Embed Size (px)
DESCRIPTION
2nd part
Citation preview

Substance Use Disorder
Addiction (DSM 5)
By
Soheir H. ElGhonemy
Assist. Professor of Psychiatry- Ain Shams University- Egypt
Member of International Society of Addiction Medicine
Member of European and American Psychiatric Associations
Trainer Approved by NCFLD


Dopamine Pathways
Functions
•reward (motivation)
•pleasure,euphoria
•motor function
(fine tuning)
•compulsion
•perserveration
•decision making
Serotonin Pathways
Functions
•mood
•memory
processing
•sleep
•cognition
nucleus
accumbens
hippocampus
striatum
frontal
cortex
substantia
nigra/VTA
raphe

Medial Forebrain Bundle
Ventral tegmental area (VTA)
(Lateral) hypothalamus (LH)
Nucleus accumbens (NAc)
Frontal cortex (FC) - key portions
Prefrontal cortex (pfc)
Orbitofrontal cortex (ofc)

Drugs Associated wth
Neurotransmitters
Why do people have “drugs of choice”?
Dopamine - amphets, cocaine, alcohol
Serotonin - LSD, alcohol
Endorphins - opioids, alcohol
GABA - benzos, alcohol
Glutamate -alcohol
Acetylcholine - nicotine, alcohol

A Brain Chemistry Disease!
Addicting drugs seem to “match” thetransmitter system that is not normal
A chronic, relapsing, medical disease
There are mild, moderate, and severe forms
Detox is traditionally the first step in thetotal treatment process
Methadone and nicotine maintenance isevidence that some people require achemical to overcome the non-normaltransmitter system

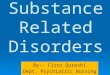
Figure 5

The combination of neuroadaptations in the braincircuitry for the three stages of the addiction cyclethat promote drug-seeking behavior in theaddicted state.
Activation of the ventral striatum/dorsalstriatum/extended amygdala driven by cuesthrough the hippocampus and basolateralamygdala and stress through the insula.
The frontal cortex system is compromised,producing deficits in executive function andcontributing to the incentive salience of drugscompared to natural reinforcers.
Dopamine systems are compromised, and brainstress systems such as CRF are activated toreset further the salience of drugs and drug-related stimuli in the context of an aversivedysphoric state


Common Underlying NeurobiologicalFactors Can Be
Neurochemical (imbalance of
neurotransmitters)
Structural/anatomical (same
regions and pathways)
Genetic (inherited factors that
compromise function)

Drug Disorder
Cocaine and Methamphetamine Schizophrenia, paranoia,
anhedonia, compulsive
behavior
Stimulants Anxiety, panic attacks, mania
and sleep disorders
LSD, Ecstasy & psychedelics Delusions and hallucinations
Alcohol, sedatives, sleepaids
& narcotics
Depression and mood
disturbances
PCP & Ketamine Antisocial behavuor

DRUG USE(Self-Medication)
STRESS
CRF
Anxiety
CRF
Anxiety
What Role Does Stress Play
In Initiating Drug Use?

Consequence: There is no “cure”…
To be successful, treatment is a Lifetime
Process
Science is helping to improve our
strategies and successes

History Taking

The history is the chronological story of the
patient’s life from birth to present
Personal data:
Name, age, sex, marital status, religion,
address, occupation, education.
n.b.; source of referral could be mentioned
here if the patient won’t cooperate

Personal History:
Birth and developmental milestones, family
atmosphere, school performance and general
conduct in school, educational achievement,
occupational history, sexual and marital history.
Attempt to correlate social problems with
evolving drug problems. Enquire about impact
of drug use on lifestyle.

Family History:
Brief vignette of father, mother and other
siblings should include age, occupation
and relation with the client. History of
psychiatric problems or problems
resulting from alcohol, drugs or nicotine.

Drug History:
This section should attempt to give a clear picture of
initiation of drug use accounting for each specific
drug. The evolution of drug use with the
development of personal and social problems as a
consequences of drug use.
Type, quantity, and route of use of each individual
drug. Alcohol consumption should be checked as a
routine part of drug history taking.

