Embed Size (px)
Citation preview
Experiences in Scaling Supply Chain Interventions for iCCM Supply Chain Management Subgroup
of the iCCM Task Force
Tuesday 14 April 2015 CORE Group Spring 2015 Global Health
Practitioner Conference
Pilot and scaling cStock and DPATs in Malawi
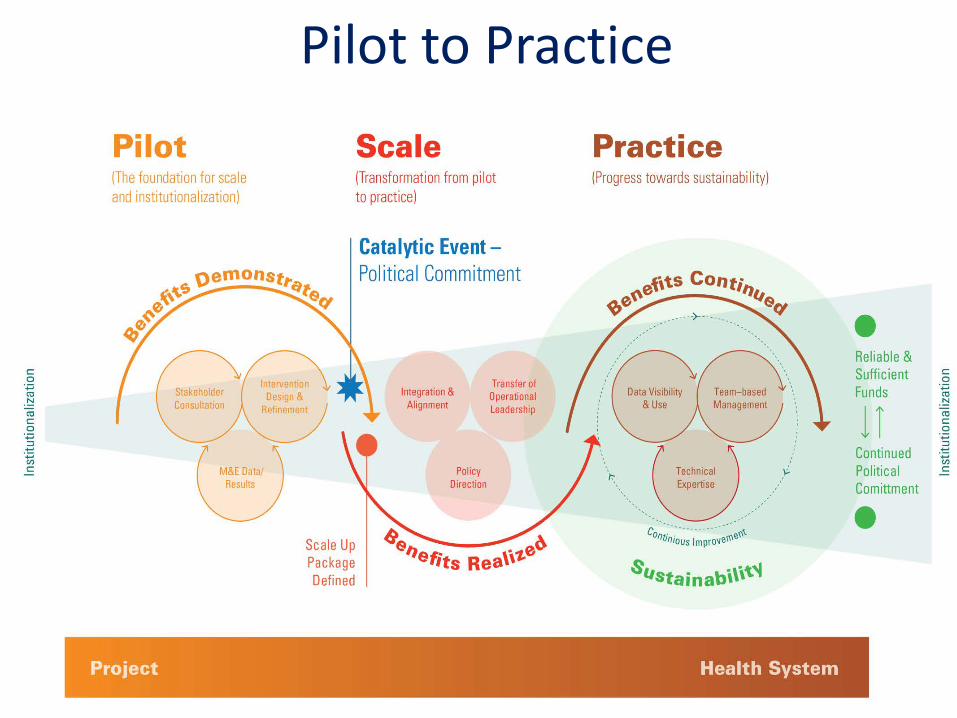
Pilot to Practice
Intervention Design and Refinement
• Kept the design simple and suitable for the context
• Considered sustainability - scalability, institutionalization and integration – from the design phase
• Used a systems approach: combined an mHealth solution with quality improvement structures
• Used quarterly monitoring data to inform intervention support and refinement of interventions
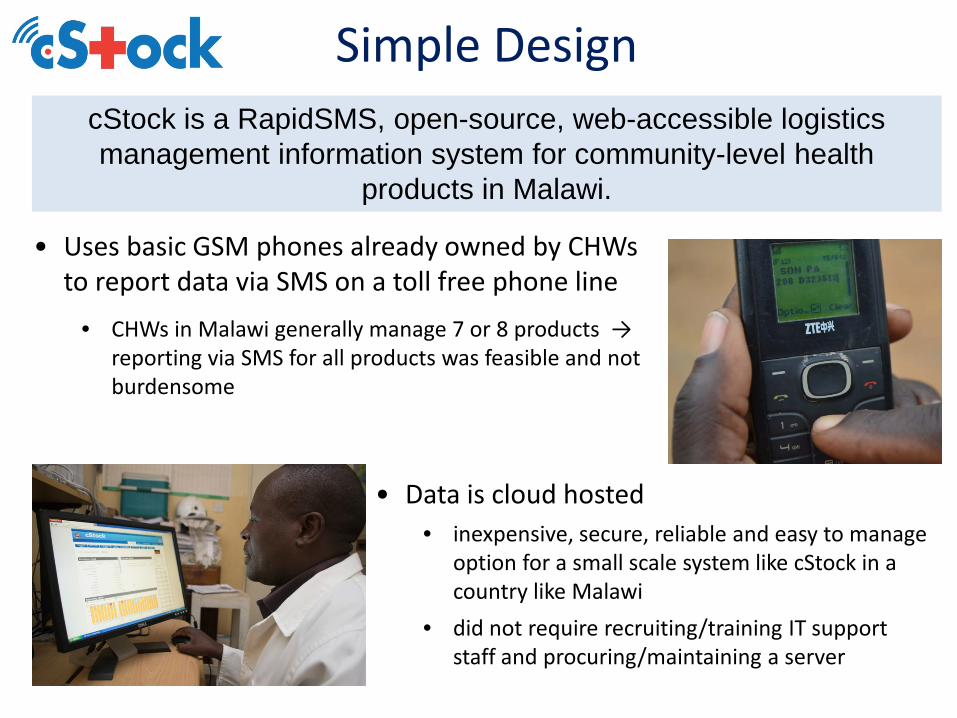
Simple Design cStock is a RapidSMS, open-source, web-accessible logistics management information system for community-level health
products in Malawi.
