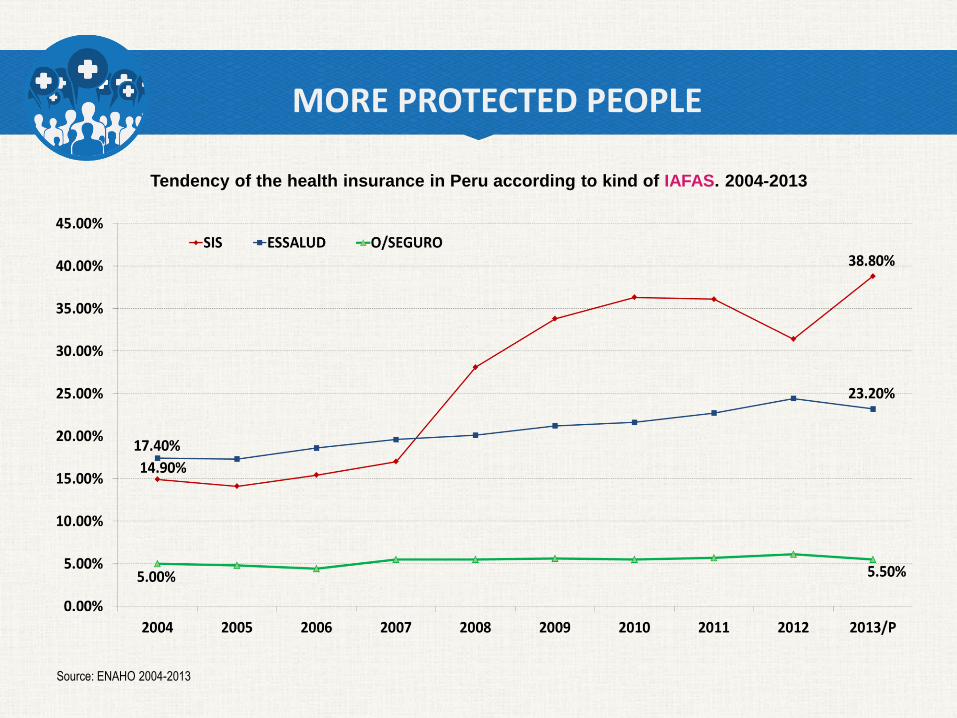
Source: ENAHO 2004-2013
Tendency of the health insurance in Peru according to kind of IAFAS. 2004-2013
MORE PROTECTED PEOPLE
MORE PROTECTED PEOPLE
MORE AND BETTER CARE
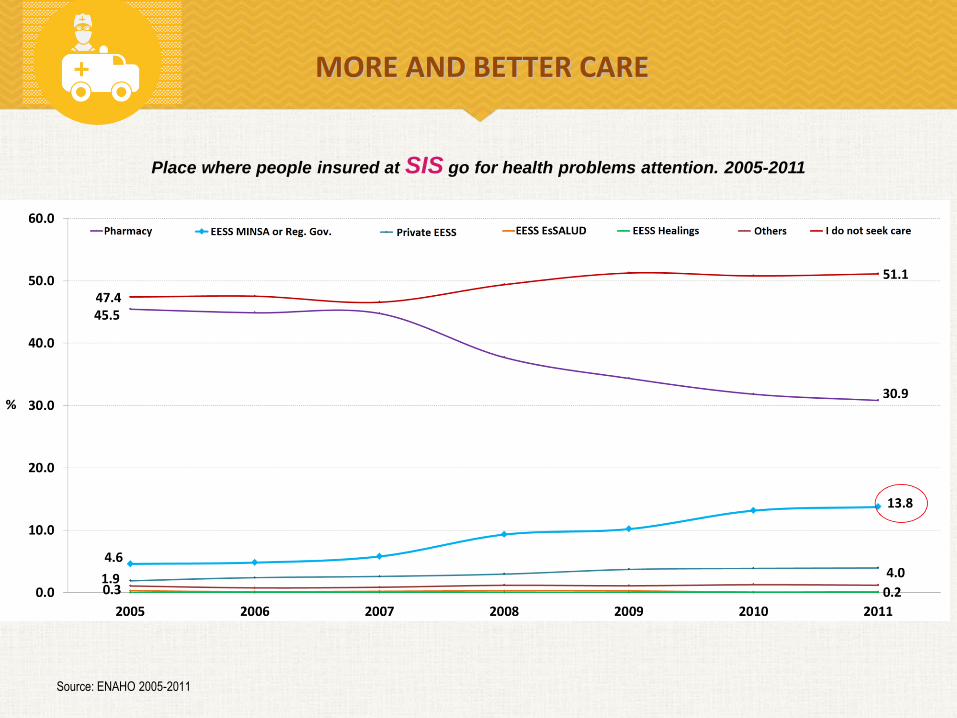
Place where people insured at SIS go for health problems attention. 2005-2011
Source: ENAHO 2005-2011
MÁS Y MEJORES CUIDADOSMORE AND BETTER CARE
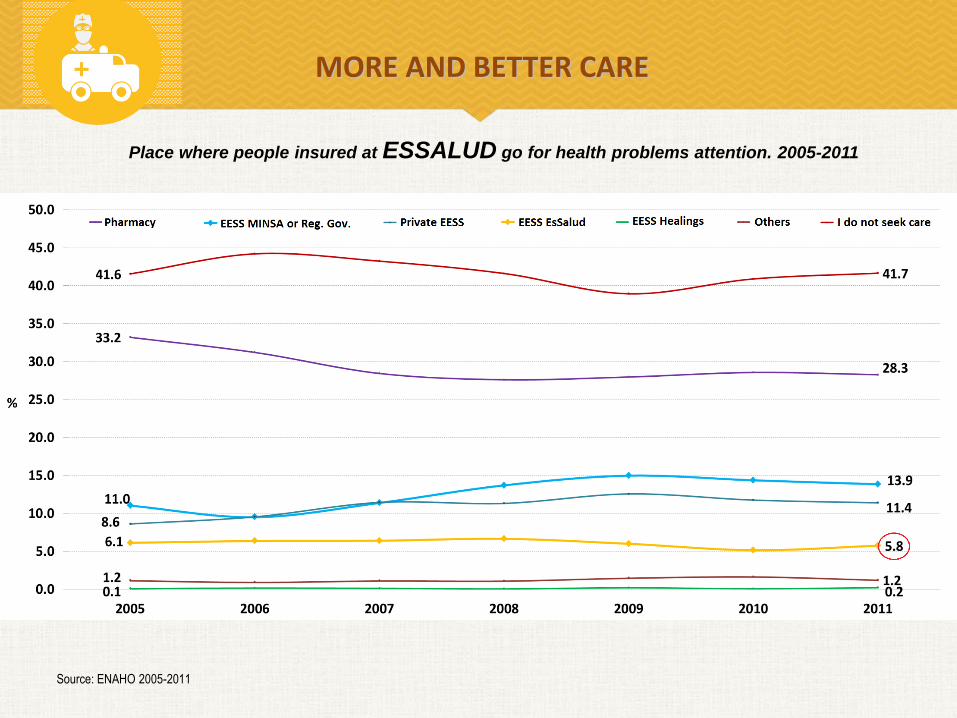
Source: ENAHO 2005-2011
MORE AND BETTER CARE
Place where people insured at ESSALUD go for health problems attention. 2005-2011

Bring closer the health interventions and
services thorugh integrated nets of primary health attention, including specialized attention
Establish a remunerative policy that encourages
the primary health attention, the specialized attention, the work in remote areas, the responsibilities of leadership and adequate performance
Expand the use of the existing public offer through exchange and the provision of complementary services
