Embed Size (px)
Citation preview
AETNA MEDICAID
Scott BrunnerOctober 28, 2016
Medicaid Managed Care and the Final Rule
Agenda
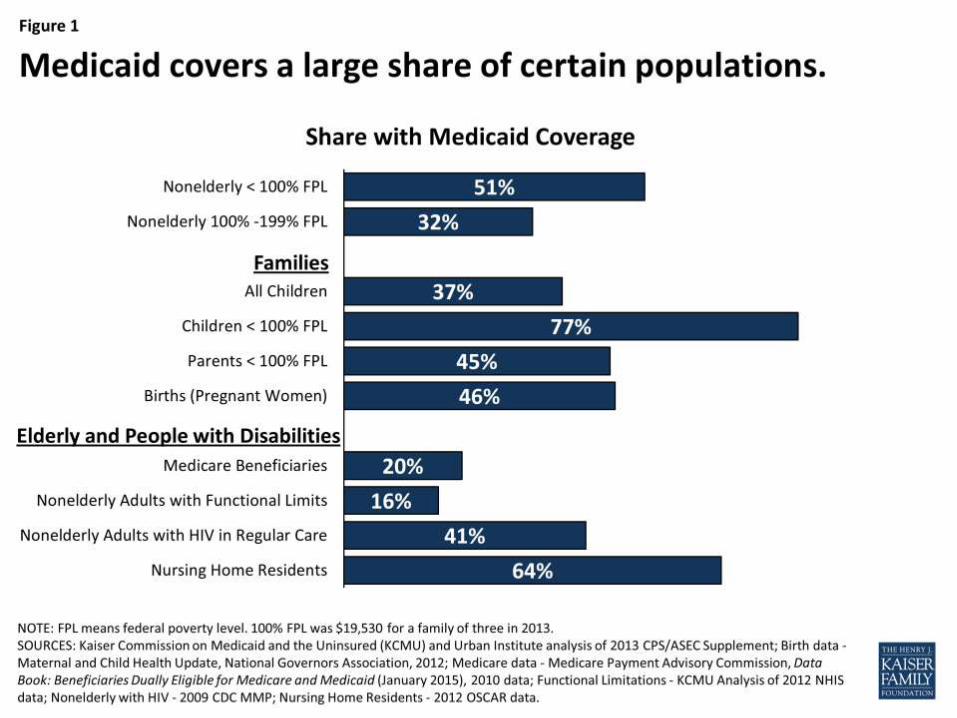
Growth of Medicaid in the health care system
Growth of Managed Care within Medicaid
Aetna’ Footprint in Medicaid Managed Care
Implications of the Medicaid Managed Care Final Rule (Mega Rule)
2
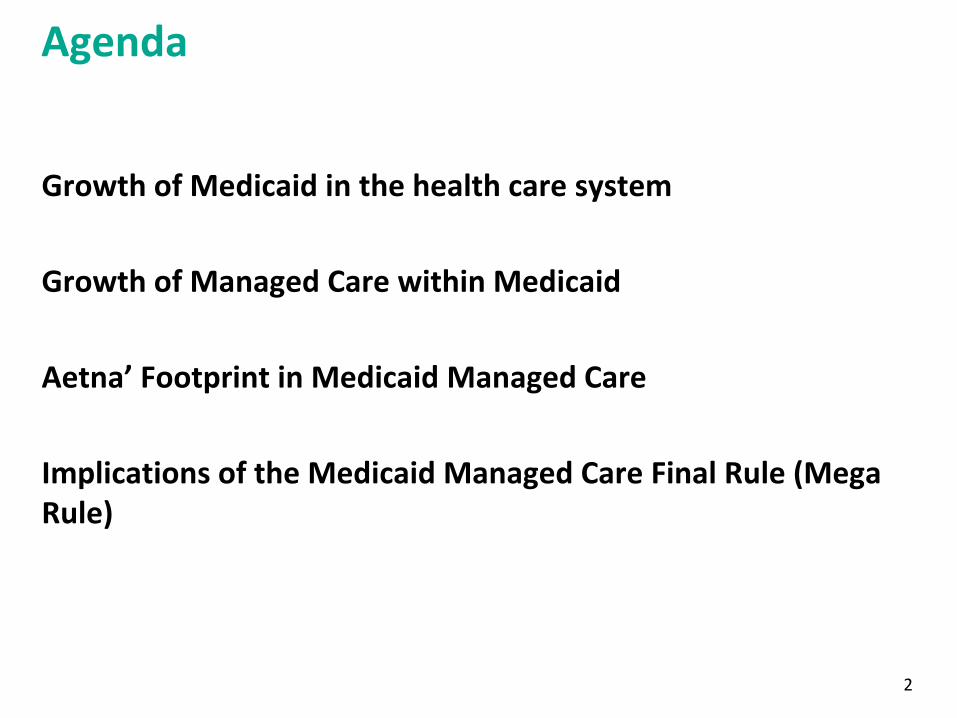
$5 $13 $26 $41 $74$145 $203 $317 $409 $563 $742 $999
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1970 1975 1980 1985 1990 1995 2000 2005 2010 2015 2020 2025
Historical and Projected National Health Expenditures by Payer
FY1970–2025
Medicaid and CHIP Medicare Private insurance
Other health insurance Other third party payers Out of pocket
Source: MACPAC 2016 analysis of Office of the Actuary (OACT), Centers for Medicare & Medicaid Services 2015 National health expenditures by type of service and source of funds: Calendar years 1960–2014
Medicaid 101, May 2016
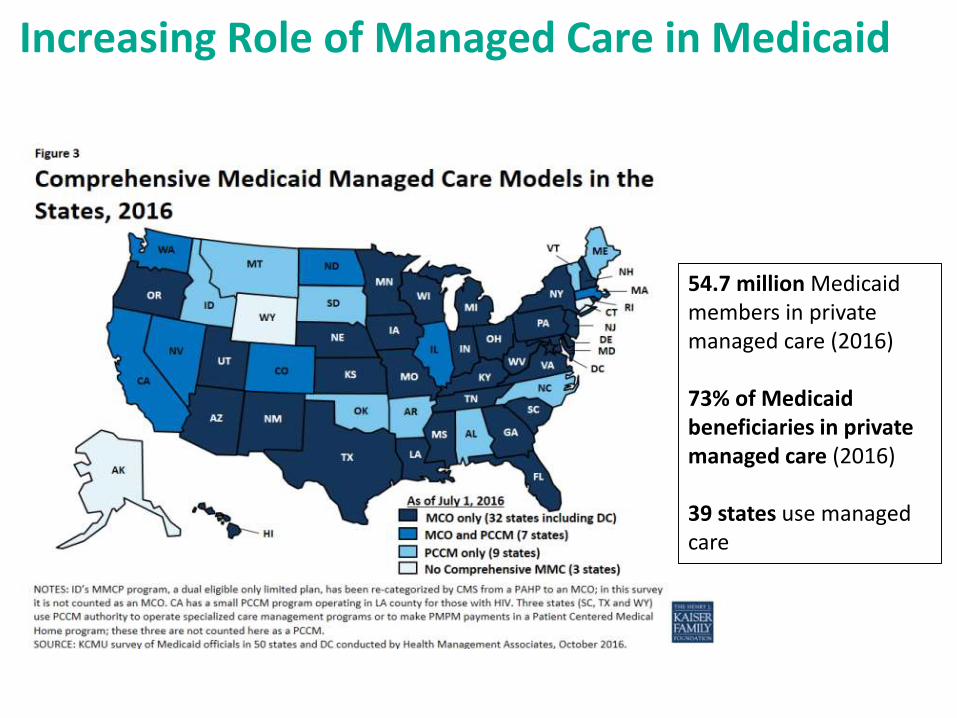
Increasing Role of Managed Care in Medicaid
54.7 million Medicaid members in private managed care (2016)
73% of Medicaid beneficiaries in private managed care (2016)
39 states use managed care
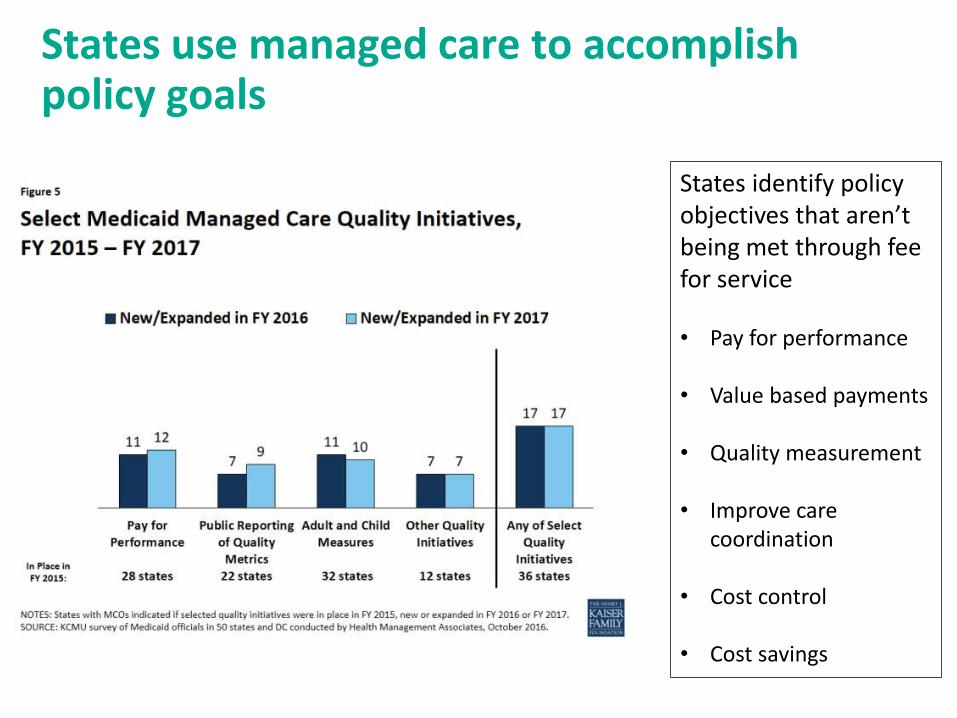
States identify policy objectives that aren’t being met through fee for service
• Pay for performance
• Value based payments
• Quality measurement
• Improve care coordination
• Cost control
• Cost savings
States use managed care to accomplish policy goals
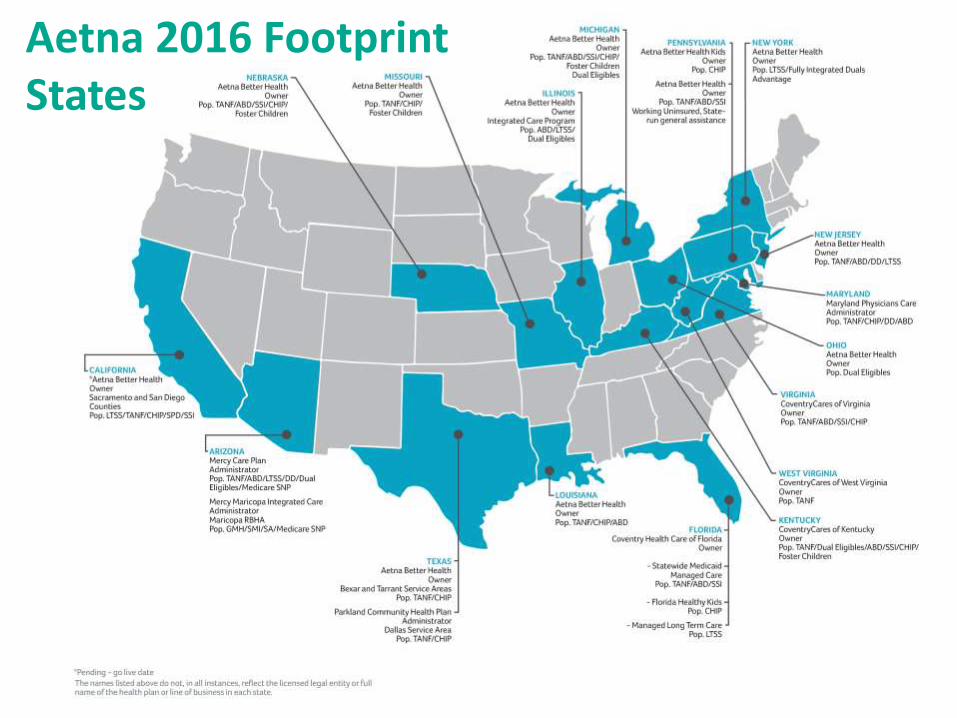
