Embed Size (px)
Citation preview
The skin in systemic
disease
The skin and internal
malignancy acne seen with some adrenal tumours
flushing in the carcinoid syndrome
jaundice with a bile duct carcinoma
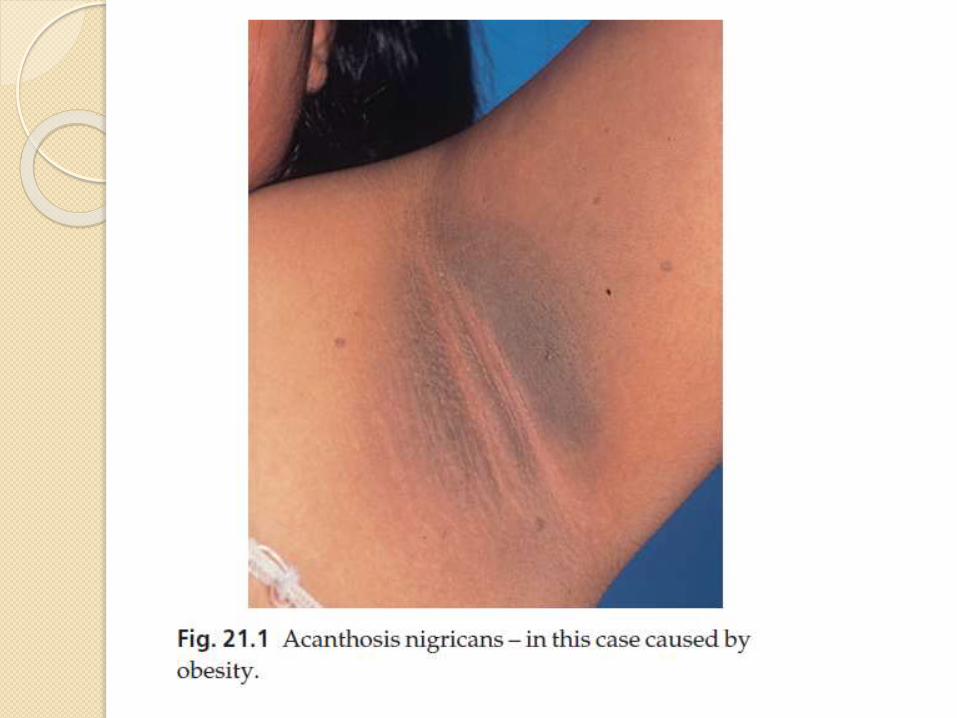
Acanthosis nigricans
is a velvety thickening and pigmentation of the major flexures
caused by:
obesity
metabolic syndrome (including type 2 diabetes with insulin resistance)
Drugs as nicotinic acid used to treat hyperlipidaemia
the chances are high that a malignant tumour is present, usually within the abdominal cavity.
Erythema gyratum repens
looks like the grain on wood
The skin and internal
malignancyAcquired hypertrichosis lanuginosa (‘malignant
down’)
is an excessive and widespread growth of fine lanugohair.
Necrolytic migratory erythema
is a figurate erythema with a moving crusted edge it signals the presence of a glucagonsecreting tumour of the pancreas.
Bazex syndrome
is a papulosquamous eruption of the fingers and toes, ears and nose, seen with some tumours of the upper respiratory tract.
Dermatomyositis, other than in childhood
About 30% of adult patients have an underlying malignancy. Pay special attention to the ovaries where ovarian cancer may lurk undetected.
The skin and internal
malignancyGeneralized pruritus
usually a lymphoma
Superficial thrombophlebitis.
the migratory type associated with carcinomas of the pancreas.
