Embed Size (px)
Citation preview


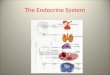
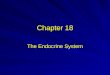
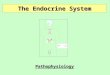
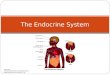
“Highly integrated and widely distributed
group of organs that provides homeostasis
among various tissues”
Signaling by Extracellular secreted
molecules:
Autocrine
Paracrine
Endocrine-Hormones
“Secretory molecules that act on target cells
distant from their site of synthesis”
Two types:
Interact with cell surface receptors
a) Peptide hormones i.e. Growth hormone and
insulin
b) Small molecules i.e. epinephrine
Interact with intracellular receptors
a) Lipd soluble hormones i.e. thyroxine

Bean-shaped structure at base of brain.
Connected to Hypothalamus through a stalk
called Infundibulum.
Two lobes:
Adenohypophysis
Neurohypophysis
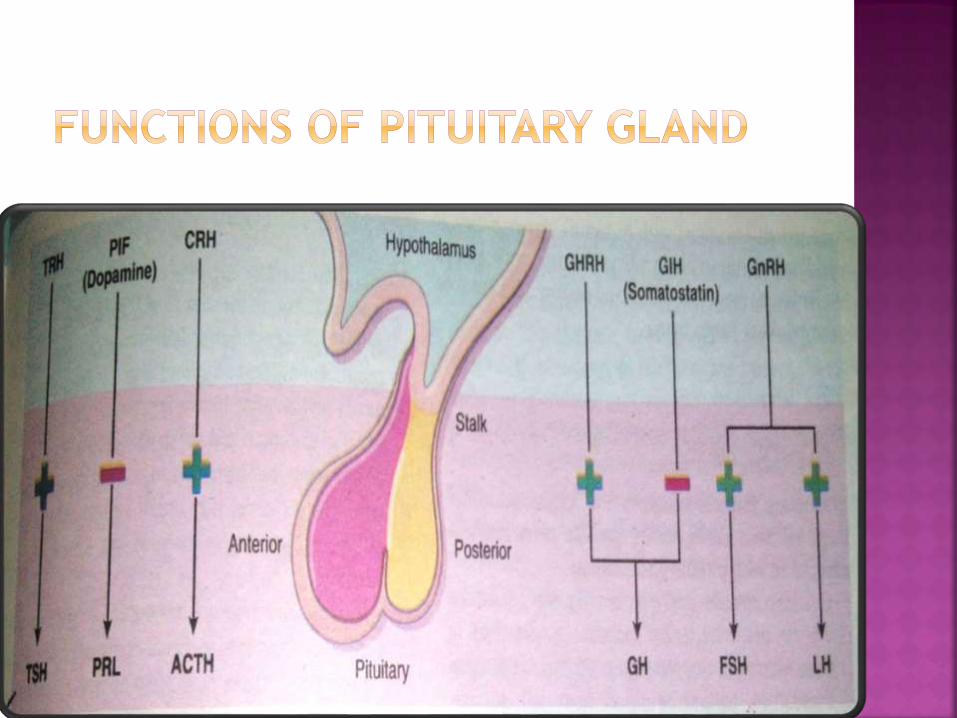
Release of trophic hormones is under
control of hypothalamic factors i.e either
stimulatory or inhibitory.
Hyperpituitarism
Excessive secretion of trophic hormone
Causes:
Anterior lobe pituitary adenoma
Hypopituitarism
Deficiency of trophic hormone
Causes:
Ischemic injury
Surgery or radiation
Inflammatory reactions

Two bulky lateral lobes connected by isthmus
Located below or anterior to larynx
Lobules composed of dispersed follicles
Follicles- cuboidal to low columnar
epithelium
Thyroglobulin- presursor protein of thyroid
hormone

Upregulation of carbohydrates and lipid
catabolism
Stimulation of protein synthesis in wide
variety of cells
Increase in basal metabolic rate
Hyperthyroidism:
Thyrotoxicosis due to elevated circulating
levels of free T3 and T4
GRAVES Disease – autoimmune disease
Autoantibodies to TSH receptor
Activate TSH receptors on thyroid epithelial
cells leads to hyperthyroidism
Hypertrophy and hyperplasia of follicles.
Ophthalmopathy

Sympathetic
overstimulation.
Accumulation of
loose connective
tissue behind
orbits
Inadequate levels of thyroid hormone.
Cretinism – infants
Iodine deficiency
Impaired development of skeletal system and
CNS
Goiter-impaired synthesis of thyroid
hormone
Compensatory rise in TSH
Enlargement of thyroid gland
Pancreatic cells – islets of langerans
Contain 4 cells
Alpha cell releasing glucagon
Beta cell releasing insulin
Delta cell releasing somatostatin
PP cells releasing VIP

