Embed Size (px)
Citation preview
Risk Reduction through Family Therapy (RRFT): An Integrative Approach to Treating Substance Use Problems and PTSD Among Maltreated Youth
Carla Kmett Danielson, Ph.D.
Medical University of South Carolina
April 13, 2015
Objectives• 1) Understand the relation between high-risk
behaviors and child victimization
• 2) Become familiar with the clinical and empirical rationale for taking an integrated and risk reduction approach to treatment with maltreated adolescent populations
• 3) Learn the fundamental components in administering RRFT
Relation Between High-Risk Behaviors and
Child Victimization
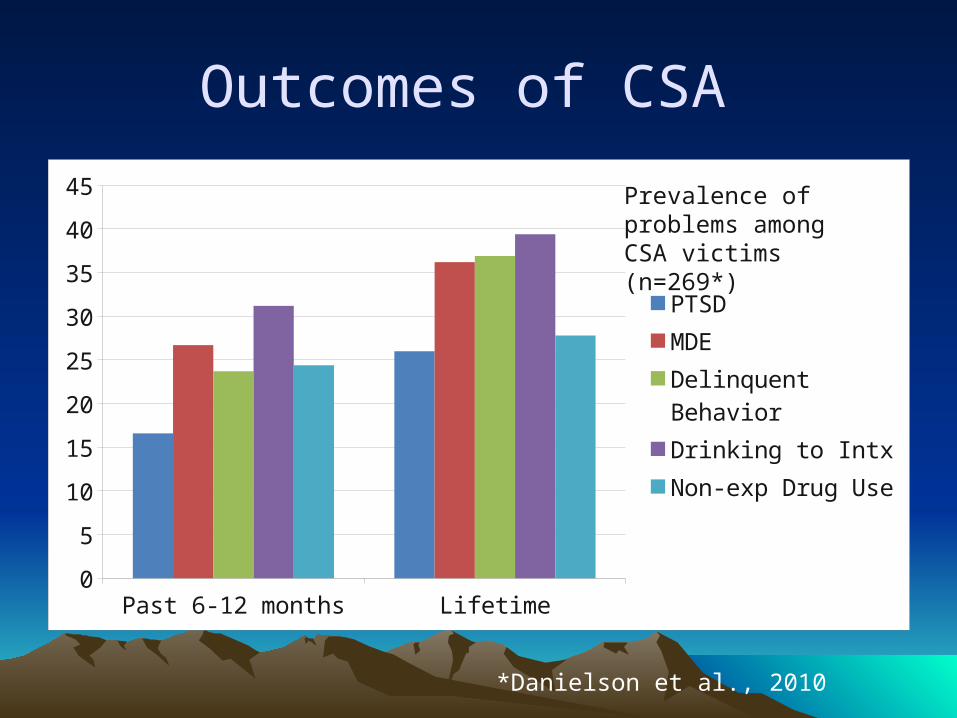
Outcomes of CSA
Past 6-12 months Lifetime0
5
10
15
20
25
30
35
40
45
PTSDMDEDelinquent BehaviorDrinking to IntxNon-exp Drug Use
*Danielson et al., 2010
Prevalence of problems among CSA victims (n=269*)
Trauma and Substance Abuse
• CSA: Over 2 times more likely to develop alcohol or hard drug abuse
• CPA: Over 1.5 times more likely to develop alcohol or marijuana abuse; over 3 times more likely to develop hard drug abuse
• WV: Over 2.5 times more likely to report alcohol abuse and over 4 times more likely to report marijuana or hard drug abuse
• PTSD: Over 2 times more likely to report marijuana or hard drug abuse
CSA and Risky Sexual Bx
• Among adolescent girls: – CSA significantly increased the odds of experiencing
an adolescent pregnancy by 2.21-fold (up to 13 times more likely);
– 2. 5 times more likely to have 3 or more partners;
• Among adolescent boys:– Sexually abused boys were significantly more likely
than nonabused boys to report unprotected intercourse (1.91), multiple sexual partners (2.91), and pregnancy involvement (4.81).

Rationale for an Integrated Approach to Treatment
What drives risky behavior among trauma-exposed teens?