Aetna 2016 Footprint States
Key Provisions of the “Mega Rule” impacting managed care
Actuarial Soundness
Pass through payments
Network Adequacy
Provider Screening and Enrollment
Information for Enrollees
8
Goals of the CMS Managed Care Final Rule
Modernize CMS rules to fit current Medicaid Managed Care practice. • Consistency among state Medicaid managed care approaches
• Use Medicaid managed care to drive delivery system reforms and quality improvement throughout the healthcare system
• Align CMS standards for Medicaid managed care with Medicare Advantage and Marketplace plan requirements
• Make CMS oversight standards more consistent across states
9
Standardized State Flexibility
• Medical Loss Ratio and rate setting• Appeals and grievances policies and
timelines• Provider enrollment shifted to the
state level• Encounter data and annual reports
• Network adequacy metrics and definitions
• IMD and “in-lieu of” options• Delivery system and payment
reforms• State managed care quality strategy
Actuarial Soundness
Soundness requirements• Any difference in rates cells or population must be due to risk based rating
factors and not requirements to pay providers higher rates.
• Each rate cell must have a specific rate. No rate ranges are allowed
• States can increase or decrease the certified capitation rate by 1.5% without submitting a revised rate certification for CMS’ approval.
• Rate cells cannot be used to cross subsidize another rate cell.
• Rate trend factors must be developed from actual experience or a real member population.