Reduce pocket spending on medication through
improvement of access to generics for people insured by SIS
Strengthen the public offer of health services,
modernizing the management of investments and complementing it with APP
MORE AND BETTER CARE
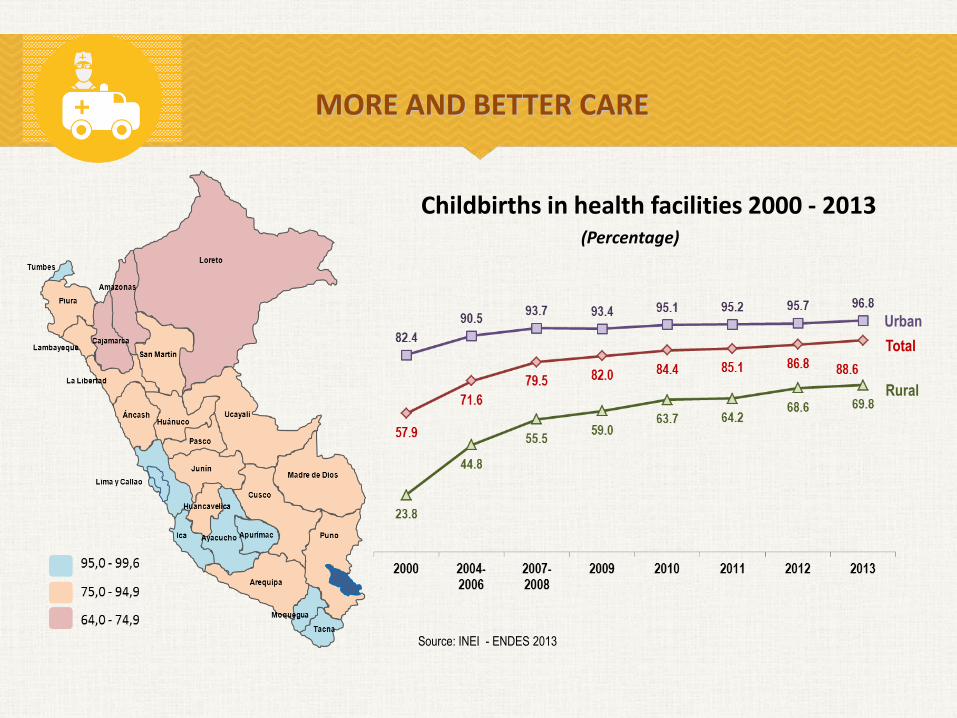
(Percentage)
Childbirths in health facilities 2000 - 2013
Urban
Total
Rural
Source: INEI - ENDES 2013
MORE AND BETTER CARE
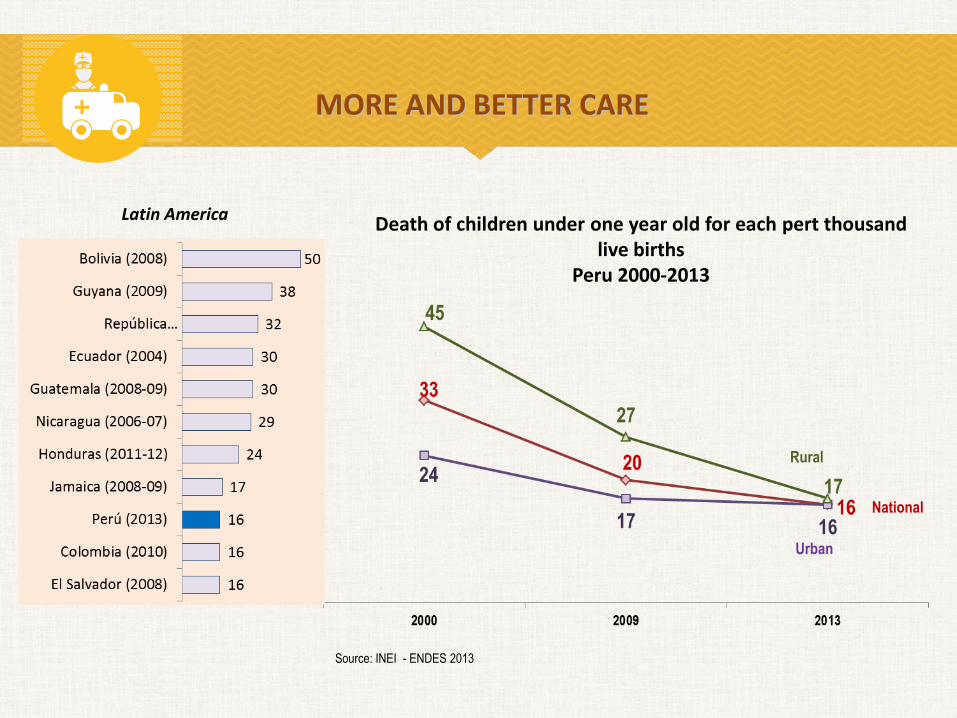
Urban
National
Rural
Latin AmericaDeath of children under one year old for each pert thousand
live birthsPeru 2000-2013
Source: INEI - ENDES 2013
MORE AND BETTER CARE

MORE PROTECTION OF RIGHTS
Gestionar el riesgo operativo de las instituciones del sistema
Orient and protect the rights of users
Propose appropriate models of providers
Monitor the adequacy of the categorization and of accreditation of providers
Monitor the compliance with standards in the provision of health services