What drives risky behavior among trauma-exposed teens?
Being an adolescent (Neurology)
Coping skills Other traumatic
event exposure
Allstate Ad, 2007
WHY?
• Traumatic Event Exposure?– Reenactment– Coping– G X E
Link between trauma and substance abuse: Negative Reinforcement Model
• Negative reinforcement models– “Self-Medication Hypothesis”
– The motivational basis of behavior is the reduction or avoidance of aversive internal states.
Link between trauma and substance abuse: Negative Reinforcement Model
Example: Substance Abuse is Increased by Removing Aversive Affect
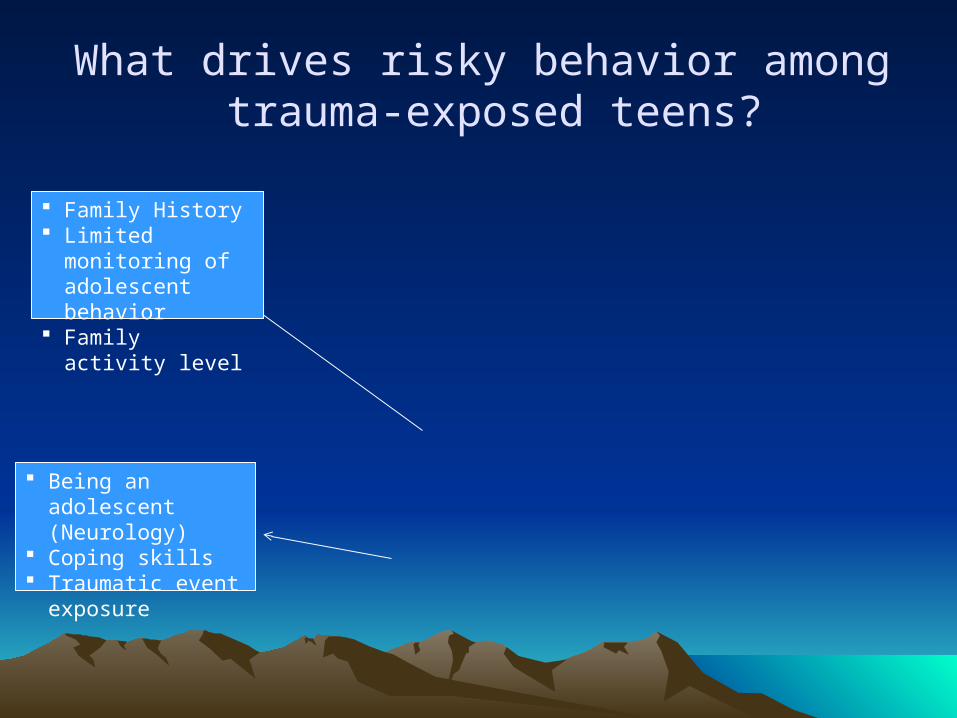
What drives risky behavior among trauma-exposed teens?
Family History Limited monitoring
of adolescent behavior
Family activity level
Being an adolescent (Neurology)
Coping skills Traumatic event
exposure
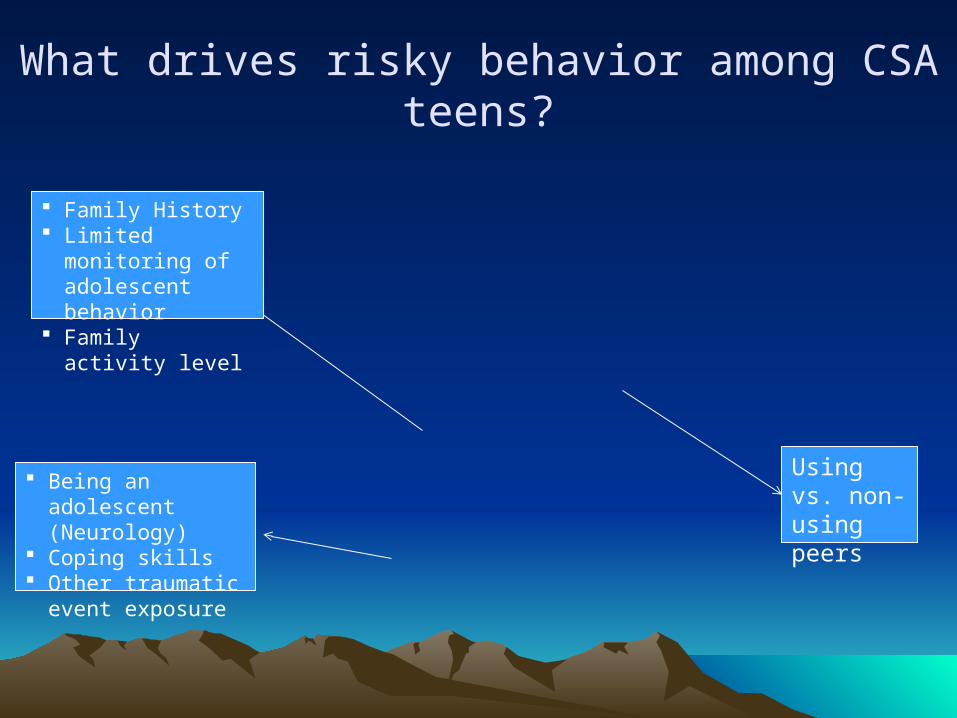
What drives risky behavior among CSA teens?
