Embed Size (px)
Citation preview

Michael Fingerhood MD FACP

None, except strong passion for integrating addiction treatment with primary care

To increase knowledge of epidemic of opioid use disorder
To increase knowledge of treatment of opioid use disorder
To be convinced that integrating treatment for substance (opioid) use disorder with primary care is beneficial (for patient, providers and the health system)



“SWAF”




In 2006, the IOM released a report recommending improvement in coordination of mental health and substance-related services into general health care services:
“Available evidence suggests that integration of mental health and primary care may lead to improved care and quality of life”
“With the advent of health care reform, community-based health centers will be increasing their capacity for behavioral health care. Workforce development and systems factors will need to be addressed in order to make this happen”
“Studies of health delivery, process of care, and health outcomes in integrated clinical settings will be critical to inform the process”

Desire to receive care that will improve health
Ability to receive care based on trust and rapport
Press K, Zornberg G, Geller G, Carrese J, Fingerhood M. What patients with addiction disorders need from their primary care physicians: a qualitative study. Substance Abuse 2016; 37:349-55.

Knowledge about addiction
Duty to treat
Focus on overall health
Engage patients in care
Treat the full scope of illness (isolation, rejection, creating hope)

In 2015, an estimated 25 million persons aged 12 or older (9.4 percent) were current illicit drug users
◦ Despite the high prevalence, the vast majority of individuals who need treatment do not receive it
◦ The economic burden of substance use in the US is estimated at $524 billion/year much of which is attributed to losses in productivity
In 2015, over 4.5 million Americans aged 12 and older met the criteria for substance use disorder related to opiate analgesics, and over 700,000 used heroin in the past year
According to the CDC, drug overdose death rates in the US have more than tripled since 1990 and are at an all-time high, surpassing motor vehicle accident deaths
NSDUH 2011, CDC 2011

1. Boredom from lectures like this
2. Voted for Nixon’s re-election
3.Won a Super Bowl 4.Love Uncle John’s
Band 5.Opioid use
disorder

“Seventy glassine baggies of heroin packed for individual sale — at least 50 of them unopened — were discovered in the $10,000-a-month rental where the Oscar-winning actor was found dead Sunday with a needle stuck in his left arm
Some of the envelopes had the words ‘Ace of Spades’ written on them, and others were stamped with the name ‘Ace of Hearts.’ Both are brands of heroin that are often cut with a powerful pain reliever called fentanyl...”

“Prince died unexpectedly at his home in Minnesota on April 21. According to the Associated Press, Prince died of an overdose from fentanyl, a highly potent opioid”



“According to most firsthand accounts of his days at Johns Hopkins, Halsted was moody, elusive, sarcastic, and prone to dropping out in the middle of an operation ... Most famously, Dr. William Osler recalled in 1890 that he had seen the surgeon having severe chills. Suspecting that Halsted was still addicted to morphine and was going through withdrawal, Osler gained the surgeon's trust and confidence.”

In a secret diary that Osler kept sometime between 1902 and 1905, which was not unsealed until 1969, Osler wrote, "[Halsted] has never been able to reduce the amount to less than three grains [of morphine] daily, on this he could do his work comfortably and maintain his excellent physical vigor. . . I do not think that anyone suspected him — not even Welch."

28F seen for first visit. Able to review in CRISP/PDMP- multiple ER visits for back pain and one opioid overdose, and many filled scripts for oxycodone from many providers. Had abnormal PAP 3 years ago. History of HIV (not addressed) and hypertension (has elevated BP today)
Her agenda- getting script for oxycodone. My agenda- getting her engaged in medical care and treatment for opioid use disorder

First cultivation of opium poppies was in Mesopotamia, approximately 3400 B.C., plant called Hul Gil, the "joy plant”
The Greek gods Hypnos (Sleep), Nyx (Night), and Thanatos (Death) were depicted wreathed in poppies
The Persian physician, al-Razi (845-930 A.D.) made use of opium in anesthesia and recommended its use for the treatment of melancholy.