Acquired ichthyosis
especially lymphomas
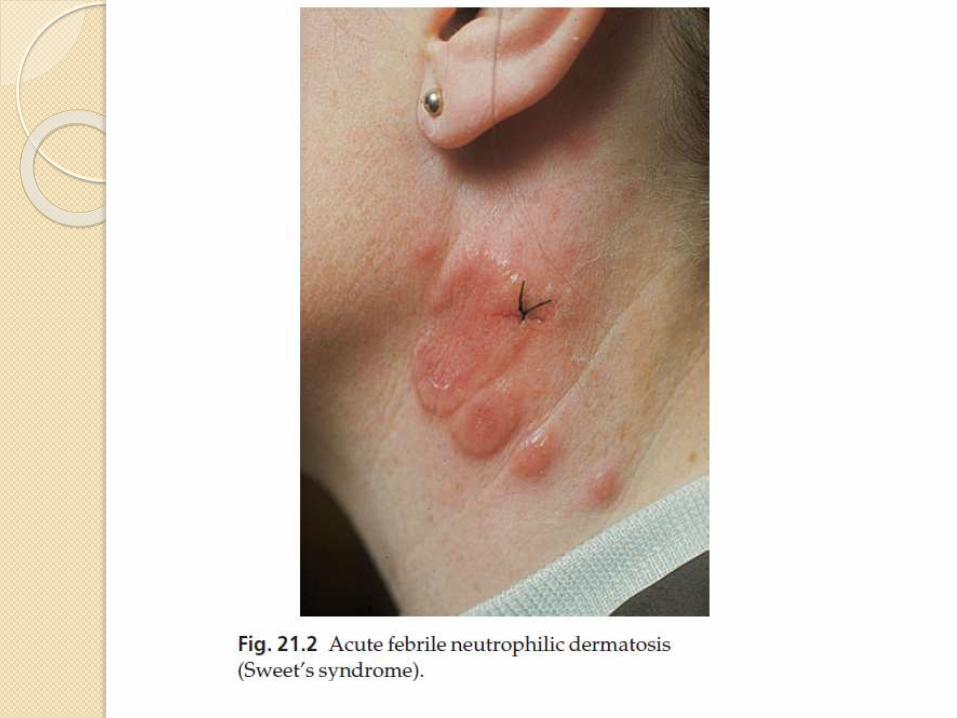
Acute febrile neutrophilic dermatosis (Sweet’s syndrome)
The classic triad found in association with the red oedematous plaques consists of fever, a raised erythrocyte sedimentation rate (ESR) and a raised blood neutrophil count. The most important internal association is with myeloproliferative disorders.
The skin and internal
malignancyParaneoplastic pemphigus
similar to pemphigus vulgaris but with
extensive and persistent mucosal
ulceration.
It is associated with myeloproliferative
malignancies as well as underlying
carcinomas.
Others. Pachydermoperiostosis
The skin and diabetes mellitus
Necrobiosis lipoidica.
Less than 3% of diabetics have necrobiosis, but 11–62% of patients with necrobiosis will have diabetes.
Non-diabetic necrobiosis patients should be screened for diabetes as some will have impaired glucose tolerance or diabetes, and some will become diabetic later.
The association is with both type 1 and type 2 diabetes.
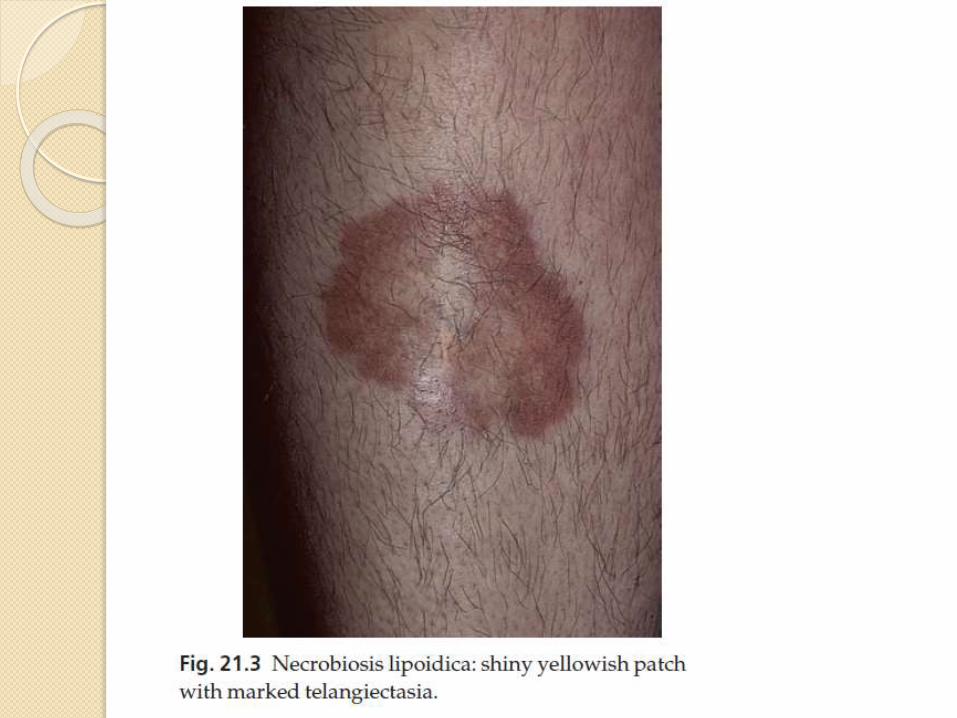
The lesions appear as one or more discolouredareas on the fronts of the shins
Early plaques are violaceous but atrophy as the inflammation goes on and are then shiny, atrophic and brown–red or slightly yellow.