Using vs. non-using peers
Family History Limited monitoring
of adolescent behavior
Family activity level
Being an adolescent (Neurology)
Coping skills Other traumatic
event exposure
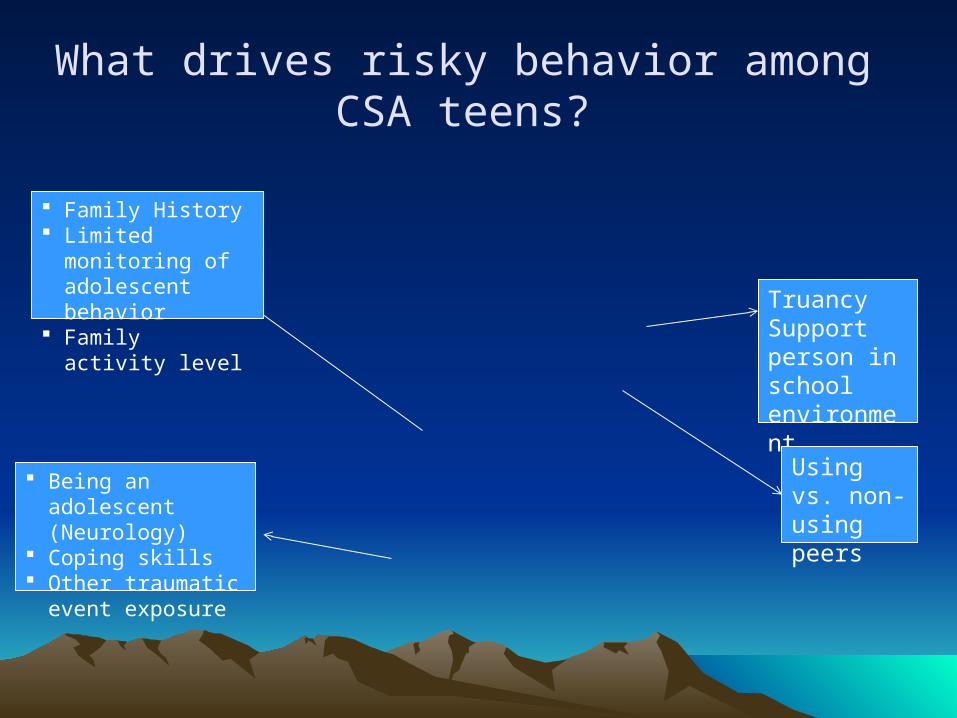
What drives risky behavior among CSA teens?
TruancySupport person in school environment
Using vs. non-using peers
Family History Limited monitoring
of adolescent behavior
Family activity level
Being an adolescent (Neurology)
Coping skills Other traumatic
event exposure
What drives risky behavior among CSA teens?
Drug communityActivities in the community
TruancySupport person in school environment
Using vs. non-using peers
Family History Limited monitoring
of adolescent behavior
Family activity level
Being an adolescent (Neurology)
Coping skills Other traumatic
event exposure
Risk Factors: Community
• Drug community? • Rural?• Structured activities?