Between 400 and 1200 AD, Arab traders introduced opium to China.
14th century Ottoman Empire-opium used to treat headache and back pain.
15th century China- first officially recorded use of opium as a recreational drug.
1874- heroin developed 1898-heroin marketed by Bayer as safe
pediatric cough suppressant


Opiates = naturally present in opium
e.g. morphine, codeine, thebaine
Opioids = manufactured
Semisynthetics are derived from an opiate
Heroin from morphine
Buprenorphine, oxycodone from thebaine
Synthetics are completely man-made to work like opiates
Methadone
Fentanyl

1914- Harrison Narcotics Tax Act
1925- Linder vs United States
1964- Methadone introduced as experimental treatment for opioid addiction
1968- Bureau of Narcotic and Dangerous Drugs formed (changed to DEA in 1973)

1. Tolerance2. Withdrawal3. Larger amounts/longer period than
intended4. Inability to/persistent desire to cut down or
control5. Increased amount of time spent in activities
necessary to obtain6. Social, occupational and recreational
activities given up or reduced7. Use continued despite adverse
consequences

Ask
Survey/screening tools
Clinical assessment
Local medical record
CRISP/PDMP
Search criminal record?

A. Primary care
B. Emergency room
C. Inpatient hospital
D. All places equally

SBIRT
vs
SIT (screen, intervene and treat)

Interventions and education are effective Interventions should emphasize health and
relationship benefits Use family/friends in a positive way Avoid threats- “If you use, you will die” Give hope that life can improve Acknowledge reasons for use, but… Work together to define the benefits of change


1. Accepting powerlessness
2. Disease identification
3. Surrender to a Higher Power
4. Commitment to AA/NA
5. Commitment to abstinence
6. Sober social support
7. Intention to avoid high-risk situations

Stabilize neuronal circuitry◦ Mu occupation/blockade
◦ Cross-tolerant, long-acting
Prevent withdrawal and craving
Extinguish compulsive behavior
Prevent spread of HIV and HCV
Prevent criminal activity

Pure opioid blocker
Available as oral drug and monthly injection
Acceptance poor
Works if part of contingency management
Little evidence for long term efficacy

Opiate dependence is a brain-related medical disorder
Treatment is effective-
“Although a drug-free state represents an optimal treatment goal,
research has demonstrated that this goal cannot be achieved or
sustained by the majority of opiate-dependent people.”
Reduce unnecessary regulation of long-acting agonist
treatment programs
Improve training of health care professionals in treatment
of opiate dependence

Dole, Arch Int Med, 1966

MEDICATIONS
NOT MAT


H H HH
H H HH
H H HH
H H HH
H
H H HH
H H HH
H H HH
H H HH
H
Methadone Regular Outpatient
Baseline

P H HH
H
P HP
H H HH
H H HH
H H H
Methadone No Methadone
After 2 Years
1
32
1- Sepsis & endocarditis
2- Leg amputation
3- Sepsis

P H H
H
P P
P
Methadone No Methadone
After 5 Years



0
5
10
15
20
25
30
35
40
45
Baseline 1 yr. 2 yr. 3 yr.
% s
ero
po
sit
ive
Methadone Out-of-treatment

Less than 20% of opioid dependent persons receiving treatment
Stigma associated with going to a methadone clinic
Highly regulated doses & take homes
Criteria exclude persons under age 18
Ability to get to treatment limited- based on geography and insurance as well

Allowed “Qualified” physicians to treat opioid
dependence outside methadone facilities
1. Addiction certification from approved organization, or
2. Physician in clinical trial of qualifying medication, or
3. Complete 8-hour course from approved organization
DEA issues (free) to qualifying physicians a new
DEA number to use medication for opioid
dependence
As of today, only one medication formulation is
approved for this use

Methadone Clinic Buprenorphine
• Criteria:
Withdrawal
12 months use
• Criteria:
DSM IV
No time criteria
• Dose regulated • MD sets dose
•Age > 18 •Age > 16
• Limited take homes • Take homes (30 days)
• Services “required” • Services must be “available”

Perc
ent
Reta
ined
0
20
40
60
80
100
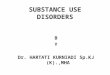
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
58% Bup
73% Hi Meth
53% LAAM
Stud(9Johnson RE, et al NEJM 2000

Modest agonist activity with ceiling
Long half life
Precipitated withdrawal if taken after full
agonist
Sublingual route of administration
“Combo” tablet with naloxone limits abuse by
injection

No alteration of cognitive functioning
◦ feel “normal”
No organ damage
◦ Early concern of hepatic toxicity unconfirmed
◦ No evidence of QT prolongation
Ceiling prevents respiratory depression/overdose
(Overdose reports with combining use with benzodiazepines)
No clinically significant interactions with other drugs


Done at home
No different than starting blood pressure medication- may need some titration
Much easier than starting insulin (and safer)
Counsel on taking first dose once in withdrawal
Titrate dose up to 16 mg/daily by second day
Phone check ins
One week follow-up


