Embed Size (px)
Citation preview


Fluid & Electrolyte Balance
Dr . N. Sivaranjani ,MD biochem
Asst prof.

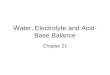
60% of body consists of fluid
Intracellular space
Extracellular space
Distribution of water in different body water compartments depends on the solute
content of each
compartment
Osmolality of the intra andextra-cellular fluid is the same, but there is marked difference in the solute content.Dr. N. Sivaranjani 3

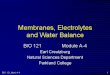
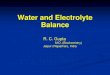
Distribution of Body Water
Intravascular
Interstitial
IntracellularICF
ECF Na+
K+
Cl-
Essential for normal cell function
Provides medium for metabolic processes
spaces between cells
plasma-arteries, veins, capillaries
Cerebrospinal fluid, Pleural spaces, Synovial spacesPeritoneal fluid spaces
Transcellular1 L
Dr. N. Sivaranjani 4

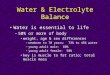
Fluid composition varies with body fat, age and gender
75% water
ECF=45%,ICF=30%65% water,
ECF= 25%, ICF = 40%
Adult female
50% water, ECF=10-15%, ICF=40%
fat cells contain little water and lean tissue is rich in water, the more obese the person, the smaller the percentage of total body water. Dr. N. Sivaranjani 5

Human life is suspended in a saline solution having a salt concentration of 0.9%
Body fluids must remain fairly constant with regard to amount of H2O & specific electrolytes
Primary component of body fluid: WaterWomen lower % body water than menTotal body water decreases with age
Dr. N. Sivaranjani
6

How importance is water Water provides a medium for transporting nutrients to cells and
wastes from cells and for transporting substances such as hormones, enzymes, blood platelets, and red and white blood cells
Water facilitates cellular metabolism and proper cellular chemical functioning
Water acts as a solvent for electrolytes and nonelectrolytes
Helps maintain normal body temperature
Facilitates digestion and promotes elimination
Acts as a tissue lubricant
Component in all body cavities [parietal, pleural… fluids]
Water is the principal body fluid which is essential for life.
Dr. N. Sivaranjani 7

Intake and output of water
Factors that Dictate Body Water Requirement
1) Amount needed to give the proper osmotic concentration2) Amount needed to replace water lost excretion
Normal Routes of water gain and loss
INTAKE OUTPUTml/day ml/day
Exogenous :-
Fluid intake 1,500
Food 700
Endogenous :-
Metabolism 300
TOTAL 2,500
Insensible loss (skin + lung) 850
Feces 150
Urine (kidney) 1,500
TOTAL 2,500

Dr. N. Sivaranjani 9

Regulation of Body Fluid Compartments
Diffusion
Molecules → from an area of ↑ concentration to an area of ↓concentration
Osmosis
is the movement of water through a semipermeable membrane to a higher concentration of solutes.
Active Transport
is movement of substance across permeable membrane and gradient; requires energy and pump.
Filtration
H2O & dissolved substances → from an area of high hydrostatic pressure to an area of low hydrostatic pressure
Dr. N. Sivaranjani 10

Diffusion
High Solute Concentration Low Solute Concentration
Fluid
Solutes
Dr. N. Sivaranjani 11

Osmosis
Fluid
High Solution
Concentration,
Low Fluid
Concentration
Low Solute
Concentration,
High Fluid
Concentration
Controls body fluid movement between ICF & ECF
Dr. N. Sivaranjani 12

Dr. N. Sivaranjani
13

Dr. N. Sivaranjani 14

Osmotic Pressure
The amount of hydrostatic pressure required to stop the flow of water by osmosis
Osmolality
reflects the concentration of fluid that affects the movement of water between fluid compartments by osmosis
Dr. N. Sivaranjani 15

Osmolality : Number of osmotically active particles present per kilogram of water.
Osmolarity: Number of osmotically active particles present per litre of water.
Electrolytes: Electrolytes are substances whose molecules dissociate into ions when placed in solution
Ions : An ion is an atom or group of atoms with an electrical charge.
Dr. N. Sivaranjani 16

Normal plasma Osmolality = 285-292 mOsm/kg
Plasma osmolality can be measured directly using the osmometer
or indirectly as the concentration of effective osmoles
Osmolality =2(Na+) + 2(K+) + Urea + Glucose, mmol/L.
Plasma osmolality (mmol/kg) = 2x Plasma Na+(mmol/l)
Estimated by doubling serum Na concentration
Clinical uses :- diagnosis of disorders of water and electrolyte
balance and NKHC
Osmolality increases – Hyperglycemia, DKA, NKHC, Hypernatremia with water loss (DI)
Decreased – Hyponatremia – water and Na gain (CCF), SIADH. Dr. N. Sivaranjani 17

The difference in measured osmolality and calculated osmolality called Osmolar Gap. (normal - numerically similar)
Increase in osmotically active substances – Ethanol, Mannitol, neutral and cationic amino acids.
Fractional water content of plasma is reduced –hyperlipidemia or hyperproteinemia .
Dr. N. Sivaranjani 18