State of the Science for Integrated Approaches for Adolescents
• Progress in Adult Trauma/Substance Abuse Field– Some data that integrated approaches are safe (exposure),
efficacious, and preferred by consumer (Back et al., 2006; Brady et al., 2001; Cocozza et al., 2005; Mills et al., 2012)
• Seeking Safety (Najavits, Gallop, & Weiss, 2006)
– 1 Pilot RCT (n=33; vs. TAU)– No treatment effects for PTSD
• No Exposure
State of the Science for Integrated Approaches for Adolescents
• Three RRFT studies to date– Completed open pilot trial (N=10) (Danielson et al., 2010b )– Completed pilot RCT vs. Usual Care (N=30) (Danielson et
al., 2012)– CSA; 70% reported other types of traumatic events– Assessments:
• Interviews, urine drug screens, parent-report, youth-report, chart
• Pre, Post, 3-month and 6-month follow-ups
– Ongoing RCT vs. TAU (n=80 to date)• Through 18 month follow-up

RRFT Overview
Identifying RRFT Clients
• ‘Who’ is an RRFT case?
RRFT Overview
• Clinical Pathways Approach– Use assessment to guide clinical decisions regarding
risk reduction vs. intensive treatment and order
• Seven primary OVERLAPPING components:– Psychoeducation & Engagement– Family Communication– Substance Abuse– Coping Skills– PTSD– Healthy Dating and Sexual Decision Making– Revictimization Risk Reduction
RRFT Overview
• Principle 1: Finding the Fit• Principle 2: Positive and Strength
Focused• Principle 3: Increasing
Responsibility• Principle 4: Present-Focused,
Action-Oriented and Well-Defined• Principle 5: Targeting Sequences• Principle 6: Developmentally
Appropriate• Principle 7: Continuous Effort• Principle 8: Evaluation and
Accountability• Principle 9: Generalization
• P sychoeducation and parenting skills
• R elaxation• A ffective expression and
regulation• C ognitive coping • T rauma narrative development
& processing• I n vivo gradual exposure• C onjoint parent child sessions• E nhancing safety and future
development
RRFT Fundamentals
• Confident• Authentic• Put it to paper• Tangible progress• Agenda• Integrity • Novelty
RRFT Fundamentals
• Confident
RRFT Fundamentals
• Authentic
• “What made the difference?”• Hearing what is important to the teen, the
caregiver, the family….
RRFT Fundamentals
• Put it to paper• What should get written down?
RRFT Fundamentals
• Tangible progress• What is the value of this?• How does efficacy get built?• Real example
RRFT Fundamentals
• Agenda• What does this mean?• What is the value of this?