Multicenter randomized clinical trial- n=653
In both phases patients randomized to standard
medical management(SMM) or SMM plus
counseling
In both phases (3 &12 weeks of buprenorphine),
separate counseling did not change outcomes


“You’re not in recovery if you’re on medication”

“Doc, I feel normal”
“I wake up not sick”
“I have my life back”
Treatment in normal medical settings:
◦ Encourages continuity of medical care
◦ Encourages relationship building
◦ Legitimizes opioid use disorder as a treatable, chronic illness

Treatment duration (days)
Rem
ain
ing in t
reatm
ent
(nr)
0
5
10
15
20
0 50 100 150 200 250 300 350
Bup 6 day detox
Bup Maintenance
4 deaths
0 deaths
Kakko J, Lancet 2003

Opioid Dependence Treatment
in Primary Care
Stein, JGIM 2005
At 24 weeks, 59% remained
in treatment

Buprenorphine Diversion
Cicero, NEJM 2005
OXYCODONE
METHADONE
BUPRENORPHINE

All patients initiated on buprenorphine August
2003 through September 2007
Visits 15 minutes; frequency at discretion of
provider; non-witnessed urines checked for
temperature

Co-morbidities- Heptatitis C-49%; psychiatric
disorders 49%; HIV 14%; chronic pain 18%
Outcomes-
At the end of one year- 145 patients (57%) were
still receiving buprenorphine treatment
Overall 65% of month-long treatment blocks
were opioid negative

Treatment success higher for non-heroin users; all other demographic variables not significantly different
Non-retained patients (109)- 63 lost to f/u; 10 lost insurance; 21 discontinued- 8 transferred to methadone maintenance; 2 had adverse effect; 5 deaths – 3 overdose (none on buprenorphine at time of death); 1 AIDS; 1 cerebral hemorrhage.

Characteristic BUP METH P value
Mean Age 39.7 39.5 0.83
Female 44% 58% 0.001
Insurance
Commercial 41% 1% <0.001
Medicare 20% 3% <0.001
Medicaid 35% 56% <0.001
None 3% 39% <0.001
Employment
Employed 45% 13% <0.001
Unemployed 29% 72% <0.001
Disabled 26% 16% <0.001
65

Characteristic BUP METH P value
Abused Substances
Heroin 83% 86% 0.39
Opioid Rx 29% 9% <0.001
Cocaine 53% 55% 0.73
Benzodiazepines 9% 23% <0.001
Injection drug use 61% 69% 0.051
HIV infection 14% 8% 0.023
Chronic pain 18% 12% 0.063
Recent criminal charges 43% 50% 0.129
66


Maryland Medicaid-Priority Partners MCO 5/1/08-
4/30/11
Buprenorphine n=1292- avg age 35.8, 66%F,61%
White; 36% Baltimore City; 32% rural
Methadone n=2732- avg age 39.0, 69%F, 55%
White, 52% Baltimore City, 11% rural
Both agonists n=348- avg age 36.2, 70%F, 54%
White; 50% Baltimore City, 14% rural


Maryland Medicaid Priority Partners beneficiaries who received a script for buprenorphine between 1/1/08 and 7/31/12and no buprenorphine script in previous 3 months
Only first episodes analyzed

CCP n=137
Non-CCP n=992
6 month retention
80.3% 59.2% p<.001
Any ED visit 12 months
63.5% 60.4% NS
Any acute hospital stay 12 months
15.3% 18.9% NS
Total cost 12 months mean
$10,785 $12,210 P<.001

Prescribing is the easy part
The conversation is the art of medicine (and the fun)


You- “The best thing you can do for yourself is stop drinking”
Person- “I don’t deserve the best, what else can I do?”



What have you done today to make the world a better place?
What have you done today to make today better than yesterday?
Give me an update for your fan club


My patient’s urine drug screen is positive for…
My patient’s urine drug screen is negative for buprenorphine
My patient misses an appointment
My patient asks for a refill early
My patient has an overdose

Work on weight loss
Work on smoking cessation
Work on increasing exercise
Treat hepatitis C
Get better diabetic control
Make sure HIV VL is suppressed
Control blood pressure
Update vaccines
Make sure health maintenance is up to date-PAP, colonoscopy

After 3 months - seen 7 times
On medication for hypertension; adherent with
HAART for HIV and viral load undetectable; had
PAP done. No ER visits.
Doing well on buprenorphine/naloxone. No back
pain. Urine drug screens all negative since the
first visit.
Mood/self-esteem much improved. Better
relationship with family. Working part-time.