In a healthy state, the osmotic pressure of ECF, mainly due to Na+ ions, is equal to the osmotic pressure of ICF which is predominantly due to K+ ions
Dr. N. Sivaranjani
19

Tonicity - measure of transport of water across the biological system causing change in cell volume.
0.9% Normal SalineDr. N. Sivaranjani
20

0.9% Normal Saline
Dr. N. Sivaranjani
21

(0.45% NS)< concentration of solutes as plasma
Causes H2O to move into cells & swell (hemolysis)Dr. N. Sivaranjani
22

(3% NS)
> concentration of solutes as plasma
Causes H2O to draw out of cell (shrink)
Mannitol –treatment of cerebral edema.
Dr. N. Sivaranjani
23

Dr. N. Sivaranjani
24

ELECTROLYTES
Substances whose molecules dissociate into ions (charged particles) when placed into waterCations: positively-chargedAnions: negatively-charged
Sodium – major cation of ECF Chloride - major anion of ECF
Potassium – major cation of ICF Phosphate – major anion of ICF
Dr. N. Sivaranjani 25

ELECTROLYTE Composition
Electrolyte Conc Plasma (mEq/L) ICF
Sodium, Na+ 142 10 Potassium, K+ 5 150Calcium, Ca++ 5 2Magnesium, Mg++ 3 40
(155)
Chloride, Cl- 103 2Bicarbonate, HCO3
- 27 10Biphosphate, HPO4
- 2 140Sulfate, SO4
-2 1 5Protein 16 40Organic acids 6 5
(155)Dr. N. Sivaranjani 26

Functions of Electrolytes
Promote neuromuscular irritability
Regulate acid and base balance
Regulate distribution of body fluids among body fluid compartments
Dr. N. Sivaranjani 27

are regulated together
kidneys play a predominant role
major regulatory factors are the hormones - Aldosterone, ADH and Renin angiotensinAtrial natriuretic peptide
Hypothalamic regulation - Stimulates thirst and ADH release Pituitary regulation - Releases ADH Adrenal cortical regulation – Releases Aldosterone Renal regulation - Primary organs for regulating fluid and electrolyte balance
Selective reabsorption of water and electrolytesRenal tubules are sites of action of ADH and aldosterone
Electrolyte and water balance
Dr. N. Sivaranjani 28

Synthesis Action Action on sodiumand water
Aldosterone secreted by the zonaglomerulosaof the adrenal cortex
regulates theNa+ → K+ exchange and Na+ → H+ exchange atthe renal tubules.
Sodium and waterretention
Anti-Diuretic Hormone (ADH)
Under control of hypothalamus, posterior pituitary releases ADH
increase the waterreabsorption by the renal tubules.
Retention ofwater
Renin-Angiotensin System
release of renin by the juxtaglomerular cells
Angiotensin-II BP by vasoconstriction of the arterioles.It also stimulates
aldosterone production
Retention of sodium and water
Atrial natriuretic peptides
stimulation of atrial stretch receptors
Inhibit renin and aldosterone secretion –cause elimination of sodium
Increases urinary excretion of sodium.Dr. N. Sivaranjani 29

DECREASED FLUID VOLUME
Stimulation of thirst
center in hypothalamus
Increase in thirst
↑ intake of water
INCREASES PLASMA OSMOLALITY
Dr. N. Sivaranjani 30

Posterior pituitary
gland
Osmoreceptors in
hypothalamus + ↑Osmolarity
↑ADH
Kidney
↑H2O reabsorption
↑vascular volume and
↓osmolarity
Stress, hypoglycaemia,
Anesthetic agents, Heat,
Nicotine, Antineoplastic
agents, Narcotics,
Surgery
ANTIDIURETIC HORMONE REGULATION MECHANISMS
Fluid
volume
Increase permeability of renal
collecting ducts to water by
binding to V2 receptors –
cause insertion of water
channels to luminal
membrane

Juxtaglomerular cells↓Serum Sodium
↓Blood volume
↓Blood Pressure
↓renal blood flow Angiotensin I
Distal renal
tubules
Angiotensin II
Adrenal Cortex↑Sodium reabsorption (H2O
resorbed with sodium)
Angiotensinogen in
plasmaRENIN
Angiotensin-
converting enzyme
ALDOSTERONE
Via vasoconstriction of arterial smooth muscle
ALDOSTERONE-RENIN-ANGIOTENSIN SYSTEM
Increases Blood Pressure

INCREASED BLOOD VOLUME ,
INCRESED BLOOD PRESSURE
ATRIAL NATRIURETIC PEPTIDE RELEASE
Reduces in thirst
Decreased intake of water
STIMULATION OF ATRIAL STRETCH RECEPTORS
Inhibits release of ADH
Diuresis – increase urine output
Inhibits release of
Aldosterone
Decreases Na reabsorption
Natriuresis – Na excretion