The skin and diabetes
mellitus The underlying blood vessels are easily seen through
the atrophic skin and the margin may be erythematousor violet.
Minor knocks or biopsy can lead to slow-healing ulcers
Treatment
No treatment is reliably helpful, the atrophy is permanent
the best one can expect from medical treatments is halting of disease progression.
A strong topical corticosteroid applied to the edge of an enlarging lesion may halt its expansion.
There is little evidence that good control of the diabetes will help the necrobiosis.
The skin and diabetes
mellitusGranuloma annulare.
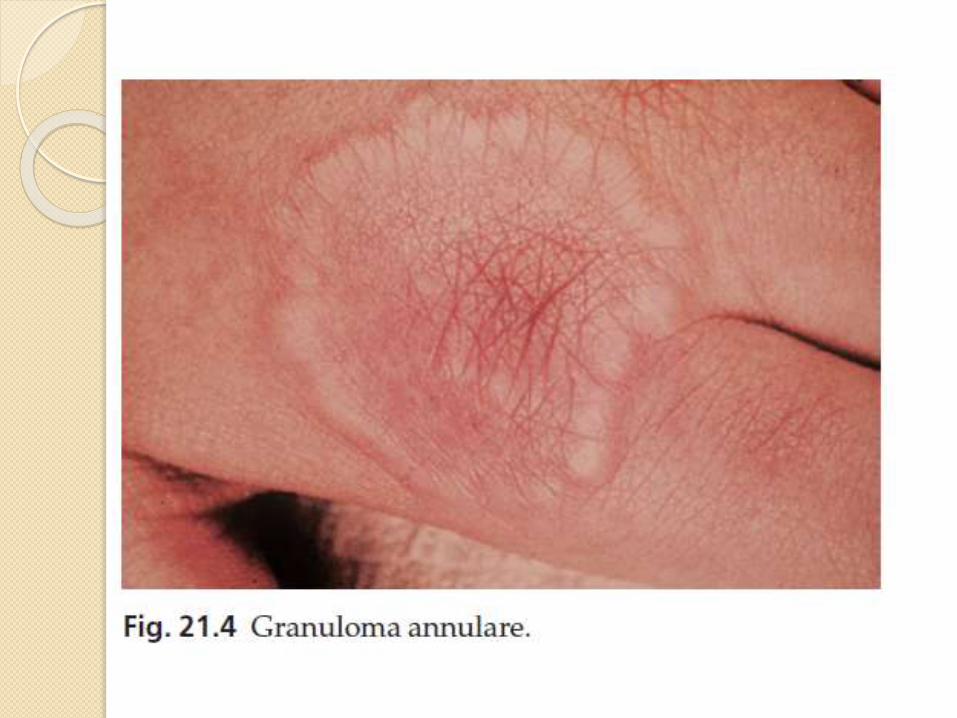
Clinically, the lesions of the common type of granulomaannulare often lie over the knuckles and are composed of dermal nodules fused into a rough ring shape
On the hands the lesions are skin-coloured or slightly pink; elsewhere a purple colour may be seen.
histology shows a diagnostic palisading granuloma
Lesions tend to go away over the course of a year or two.
Stubborn ones respond to intralesional triamcinoloneinjections.
Diabetic dermopathy
In about 50% of type 1 diabetics, multiple small (0.5–1 cm in diameter) slightly sunken brownish scars can be found on the limbs, most obviously over the shins.
The skin and diabetes
mellitusCandidal infections
Staphylococcal infections
Vitiligo
Eruptive xanthomas
Stiff thick skin (diabetic sclerodactyly or cheiroarthropathy)
on the fingers and hands, demonstrated by the ‘prayer sign’ in which the fingers and palms cannot be opposed properly
Atherosclerosis with ischaemia or gangrene of feet.