The National Health Superintendence is the institution that, through itsactions, induces to aggregate value to the operations of the health systemin benefit of users

MORE STEWARDSHIP AND GOVERNANCE OF THE SYSTEM
Reorganize the ministry with emphasis in public health and multisectorial actions about the social determinants of health
Strengthen the intergovernmental articulation on health
Strengthen the capacity of Regulation and Fiscalization of the health related markets
Develop the Sectorial System of Health Information connected to the system of monitoring and evaluation of the objetives and goals of health and reform
Guarantee the public service in emergency situations
To make possible and sustainable the measures designed for the people
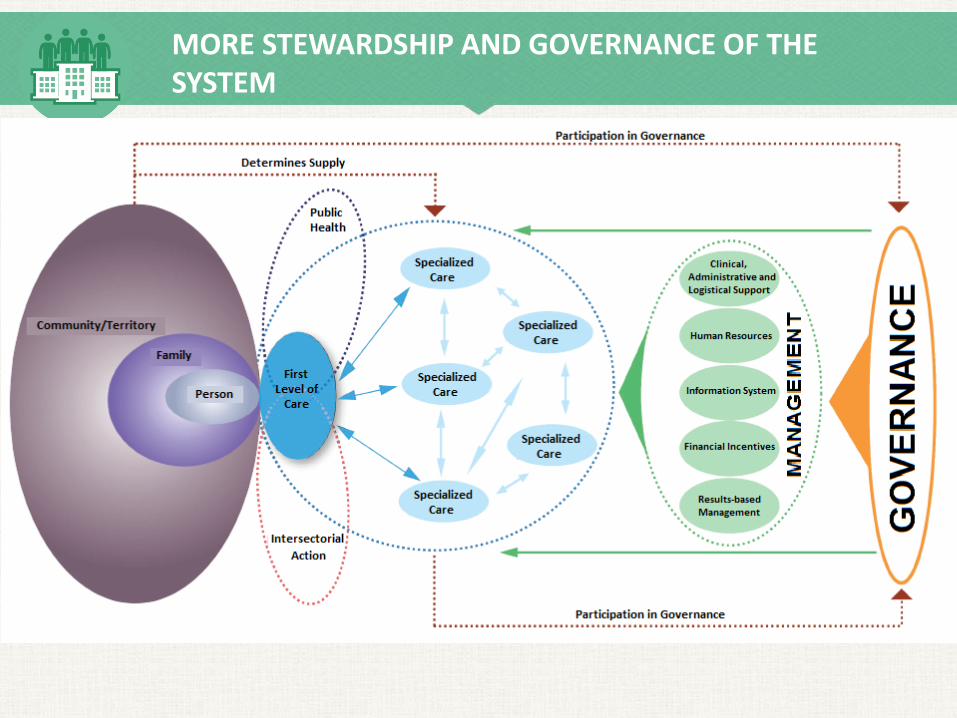
MORE STEWARDSHIP AND GOVERNANCE OF THE SYSTEM

MORE STEWARDSHIP AND GOVERNANCE OF THE SYSTEM
Of Coordination: Para generar acuerdos intergubernamentales.
Of Colaboration: Bilateral and reciprocal support.
Of Cooperation: In the framework of the respective competences.
In search of eficacy, quality and good orientation of Stateintervention
Mechanisms for the Process
• Management Agreements (Convenios de Gestión) with the Regional Governments for compliance with institutional goals, performance indicators and improvements in services, under the DL N°1153.
• Convenios entre el SIS y los Gobiernos Regionales para pago “capitado” que estimule las actividades de prevención y la mejora de los indicadores sanitarios.

MORE STEWARDSHIP AND GOVERNANCE OF THE SYSTEMMultisectoral and Intergovernmental Alliances
Lima Respira Vida Juntos against TuberculosisSeptember 11th, 2011
Agreement MINSA – ESSALUD – Regional GovernmentsPerformance Exchange
Plan Integral Peste – Macro Norte Region
egional La LibertadRepresentants OPS/OMS
Provincial Mayors
Plan TB Cero
Eco. Victor Salcedo R.Mayor El Agustino
Arq. Alberto Sánchez A.Mayor La Victoria
Coronel® Marco ÁlvarezAlcalde San Borja
Dra. Carmen MasíasPresidenta DEVIDA
Preventorium for children a and adolescents






