Dr. N. Sivaranjani
34

Volume Disorders 2° Alteration in Sodium Balance
ECF Expansion
Isotonic Inc N N Water and Na retention – Edema- 2 ̊ Cardiac failure2 ̊ Hyper- aldosteronism due to hypoalbunemia.
Hypertonic Inc Dec Inc Na retention due to excess mineralocorticoid –cushing’s syndrome or conn’s syndrome
Hypotonic Inc Inc Dec water retention due to ADH excess or Glomerular dysfuncion
Volume ECF ICF Conditions
Disorder Vol. Vol. Osmolality

ECF Contraction Isotonic Dec N Normal loss of Na & water
common cause – loss of GIT fluid SI obstruction, SI fistulae, paralytic ileus
Hypertonic Dec Dec Increased water depletionDiarrhea – Commonest cause Diabetes insipidus - rare
Hypotonic Dec Inc Decreased sodium depletioninfusion of IV fluids with low Na-dextrosealdosterone deficiency- Addison’s disease
Volume ECF ICF Conditions
Disorder Vol. Vol. Osmolality

• Dehydration • Fluid Overload
Dr. N. Sivaranjani 37

Dehydration / water depletion
Pure (tissue) water loss – less common
Depletion of Na and water – more common
and hypovolemia to sodium loss and thus loss of blood volume.
Dr. N. Sivaranjani 38

Causes of water depletion :
Decreased intake of water –
• Inadequate water supply
• Mechanical obstruction for drinking
• Impaired response of thirst center – Comatose patient
Increased loss of water –
• Increased renal loss of water – RTA, DI
• Increased loss of water from skin – Burns,
excessive sweating
• Increased loss through lungs – hyperventilation
• Increased loss of gut – vomiting ,diarrhea Dr. N. Sivaranjani 39

Earliest Detectable Signs
low BP
Dry skin and mucous membranes
Sunken eye balls, fontanels
Circulatory Failure (coolness, mottling of extremities)
Loss of skin elasticity
Delayed cap refill
lethargy , confusion and coma Dr. N. Sivaranjani 40

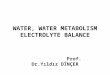
Skin turgor assessment – this assessment can be done on the forearm. Skin that does not flatten immediately after release is called “tenting”, an example of fluid volume deficit.
Dry and cracked lips
Sunken eyes
Thirst and discomfort
Dr. N. Sivaranjani 41

Loss of Skin Elasticity due to dehydration
Dr. N. Sivaranjani 42

Dr. N. Sivaranjani 43

Manifestations of ECF Deficit (Dehydration)
Signs & Symptoms
Weight loss
Blood pressure drop
Delayed capillary refill
Oliguria
Sunken fontanel
Decreased skin turgor
Physiologic Basis
Decreased fluid vol.
Inadequate circ. Blood
Decreased vascular volume
Inadequate kidney circ.
Decreased fluid volume
Decreased interstitial fluid
Dr. N. Sivaranjani 44

Degrees of Dehydration
Mild Moderate SevereFluid Vol loss <50ml/kg 50-90ml/kg >100 ml/kg
Skin Color Pale Gray Mottled
Skin Elasticity Decreased Poor Very Poor
M.M. Dry Very Dry Parched
U.O. Decreased Oliguria Marked Oliguria
BP Normal Normal or lowered
Lowered
Pulse Normal or Increased
Increased Rapid, thready
Dr. N. Sivaranjani 45

Biochemical finding : plasma sodium – increased urine volume – decreased urine concentrated
Treatment :Aim - Expand ECF volume and improve circulatory and renal function plenty of water Treatment of underlying causes Replacement of fluid deficit –
5% dextrose

Water intoxication / water excess /over hydration
predominant water excess
Decrease in serum Na+
Causes :
Excessive intake of water
Compulsive drinking of water – psychogenic polydypsia
Excessive administration of fluid through parental route
Impaired renal excretion of water
Severe renal failure
SIADH syndrome of inappropriate ADH
Drugs acting as vasopressin agonistDr. N. Sivaranjani 47

SIADH – Plasma hypo-osmolality Normal renal , thyroid, adrenal function Increased urine Na excretion Dilutional hyponatremia Elevated serum ADH
Clinical features Behavioral disturbances Confusion Headache Muscle twitching Convulsion Coma

Biochemical finding :
plasma sodium – decreased
decreased plasma osmolality
urine dilated
Treatment :
Treatment of underlying causes
Fluid restriction
SIADH – vasopressin antagonist

50
Edema
the accumulation of fluid within the interstitial space
Causes:
•increased hydrostatic pressure
• venous obstruction, lymphedema, CHF, renal failure
•lowered plasma osmotic pressure (protein loss)
• liver failure, malnutrition, burns
•increased capillary membrane permeability
• Inflammation, sepsis
Dr. N. Sivaranjani

Dr. N. Sivaranjani
51