RRFT Fundamentals
• Integrity • Ecologically valid sessions• Ways to do this?
RRFT Fundamentals
• Novelty• Always change things up
RRFT Format
• Individual and Family Sessions• Office or community• Phone Check Ins are critical• Homework
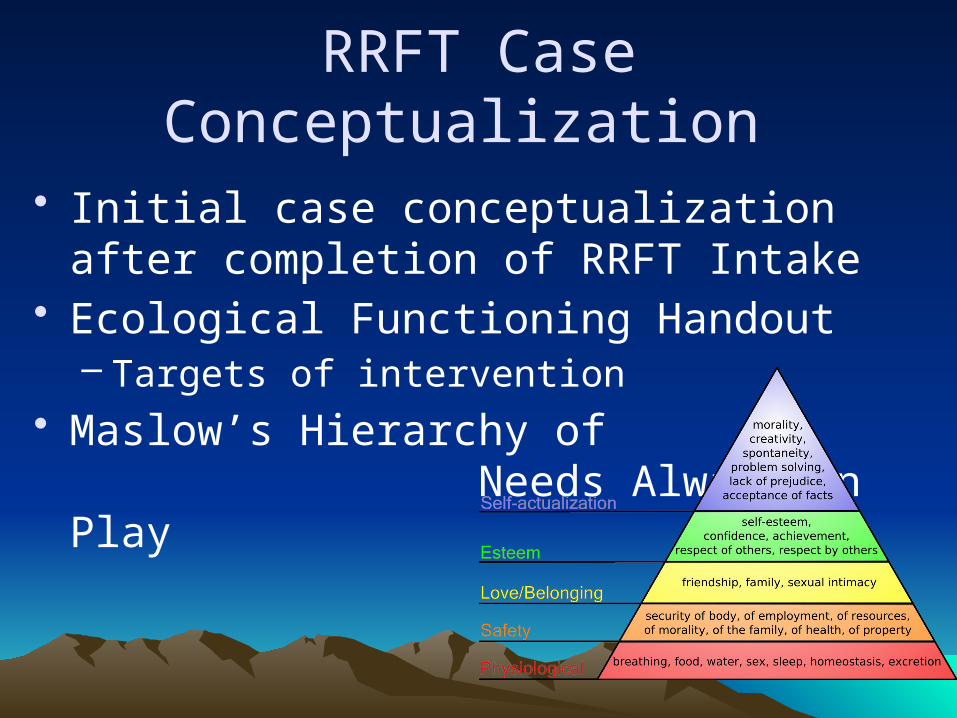
RRFT Case Conceptualization
• Initial case conceptualization after completion of RRFT Intake
• Ecological Functioning Handout– Targets of intervention
• Maslow’s Hierarchy of Needs Always in Play
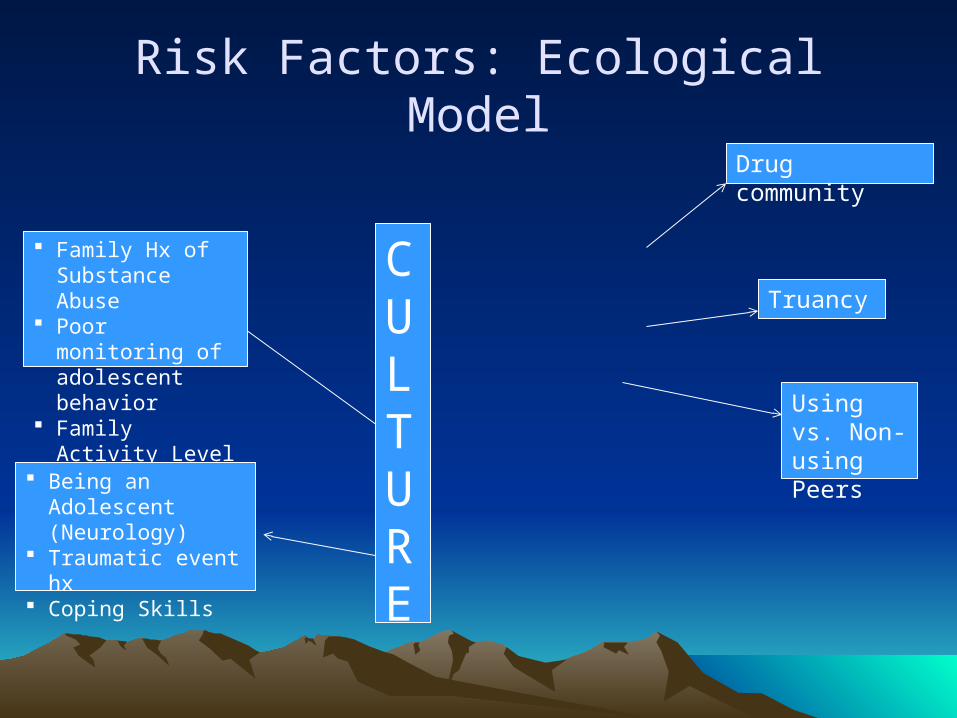
Risk Factors: Ecological Model
Drug community
Truancy
Using vs. Non-using Peers
Family Hx of Substance Abuse
Poor monitoring of adolescent behavior
Family Activity Level
Being an Adolescent (Neurology)
Traumatic event hx Coping Skills
CULTURE
Psychoeducation & Engagement (P & E)
Goals of P & E Provide information about traumatic events as relevant Provide information about psychological and physiological
reactions to stress Normalize teen’s and caregiver’s reactions to severe stress Emphasis on substance use and other risk behavior
Instill hope for teen and family recovery Engage and Educate family about the benefits and need
for sticking with treatment Barrier assessment Safety planning
SET TREATMENT GOALS!!! ( ‘carrot’) Enhance motivation for cutting down on substance use and
reducing other risky behavior as relevant Youth and caregiver

Family Communication
Goals of Family Communication
• Improve healthy communication between teen and caregivers
• Increase family cohesion• Decrease family conflict• Increase parenting skills to manage high risk
behaviors– Build caregiver’s efficacy via successful experiences
• Establish caregiver as the person the teen turns to for help in times of trouble
• For youth without a participating caregiver: – Identify other champions for the youth – Process thoughts and feelings about not having participating
caregiver
SUBSTANCE ABUSE
Goals of Substance Abuse
• To reduce substance use • To enhance motivation and efficacy in reducing use• To identify drivers of substance use problems and implement
evidence-based interventions to address the drivers– To help teen better understand link between their trauma history
and their substance abuse• To bolster protective factors against substance abuse• To teach realistic refusal skills• To replace needs met by substance use with more adaptive
strategies– Activating the reward system in other ways!