Neuropathic foot ulcers.
The skin in liver disease
Pruritus
This is related to obstructive jaundice and may precede it
Pigmentation
With bile pigments and sometimes melanin
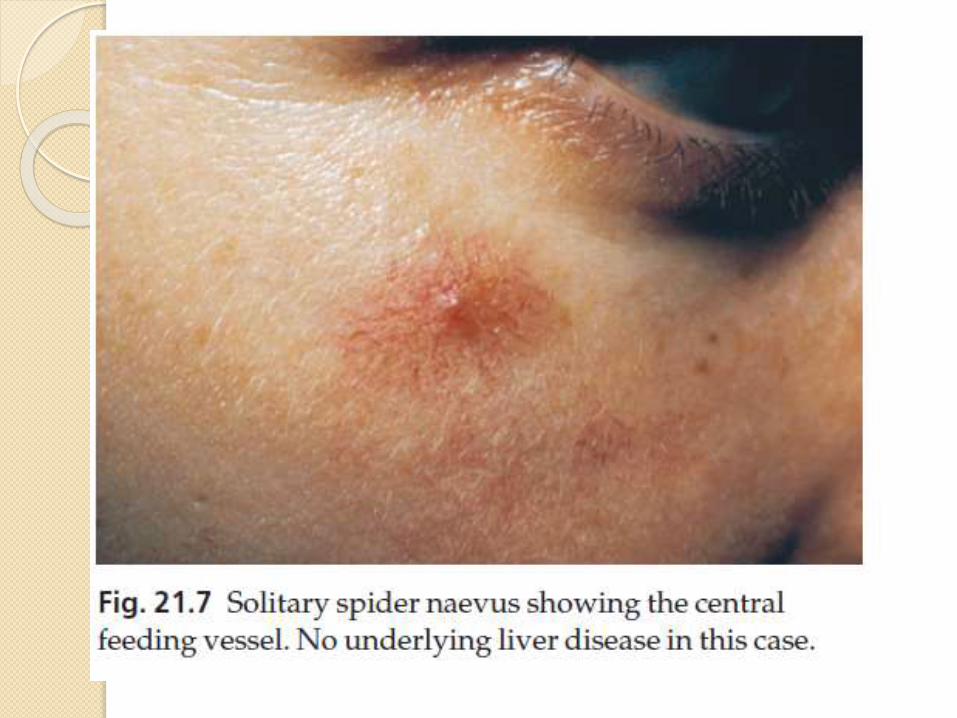
Spider naevi (These are often multiple in chronic liver disease
Palmar erythema
White nails
These associate with hypoalbuminaemia
The skin in liver disease
Lichen planus and cryoglobulinaemia with hepatitis C infection.
Polyarteritis nodosa with hepatitis B infection.
Porphyria cutanea tarda .
Xanthomas With primary biliarycirrhosis
Hair loss and generalized asteatoticeczema may occur in alcoholics with cirrhosis who have become zinc deficient.
The skin in renal disease
Pruritus and a generally dry skin.
Pigmentation A yellowish sallow colour and pallor from anaemia.
Half-and-half nail The proximal half is white and the distal half is pink or brownish.
Perforating disorders Small papules in which collagen or elastic fibres are being extruded through the epidermis.