• Any incentive payments in MCO contracts cannot exceed 105% of the capitation rate.
• Any hold backs in MCO contracts cannot exceed 5% of the capitation rate
10
Pass Through PaymentsPass-through payments are supplemental payments states direct managed care plans to provide to specific providers; not directly linked to services under the contract or outcomes
CMS has longstanding concerns with pass-through payments, including their potential to limit plans’ ability to effectively implement value-based purchasing
Final rule phases out states’ ability to use pass-through payments
Hospitals provided with ten year transition (until 7/1/27)
Physicians and nursing facilities provided with a 5-year transition (until July, 1 2022)
Exception for FQHC wrap-around payments required by law and graduate medical education (GME) payments
11
Network Adequacy
States must develop and implement time and distance standards for services covered including:• Primary and specialty care (adult and pediatric)
• Behavioral health (adult and pediatric)
• OB/GYN
• pediatric dental
• Hospital
• Pharmacy
Must have standards for Medicaid managed long term services and supports programs for providers who travel to the enrollee to provide services;
Assess and certify the adequacy of MCO provider network at least annually and when there is a substantial change to the program design (such as adding a new population, benefits, or service area).
12
42 CFR 438.332, .340; Effective: Rating periods for contracts starting on or after 7/1/18
Provider Screening and Enrollment