• To monitor use with random screening (ideally by caregiver)• To monitor use in the context of trauma treatment
– Weekly assessments
• Disclosure to caregiver right away when possible
• Harm reduction right away when possible
• Drug/breath screening right away when possible, even when youth is denying use
• Ecological Validity (create the ‘mood’)
Substance Abuse: Emphasized Key Components
Substance Abuse
• Fit Circle• Substance abuse goes in the middle• What are behaviorally specific drivers?
– Some common drivers:– Poor monitoring– Negative peers– Lack of positive activities– Low social support of family– Truancy
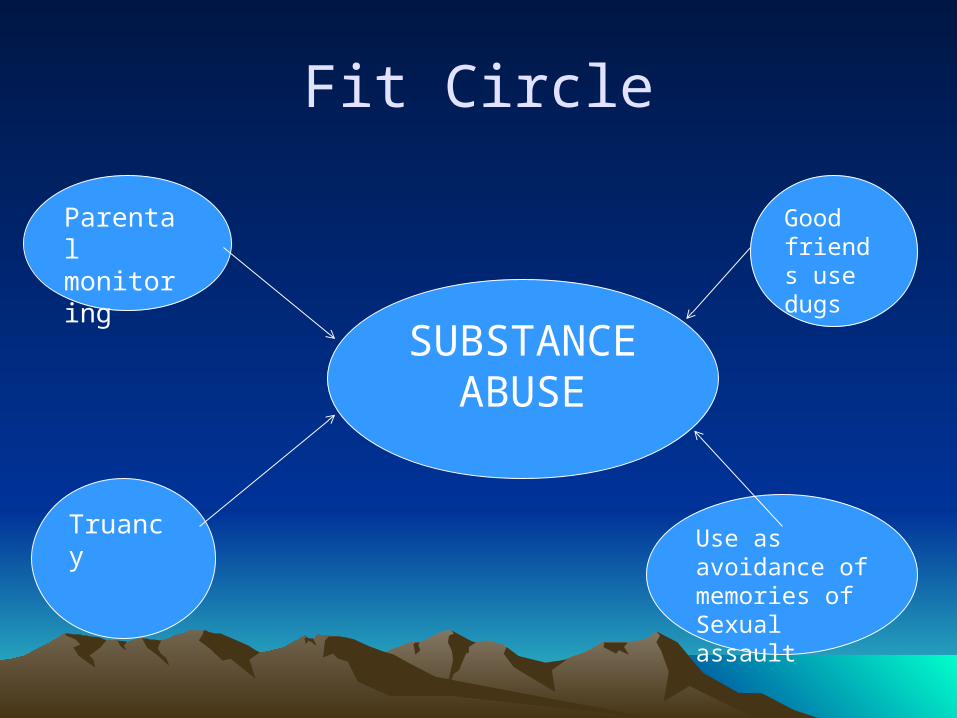
Fit Circle
SUBSTANCE ABUSE
Good friends use dugs