Pseudoporphyria
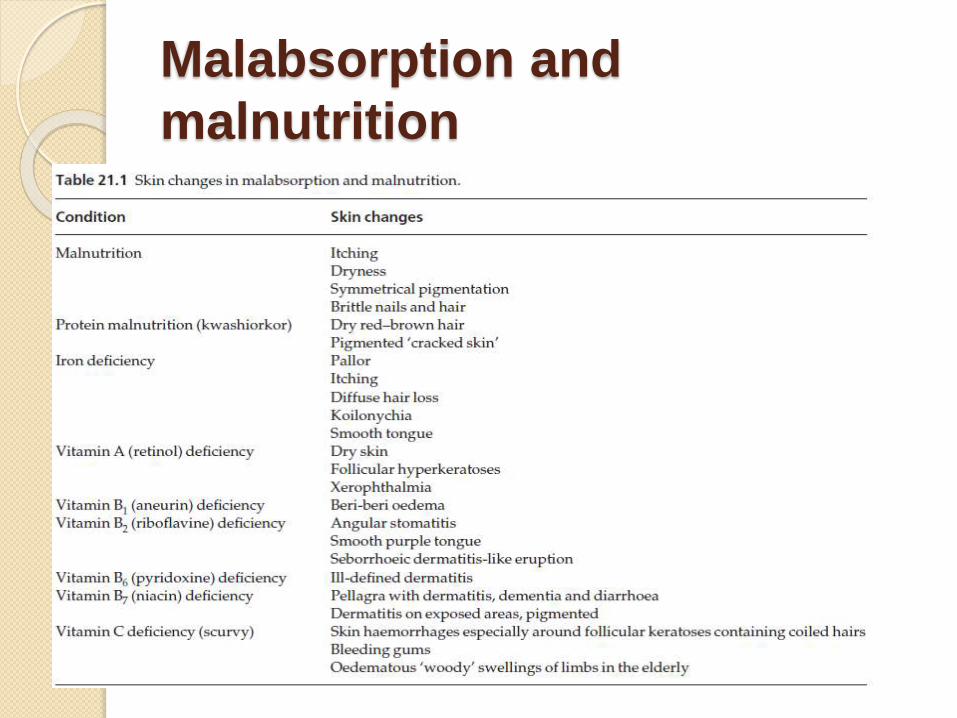
Malabsorption and
malnutrition
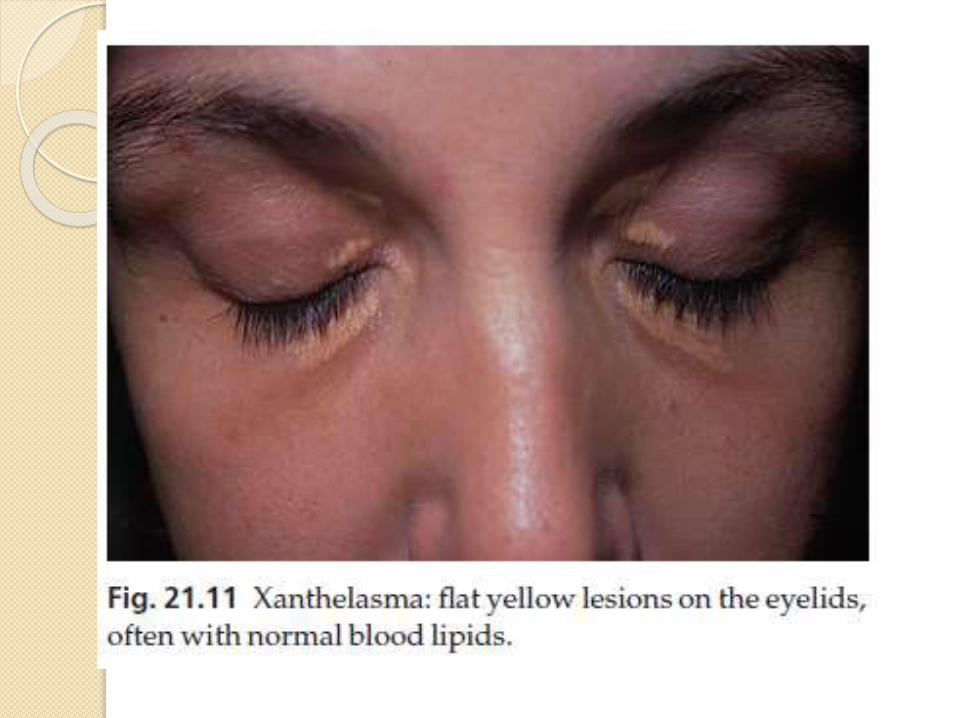
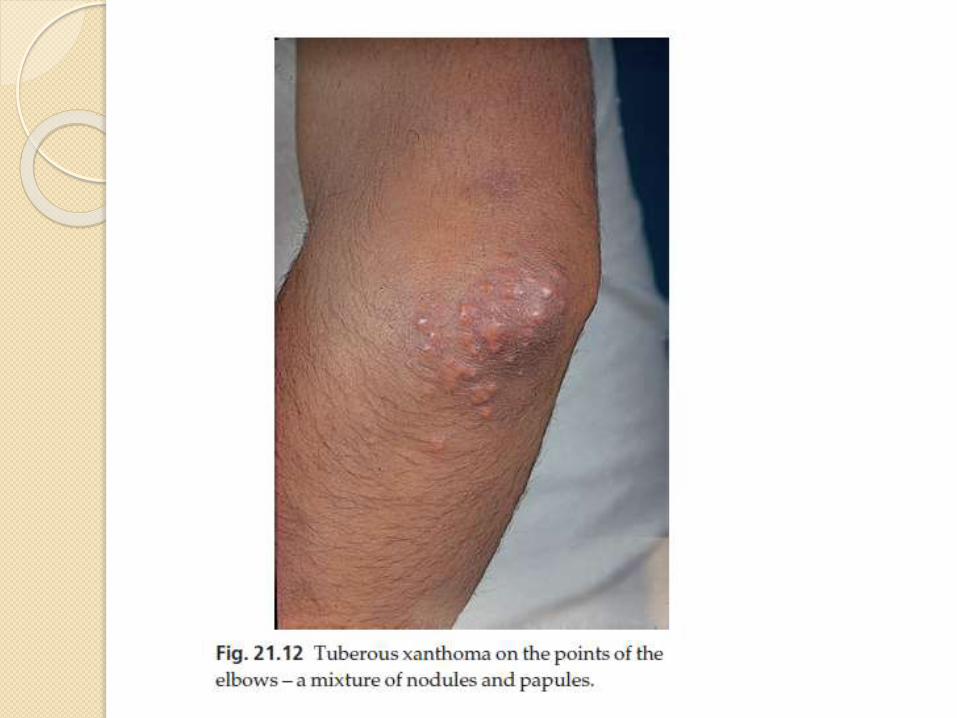
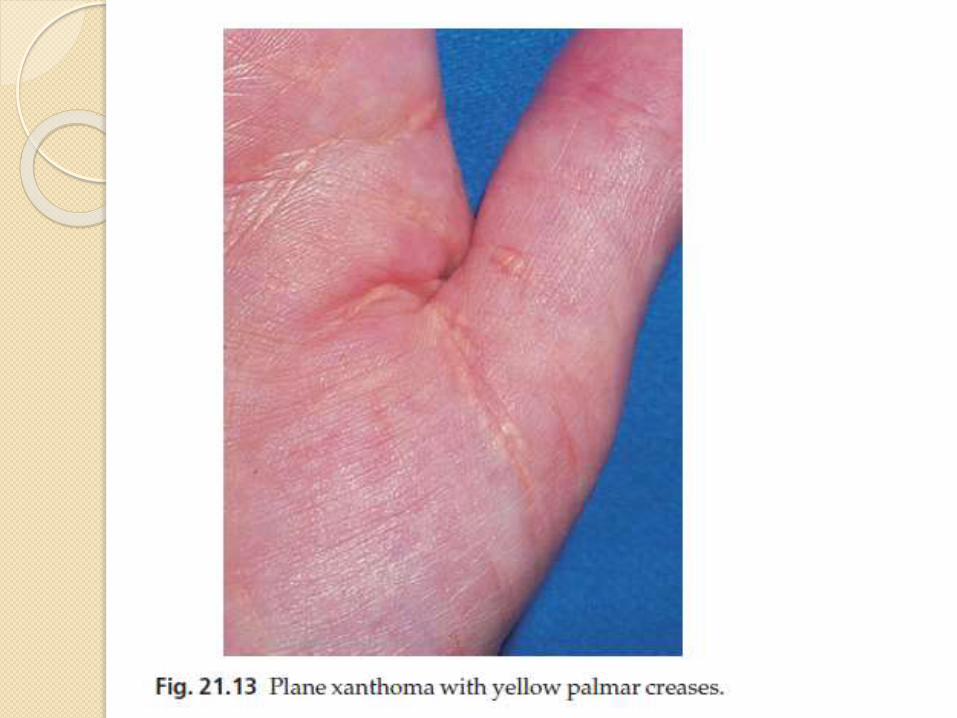
Xanthomas
Deposits of fatty material in the skin and subcutaneous tissues (xanthomas) may provide the first clue to important disorders of lipid metabolism.
Primary hyperlipidaemias are usually genetic.
Secondary hyperlipidaemia can be found in a variety of diseases including diabetes, primary biliary cirrhosis, the nephroticsyndrome and hypothyroidism.
Lipid-regulating drugs (e.g. statins and fibrates) not only stop xanthomas from appearing, but they also allow them to resolve.