Group of disorders with a common feature of
hyperlglycemia
Caused by deficient production or action of
insulin
Cause secondary damage to vital organs
Kidneys – end stage renal disease
Eyes – adult onset blindness
Nerves – non traumatic lower extremity
amputation
Blood vessels
Type I – IDDM (20%)
Type II – NIDDM (80-90%)
Monogenic forms i.e MODY– rare

Low level of glucose in body
High levels of glucose in body
Glucagon secretion
Insulin secretion


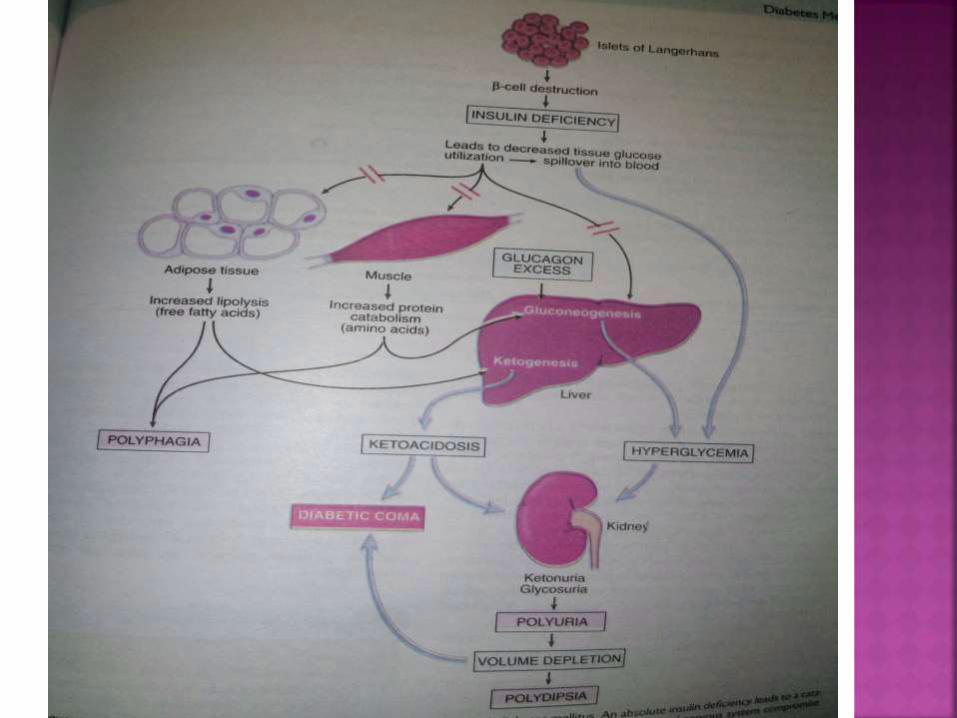
Type-1 diabetes mellitus
Production of autoantibodies against b cells of pancreas
No insulin production
Hyperglycaemia
Type-2 diabetes mellitus
Insulin production is sufficient
Cells involved in glucose metabolism become desensitized
Do not respond to insulin
Hyperglycaemia
Target tissue fails to response insulin
Decreased glucose uptake
Gluconeogenesis
Decreased glycolosis
Decreased fatty acid oxidation

Obesity - Increased body fat
OUTCOMES:
Insulin resistance
Diabetes
Cardiovascular diseases like hypertention and
hyperlipidemia

Excess free fatty acids
FFA in B cells – release of IL-1B and other pro
inflammatory cytokines – recruit
macrophages and T cells – B cell dysfunction
and insulin resistance
Adipokines release from adipocyte cause B
cell dysfunction as described above.
FFA and glucose in B cells – release of IL-1B
and other pro inflammatory cytokines –
recruit macrophages and T cells – further
cytokine production
Amylin or IAPP release IL-IB
Cause B cell dysfunction and hyperglycemia
Multifactorial but main cause is
hyperglycemia and glucose toxicity
3 pathways:
Formation of advanced glycation end
products (AGEs)
Activation of protein kinase C
Disturbances in polyol pathways
Diabetic nephropathy
Retinopathy
Hypertension
Peripheral neuropathy
Microangiopathy
Macrovascular disease
Myocardial infarction
Ketoacidosis
Diabetic coma
Hyperosmolar non-ketotic coma
Weakness
Polyuria
Polydipsia
Polyphagia
Ketoacidosis
Metabolic derangements
Glucose, fat and protein metabolism
Glycosuria
Osmotic diuresis
Proteolysis
Weightloss
Muscle weakness
Ketogenesis
Ketonemia
Ketonuria

Polyuria
Polydipsia
Obesity
Weakness
Weight loss
Hyperosmolar non-ketotic coma
Dehydration
Osmotic diuresis
Urinary fliud loss