Use as avoidance of memories of Sexual assault
Truancy
Parentalmonitoring
Substance Abuse
• Include teen and caregiver in this process (in session)
• Begin by choosing one or two primary “drivers”• Then do a fit circle around each one of these to
determine your interventions– Strength-focused – Target sequence of events– Behaviorally specific
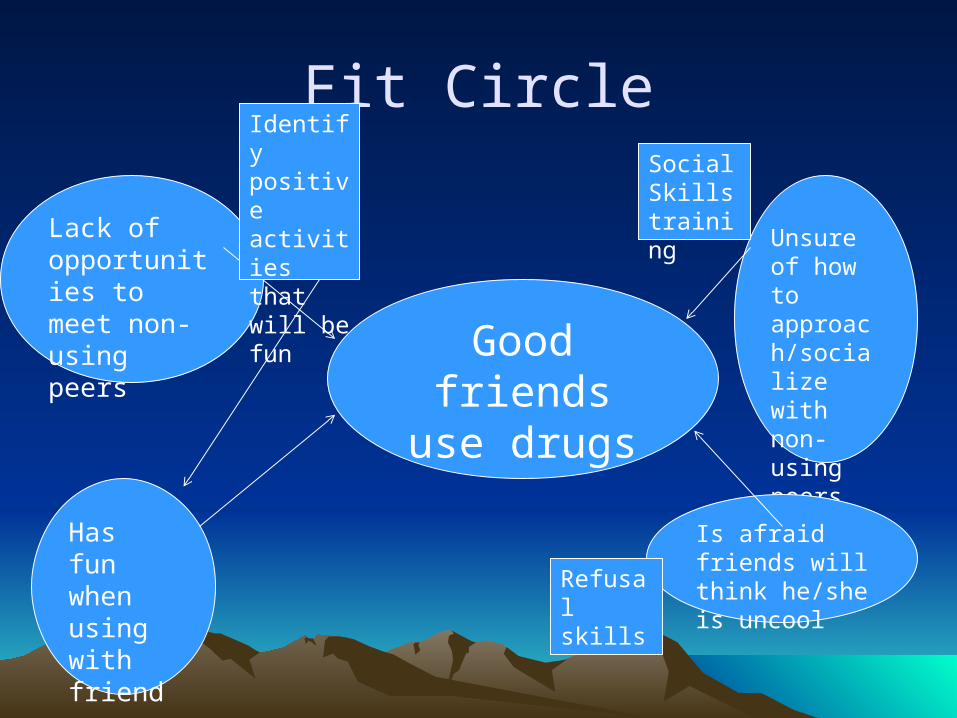
Fit Circle
Good friends use drugs
Unsure of how to approach/socialize with non-using peers
Is afraid friends will think he/she is uncool
Has fun when using with friends
Lack of opportunities to meet non-using peers
Social Skills training
Refusal skills
Identify positive activities that will be fun
Fit Circle Role Play
Drug Testing Protocol Objective:
1. Provide a reliable and valid measure of substance use so that contingencies can be applied appropriately and quickly.
Drug screening is key!• Teaching caregivers• Therapist testing in absence of caregiver• What to do with alcohol, less urine screen-able
drugs
• “7 C’s of Leverage” (Dr. Wes Boyd)1.Cash
2.Computer
3.Curfew
4.Cell phone
5.Car
6.Credit
7. Cards
Substance Use: Contingency Management
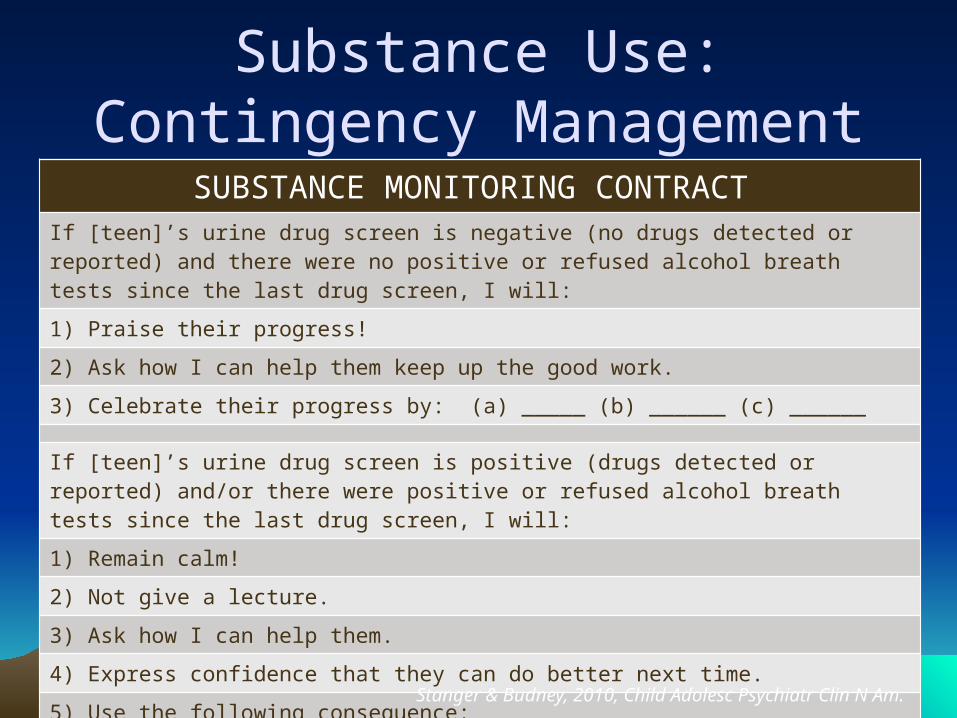
SUBSTANCE MONITORING CONTRACT If [teen]’s urine drug screen is negative (no drugs detected or reported) and there were no positive or refused alcohol breath tests since the last drug screen, I will:
1) Praise their progress!
2) Ask how I can help them keep up the good work.
3) Celebrate their progress by: (a) _____ (b) ______ (c) ______
If [teen]’s urine drug screen is positive (drugs detected or reported) and/or there were positive or refused alcohol breath tests since the last drug screen, I will:
1) Remain calm!
2) Not give a lecture.
3) Ask how I can help them.
4) Express confidence that they can do better next time.
5) Use the following consequence: __________
Parent signature _______ Date _______ Teen signature _______ Date ______
Substance Use:Contingency Management
Stanger & Budney, 2010, Child Adolesc Psychiatr Clin N Am.
Substance Abuse
• Progress is progress (harm reduction)
COPING
Goals of Coping Component• Understand concept of positive and negative coping• Feelings identification and expression
– Feeling safe– SUDS scale
• To be able to differentiate and understand the link between thoughts, feelings, and behaviors
• Increase positive coping techniques – Relaxation– Guided Imagery and PMR– Cognitive processing
• To increase distress tolerance skills– Mindfulness
PTSD
Goals of PTSD Component
• Psychoeducation-PTSD symptoms• More intensive trauma exposure work (memories,
emotions, cues): Trauma Narrative and In Vivo• Identification of Inaccurate or Unhelpful Core
– Beliefs that have been developed or reinforced as a function of trauma exposure
• Processing of such beliefs to become more helpful and/or accurate
• “Make Meaning”
Healthy Dating & Sexual Decision Making
Healthy Dating & Sexual Decision Making: Goals
• Redefine meaning of sex, intimacy• Differentiate healthy vs unhealthy romantic relationships
– Healthy relationship with self
• Discuss factors in making decisions related to dating and intimacy and how current decision making either coincides or flies in the face of client’s goals
• Provide psychoeducation related to sexuality (STDs, pregnancy)
• Develop skills for consistent and proper condom use• When feasible and appropriate, establish caregiver as the
person the client will speak with in future regarding dating and sex.
Revictimization Risk Reduction
Revictimization Risk Reduction: Goals
• Primary goal of this component is enhancement of safety– Listening to ‘inner voice’: Recognizing cues, signs, etc
for potentially unsafe people, places, and situations– For CSEC or gang, will be to reduce risk of their being
sexually exploited again, or going back to the streets.
• Other goals include: – Reduce risk of other forms of victimization (e.g., on-
line, witnessing community violence)– Relapse prevention of symptoms that have improved
Considerations for Child Welfare
• How do these youth get identified?• How do they get labeled?• What types of referrals are (or can be)
made?