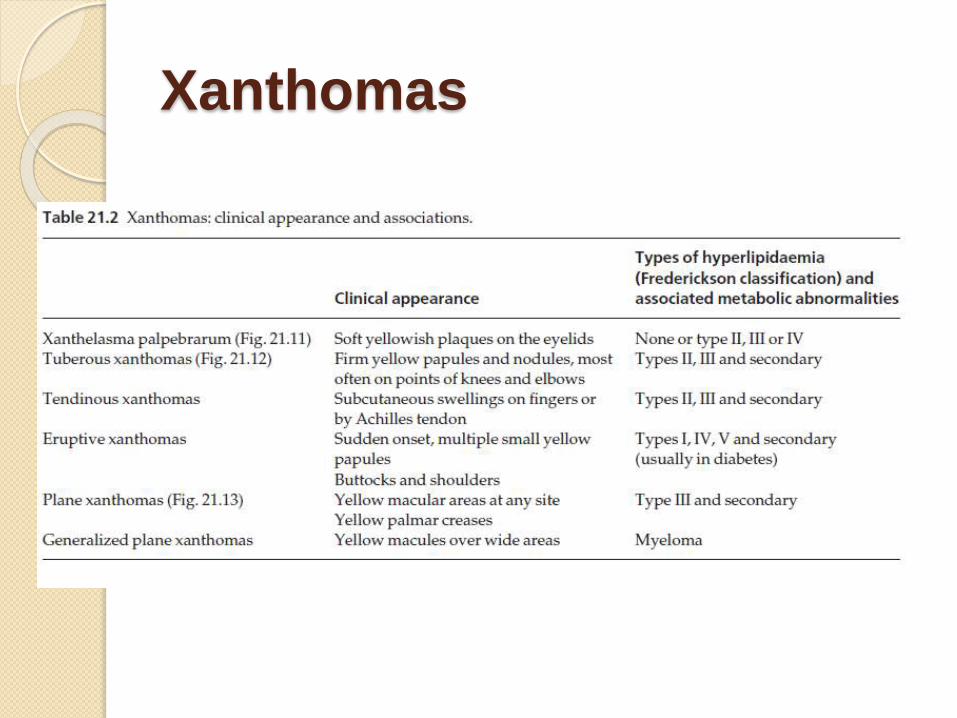
Xanthomas
Generalized pruritus
Pruritus is a symptom with many causes, but not a disease in its own right.
Itchy patients fall into two groups:
1. those whose pruritus is caused simply by surface causes (e.g. eczema, lichen planusand scabies)
2. those who may or may not have an internal cause for their itching. These patients require a
detailed physical examination, including a careful search for lymphadenopathy
Investigations including a full blood count, iron status, urea and electrolytes, liver function tests, thyroid function tests and a chest X-ray
Causes
Liver disease
Itching signals biliary obstruction.
It is an early symptom of primary biliary cirrhosis.
Colestyramine may help cholestatic pruritus, possibly by promoting the elimination of bile salts.
Other treatments include naltrexone, rifampicinand ultraviolet B.
Chronic renal failure
Ultraviolet B phototherapy, naltrexone or administration of oral activated charcoal may help.
Iron deficiency
Treatment with iron may help the itching.
Causes
Polycythaemia
The itching here is usually triggered by a hot bath; it has a curious pricking quality and lasts about an hour.
Thyroid disease
Itching and urticaria may occur in hyperthyroidism.
The dry skin of hypothyroidism may also be itchy.
Diabetes
Internal malignancy
The prevalence of itching in Hodgkin’s disease may be as high as 30%.
It may be unbearable, yet the skin often looks normal.
Pruritus may occur long before other manifestations of the disease.
Itching is uncommon in carcinomatosis.
Causes
Neurological disease
Paroxysmal pruritus has been recorded in multiple sclerosis and in neurofibromatosis.
Brain tumours infiltrating the floor of the fourth ventricle may cause a fierce persistent itching of the nostrils.
Diffuse scleroderma
may start as itching associated with increasing pigmentation and early signs of sclerosis.
Itching is usually severe
The skin of the elderly may itch because it is too dry, or because it is being irritated.
Pregnancy
Drugs
Treatment
Therapy is symptomatic and consists of sedative antihistamines
skin moisturizers, and the avoidance of rough clothing, overheating and vasodilatation, including that brought on by alcohol.
Ultraviolet B often helps all kinds of itching, including the itching associated with chronic renal and liver disease.
Local applications include calamine and mixtures containing small amounts of menthol or phenol
THE END
THANKS