Normal glucose level= 70-120mg/dl
Random glucose level >200 or =200mg/dl
Fasting glucose level >126 or =126mg/dl
OGTT – oral glucose tolerance test
>200mg/dl or =200mg/dl
Euglycemic fasting glucose level
<110mg/dl, OGTT<140mg/dl
Prediabetes fasting glucose level >110
but<126 mg/dl , OGTT>140 &<200 mg/dl
Glycaemic control- %age of glycosylated
hemoglobin (HbA1C)
HbA1C<7 = tight glycaemic control

Medical nutrition therapy
Oral hypoglycaemic therapy
Insulin therapy
First line of defense for type-2 diabetics
Adequate diet – low cholesterol intake
Excursive
1. Weight reduction
2. Improves insulin sensitivity
3. Lower blood glucose level
Metformin
Type-2 diabetes
Reduce hepatic glucose production
Sulphonylureas
Tolbutamide
Tolazamide
Increase insulin release
Pramlintide
Type-1 diabetes

Type-1 diabetes main treatment
Portable pen injectors
Subcutaneous injection
Insulin glargine……..
Blood glucose monitoring
Body weight monitoring
Personal hygeine
Healthy lifestyle
Reducing excessive salt intake
Paired organs having cortex and medulla
Synthesize
1. Glucocorticoids
2. Mineralocorticoids
3. Sex steroids
It can be :
Primary hypoadrenalism
1. Acute adrenocortical insufficiency
2. Chronic adrenocortical insufficiency
Secondary hypoadrenalism
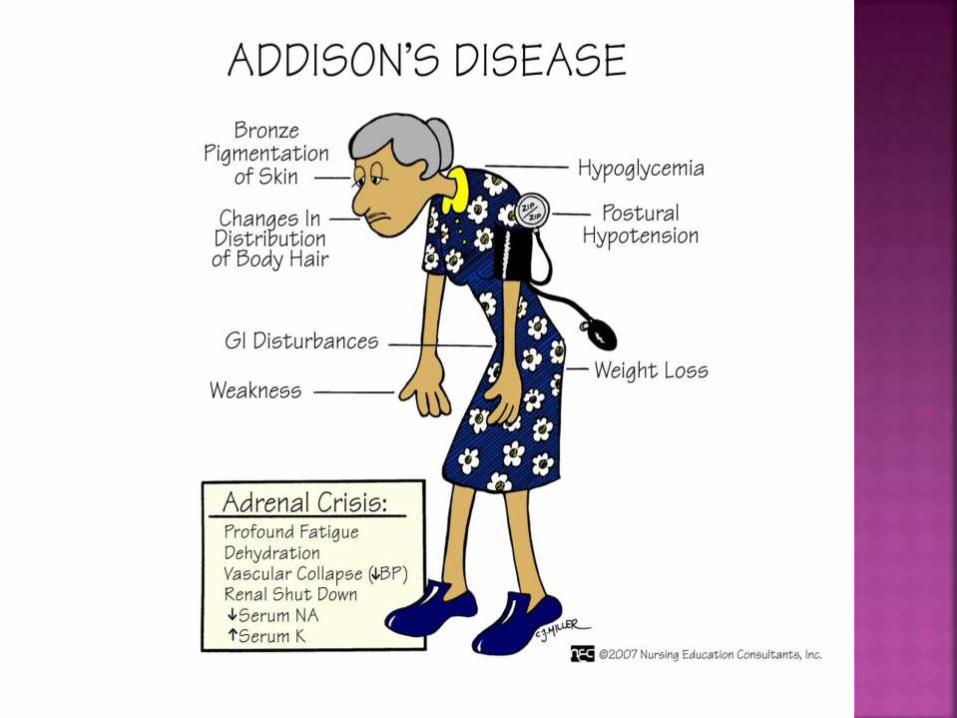
ADDISON DISEASE:
Adrenal cortex destruction
Causes
1. Autoimmune adrenalitis
2. Tuberculosis
3. AIDS
4. Fungal
5. Metastatic cancer
It includes:
Cushing syndrome
Hyperaldosteronism
Adrenogenital syndrome
Elevated glucocorticoid levels
Causes:
Exogenous glucocorticoids
Endogenous causes
-Primary hypothalamic-pituitary diseases associated with hypersecretion of ACTH
-Secretion of ectopic ACTH by non-pituitary neoplasm(tumor of thymus gland,
Small cell tumor of Lungs)
-Primary adrenocortical neoplasm (adenoma or carcinoma)
-Primary cortical hyperplasia

Small cell carcinoma of lungs
Hypertention
Weight gain
Truncal obesity-moon faces (Fat redistribution)
Buffalo hump(Fat mass at lower cervical and upper lumbar vertebra)
Atrophy
Weakness
Hyperglycemia
Glucosuria
Polydipsia (Excessive thirst)
Diabetes

When you do not succeed in taking giant steps on the road to your goal, be satisfied with little steps,
and wait patiently till the time that you are able to run, or better still, to fly.
Be satisfied to be a little bee in the hive who will soon become a big bee capable of making
honey…
Thank you …
47