Embed Size (px)
DESCRIPTION
TB treatment principles by Daniel schwartz - LSMU
Citation preview

Tuberculosis Tuberculosis treatment:treatment:
general principles general principles and approachand approachLecturer: Ph.D Lecturer: Ph.D M.G.DolynskaM.G.Dolynska

Historical backgroundHistorical background Supposed incurable until XX Supposed incurable until XX
centurycentury First approach – sanatorium First approach – sanatorium
movementmovement First pathogenically based attempt First pathogenically based attempt
–artificial pnemothorax –artificial pnemothorax (Forlanini, (Forlanini, 1882) 1882)
StreptomycinStreptomycin discovery discovery (Zelman (Zelman Waksman, 1943)Waksman, 1943)

The AIMS of treatment of The AIMS of treatment of tuberculosis are:tuberculosis are:
to cure the patient of TB;to cure the patient of TB; to prevent death from active TB to prevent death from active TB
or its late effects;or its late effects; to prevent relapse of TB;to prevent relapse of TB; to decrease transmission of TB to decrease transmission of TB
to others;to others; to prevent the development of to prevent the development of
acquired drug resistance.acquired drug resistance.

DOTS (DOTS (Directly observed Directly observed treatment short coursetreatment short course), Karel ), Karel
Styblo, 1972Styblo, 1972The organizational principles of the The organizational principles of the
DOTS are:DOTS are: availability of a decentralized availability of a decentralized
diagnostic and treatment network diagnostic and treatment network based on existing health facilities;based on existing health facilities;
good programme management based good programme management based on accountability and supervision of on accountability and supervision of health care workers;health care workers;
an evaluation system of case-finding an evaluation system of case-finding and cohort analysis of treatment and cohort analysis of treatment outcomes.outcomes.

The five elements of the The five elements of the expanded DOTS framework expanded DOTS framework
are:are: 1.Sustained political commitment to increase human and 1.Sustained political commitment to increase human and
financial resources and make TB control a nationwide financial resources and make TB control a nationwide priority integral to the national health system.priority integral to the national health system.
2. Access to quality-assured TB sputum microscopy for 2. Access to quality-assured TB sputum microscopy for case detection among persons presenting with, or case detection among persons presenting with, or found through screening to have, symptoms of TB found through screening to have, symptoms of TB (most importantly, prolonged cough). (most importantly, prolonged cough).
3. Standardized short-course chemotherapy for all cases 3. Standardized short-course chemotherapy for all cases of TB under proper case management conditions, of TB under proper case management conditions, including direct observation of treatment.including direct observation of treatment.
4. Uninterrupted supply of quality-assured drugs with 4. Uninterrupted supply of quality-assured drugs with reliable drug procurement and distribution systems.reliable drug procurement and distribution systems.
5. Recording and reporting system enabling outcome 5. Recording and reporting system enabling outcome assessment of all patients and assessment of overall assessment of all patients and assessment of overall programme performance.programme performance.

Dosage and abbreviation of Dosage and abbreviation of essential antituberculosis essential antituberculosis
drugsdrugsDrug (abbreviation) Recommended dosage
(dose range) in md/kgDaily 3 times weekly
Isoniasid (H) 5(4-6)
10(8-12)
Rifampicin (R) 10(8-12)
10(8-12)
Pyrasinamide (Z) 25(20-30)
35(30-40)
Streptomycin (S) 15(12-18)
15(12-18)
Ethambutol (E) 15(15-20)
30(20-35)

Basical treatment regimensBasical treatment regimens Diagnosticcategory
TB patients Treatment regimenI
Initial phase Continual phase
I New smear-positive patients; new smear-negative PTB with extensive parenchymal involvement; concomitant HIV disease or severe forms of extrapulmonary TB
Preferred2 HRZEI
Preferred4 HR4 (HR)3
Optional or2 (HRZE)3
or2 HRZEIV
Optional4 (HR)3or6 HEV
II Previously treated sputum smearpositivePTB:- relapse;- treatment after default
Preferred2 HRZES / 1 HRZEVI
Preferred5 HREVI
Optional2(HRZES)3/1HRZE3
Optional5 (HRE)3

Basical treatment regimensBasical treatment regimens(continued)(continued)
Diagnosticcategory
TB patients Treatment regimenI
Initial phase Continual phase
III New smear-negative PTB (other than in category I) and less severe forms of extra-pulmonary TB
Preferred2 HRZEVIII
Preferred4 HR
Optional2 (HRZE)3
Optional4 (HR)3or6 HE
IV Chronic (still sputum-positive after supervised re-treatment); proven or suspected MDR TB cases.
Specially designed standardized or individualized regimens
WHO/CDS/TB/2003.313 Treatment of tuberculosis:guidelines for national programmes, third edition. Revision approved by STAG, June 2004

Criticism concern with the Criticism concern with the DOTS strategyDOTS strategy
ClinicalClinical• Lack of smear-negative case detectingLack of smear-negative case detecting• Lack of case monitoringLack of case monitoring EthicalEthical• Treatment refusal for certain categories Treatment refusal for certain categories
(especially chronic and smear-negative)(especially chronic and smear-negative) EpidemiologicalEpidemiological• Potential hazard of untreated treated in Potential hazard of untreated treated in
improper way patientsimproper way patients

Expanded treatment Expanded treatment conceptionconception
Appropriate antibacterial treatment.Appropriate antibacterial treatment. Hygienic and dietary regimen.Hygienic and dietary regimen. Pathogenetic measures:Pathogenetic measures:• desintoxicationdesintoxication• hepatotropic therapyhepatotropic therapy• tissue stimulationtissue stimulation CollapsotherapyCollapsotherapy Surgical treatment.Surgical treatment.