All Medicaid providers – Fee for Service and Managed Care –must be enrolled with the state
States are responsible for screening and enrollment may delegate to third parties such as plans or fiscal intermediaries.
MCO network providers are not obligated to deliver services to FFS beneficiaries
Plans may execute a provider agreement for up to 120 days pending the outcome of the screening process
Rules apply to CHIP
13
New Provider Directory RequirementsAdditional information:
Provider’s group affiliationWebsite address Cultural and linguistic capabilities Whether the provider’s facility is accessible for people with physical disabilities
MCOs must update within 30 calendar days of receipt of changed provider information.
Timeframes align with QHP and Medicare Advantage
New Member Handbook Requirements• Provided in “prevalent” non-English languages• Include auxiliary aids for deaf and blind individuals • May be offered electronically on plan website and hard copy within 5
business days, without charge• Instructions on how to obtain services from out-of-network providers
Information for Enrollees
14
Conclusions about the Mega Rule
Managed care is the dominant delivery system for Medicaid.
The Mega Rule modernizes governing practices, aligns with Medicare Advantage and Marketplace, makes oversight more consistent.
The rule impacts almost all areas of Medicaid operations—both state programs and MCOs. That has a direct impact on providers serving Medicaid members.
How much variation will happen state to state? What impact will the next administration have?
15