• Uses basic GSM phones already owned by CHWs to report data via SMS on a toll free phone line
• CHWs in Malawi generally manage 7 or 8 products → reporting via SMS for all products was feasible and not burdensome
• Data is cloud hosted • inexpensive, secure, reliable and easy to manage
option for a small scale system like cStock in a country like Malawi
• did not require recruiting/training IT support staff and procuring/maintaining a server
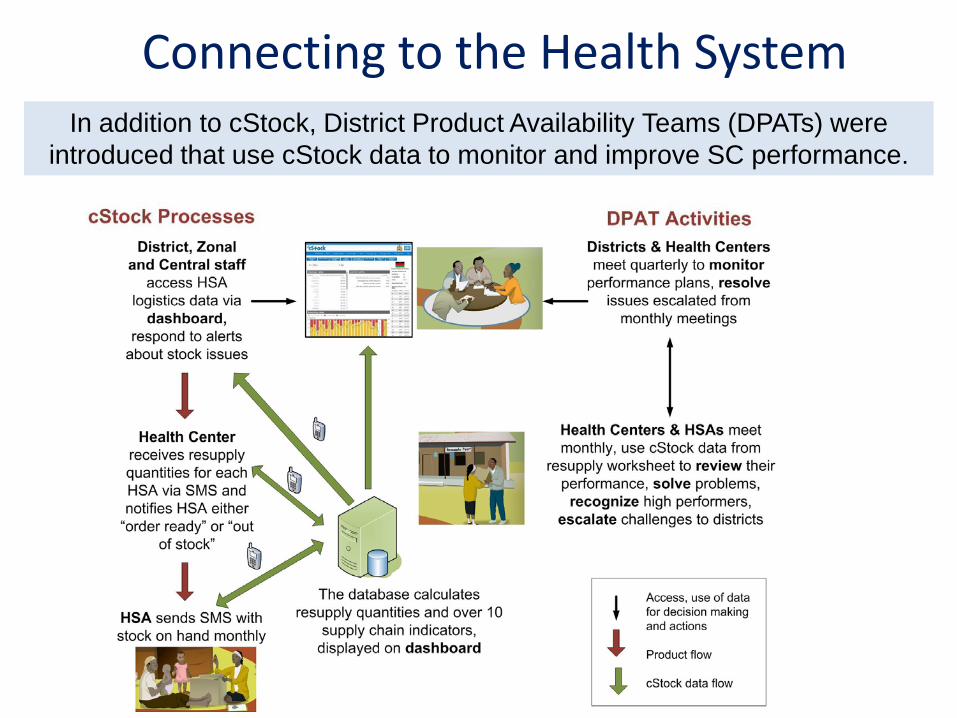
Connecting to the Health System In addition to cStock, District Product Availability Teams (DPATs) were
introduced that use cStock data to monitor and improve SC performance.
Stakeholder Consultation
• Engage MOH and partners from the outset – Project consulted with the MOH and stakeholders when
designing the intervention and throughout the pilot phase.
– Evaluation and monitoring data was shared through meetings and with individuals.
• Results: Six months after the 6 pilot districts were trained in 2011, a partner recognized the success of cStock and mobilized resources to scale up to another 9 districts.
– Partnering to Scale builds broader ownership and capacity that lasts after project ends
• Project and MOH worked with partners to mobilize resources and plan scale up together
– Results: • By end of 2014 all 29 districts (3059 HSAs) were trained in cStock and the
DPAT s with funding from WHO, Save the Children, UN Foundation, USAID and SC4CCM
• Reporting rates to cStock are consistently around 85% (vs. 43% at BL)
Moving from Pilot to Scale
Catalytic Event: Senior MOH Management Team endorsed scale up of mHealth innovation before midline evaluation based on positive feedback from users of the system.
Starting before the end of pilot (2012) SC4CCM
• Formation of a taskforce (MOH chair) with all stakeholders dedicated to institutionalization of cStock and DPATs
• Formation of National Product Availability Team to monitor implementation and provide follow up support to users
• Finding champions in MOH by having central level advocates and trainers in every districts
• Capacity building of MOH to provide management and leadership, currently have a secondee in MOH
Transfer of Operational Ownership
• Development of comprehensive, five year transition plan with cost estimates for resource mobilization, in the short term, and eventual transition to MOH budget
Lessons Learned • Design Well
– Consider sustainability - scalability, institutionalization and integration – from the design phase
– Keep the design simple and suitable for the context
– Use a whole systems approach: combining an mHealth solution with system strengthening interventions such as quality improvement processes
• Engage partners and MOH from the outset and consider partnering for scale up
• Use data to monitor and refine interventions and consult with stakeholders to get input
• Develop a transition plan well before the end of the project and help set the ground work for sustainability

ore information on cStock visit: //sc4ccm.jsi.com/cstock/
Scaling up iCCM: coordination for supply chain management
Some complexities in SCM when scaling up iCCM:
Different programs within the MoH involved
Different donors for different commodities each with different funding cycles and reporting
Many implementing partners
Different distribution procedures, reporting systems & supervision mechanisms
Demand for iCCM may change rapidly during scale up
Procurement process can take up to 12 months
Same products used at community level as in facilities
Country examples of coordination Guinea example: coordination for procurement • iCCM quantification committee
established • Forecasting and coordinated supply
plan developed, considering all orders in the pipeline
• Forecast used by IMCI unit for mobilizing resources for procurement
• Supply plan monitored and revised
Rwanda: coordination for resupply procedures • Many implementing partners
with different forms & resupply procedures
• MoH organized a review workshop- inclusive process
• Harmonized resupply procedures and forms for use by all CHWs
Key messages • Communication and coordination between
programs within the MoH, partners and donors to maximize resources and ensure supply functions at all levels of the system
• Integrate: – parallel iCCM programs into the health system – iCCM supplies into pharmaceutical system
• Need careful planning and a clear strategy for expansion