For the future, the top priority remains to administer standardized short
course chemotherapy regimens to all smear positive cases (new and
retreatment cases). This priority requires the maximum of effort, time,
drugs and money in a national tuberculosis programme, without
diverting funds and resources to smear negative and/or chronic cases.

Drug resistanceDrug resistance PrimaryPrimaryConcern with drug-resistant Concern with drug-resistant
strains inoculationstrains inoculation AsquiredAsquiredProduced by ineffective treatmentProduced by ineffective treatment

Drug resistanceDrug resistance Simple drug resistance– Simple drug resistance–
resistance to more than two resistance to more than two first line drugs including first line drugs including isoniasid or rifampicinisoniasid or rifampicin
Multidrug-resistance (MDR) – Multidrug-resistance (MDR) – resistance to more than two resistance to more than two first line drugs including both first line drugs including both isoniasid and rifampicinisoniasid and rifampicin

Main resistance typesMain resistance types
Resistance
mono
MDR
poly
XDRXDR

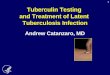
MDR-TB MDR-TB prevalence among new cases and prevalence among new cases and countries in which at least one countries in which at least one XDR-TBXDR-TB
case has been reportedcase has been reported
At the end of 2006 year XDR-TB has been detected in 17 countries

Extensively drug resistance (XDR) Extensively drug resistance (XDR) – main definitions– main definitions
Firstly has been proposed by US Centers of Disease Firstly has been proposed by US Centers of Disease Control and Prevention (CDC) in March,Control and Prevention (CDC) in March, 2006: 2006: the the disease, caused by MBT, resistant to HR (MDR-disease, caused by MBT, resistant to HR (MDR-TB)TB) and to at least 3 from six classes of and to at least 3 from six classes of antituberculosis second-line drugs antituberculosis second-line drugs (aminoglycosides, polypeptide, fluoquinolones, (aminoglycosides, polypeptide, fluoquinolones, thyamides, cyclocerine, PAS) thyamides, cyclocerine, PAS)
But on WHO meeting devoted to XDRBut on WHO meeting devoted to XDR problem (meeting problem (meeting of the WHO XDR-TB Task Forceof the WHO XDR-TB Task Force), ), on October, on October, 10-1110-11,, 2006 2006 difinition has been changeddifinition has been changed: : the disease, the disease, caused by MBT, resistant to HR (MDR-TB)caused by MBT, resistant to HR (MDR-TB) and to and to at least some fluoquinolones and one from 3 at least some fluoquinolones and one from 3 injectional antituberculosis drugs :injectional antituberculosis drugs : cyclopentincyclopentin, , kanamycin, amicacinkanamycin, amicacin. .

Second line drugsSecond line drugs Less effectiveLess effective More toxic More toxic Much more expensiveMuch more expensive

Classes of second-line antituberculosis drugs
a AminoglycosidesWhen resistance to streptomycin is proved or highly suspected,
one ofthe other aminoglycosides can be used as a bactericidal agent
againstactively multiplying organisms:• kanamycin, the least expensive, but largely used for
indications otherthan tuberculosis in some countries.• amikacin, as active as kanamycin and better tolerated, but
much moreexpensive.• capreomycin,2 very expensive but very useful in cases with
tuberclebacilli resistant to streptomycin, kanamycin and amikacin.

Classes of second-line antituberculosis drugs
b ThioamidesEthionamide or prothionamide are 2 different presentations of thesame active substance, with bactericidal activity. Prothionamide may
bebetter tolerated than ethionamide in some populations.c FluoroquinolonesOfloxacin and ciprofloxacin are two different drugs, but with completecross-resistance within the group. These drugs have a low bactericidalactivity, and are useful in association with other drugs. Thepharmacokinetics of ofloxacin are better than the pharmokinetics ofciprofloxacin. Sparfloxacin should be avoided because of severecutaneous side effects (photo-sensitisation). Norfloxacin should not beused, because it does not give adequate serum levels.

Classes of second-line antituberculosis drugs
d Cycloserine (or terizidone)This is the same bacteriostatic agent,
with 2 different formulations. It hasno cross-resistance with other
antituberculosis agents. It might bevaluable to prevent resistance to other
active drugs, but its use is limitedby its high toxicity.

Classes of second-line antituberculosis drugs
Para-aminosalicylic acid (PAS)This is a bacteriostatic agent, valuable for preventing resistance toisoniazid and streptomycin in the past and to other bactericidal
drugs today.f OthersOther drugs, sometimes mentioned as second line antituberculosisdrugs, have no place in the treatment of MDR tuberculosis:• rifampicin derivatives, like rifabutin (21), cannot be used since
there is almost complete cross-resistance between rifabutin and rifampicin
(especially when there is acquired resistance to rifampicin);• clofazimine has some activity against Mycobacterium leprae andMycobacterium ulcerans, but no activity against Mycobacteriumtuberculosis.

Acceptable regimen for the treatment of MDR Tuberculosis

It must be made clear to the patient and staff that meticulously taking the prescribed reserve regimen is all that stands between the patient and death.

Recovery criteriaRecovery criteria Clinical symptoms Clinical symptoms
disappearingdisappearing Morphological changes Morphological changes
resolvingresolving Sputum conversion (by all Sputum conversion (by all
available tests)available tests)


TB and HIV treatment TB and HIV treatment sequencesequence