Drug use in the past 24 hr.:
Detailed and sensitive questioning around this will not
only provide data about drug use and drug
dependence but should give a clear picture of the
client’s lifestyle and daily stresses and strains.
Drug use in the past month:
Should try to draw a picture of drug use over the past
4 weeks.
History of abstinence:
Number of trials , how , duration of each and reason
for relapse.

Legal History:
Charges, convictions, imprisonments and
violent incidents.
Sexual and Marital History:
Sexual behavior and marital relation and if
extramarital relationships. Relation of sexual
or marital problems to drug use.
Occupational History:
Relationships of jobs and relations to drug
use. Current employment status.

Present life situation:
Family and social support. Non drug use
friends, leisure activities and
occupational prospects, financial status
and accommodations.

Mental state examination:
On admission:
Describe relevant features. Positive and
negative findings regarding both physical
and mental condition of the client. Focus
on physical signs of drug withdrawal, liver
diseases signs and any neurological
dysfunctions. Sites of injections and any
infections.

Mental state should include level of
consciousness, alertness and orientation and as
well as level of cooperativeness. Ability to give
history will provide data about their intelligence,
cognitive state and level of insight into their
condition.
General state of dress and grooming as well as
evidence of agitation, calmness or detachment
from problem should be checked.

Pattern of sleep, appetite, energy level,
mood state and suicidal ideations giving
data about special and general
psychological state.
Any delusions or hallucinations should
be considered and relation to client
intoxication or withdrawal states

Follow up setting is meant for better
elaboration of the client’s condition and
allow building rapport for setting
management plan.
A thorough history is the substrate for a
considered opinion about the client. What is
the best for the client. History is cornerstone
in the substance abuse field.

Patient with treatment program:
Substance is being used.
Recent regular use.
Psychiatric status.
Medical condition.
Social network.
Legal aspects.

Goals of treatment:
A.Help the individual to be drug
free( detoxification).
B.Help to maintain drug free state (
relapse prevention)
C.Long term Rehabilitation.

Classification of substance:
I. CNS depressants: Alcohol
Opiates
Sedative hypnotics
II.CNS stimulants: Amphetamines
Cocaine
III.CNS hallucinogens: Cannabis
LSD
Anticholinergics

Stimulation : Depression :a. Anxiety .
b. Insomnia.
c. Twitches.
d. Convulsions.
e. Hyperthermia.
f. Tachycardia.
g. Irritability.
h. Excitement.
i. Tremors.
j. Hypertension.
k. Tachypnea
a. Apathy.
b. Retardation.
c. Inattentive.
d. Stupor.
e. Hypotension.
f. Bradypnea.
g. Ataxia.
h. Lethargy.
i. Drowsiness.
j. Confusion.
k. Hypothermia
l. Bradycardia &Coma.

Drugs of abuse that can be tested in urine:
Alcohol: 7-12 hrs.
Amphetamine : 48 hrs.
Barbiturate ; short: 24 hrs. , long acting: 3 wks.
Benzodiazepine: 3 days.
Cannabinoides : 3 days ---4 wks “ depending on the use; chronic use leads to lengthening of period”
Cocaine : 6- 8 hrs.
Codeine : 48 hrs.
Heroin : 36—72 hrs.
Methadone : 3 days.
Morphine : 48 – 72 hrs

The Neuropharmacology of Drugs of
Abuse
Psychoactive drugs alter normal neurochemical
processes . This can occur at any level of activity
including :
a. mimicking the action of a neurotransmitter .
b. altering the activity of a receptor .
c. acting on the activation of second messengers
d. directly affecting intracellular processes that control
normal neuron functioning.

Routes of administration:
It affects how quickly a drug reaches the
brain ,also ,chemical structure of a drug
plays an important role in the ability of a drug
to cross from the circulatory system into the
brain.
Four routes:
oral.nasal.Intravenous.inhalation.

alcoholMild and moderate intoxication:
1.Impaired attention , poor motor coordination.
2.Dystharthria- ataxia , nystagmus, slurredspeech.
3.Prolonged reaction time, flushed faceorthostatic hypotension.
4.Hematemesis and stupor.
Pathological intoxication:
1.Excited , psychotic state following min.consumption in susceptible individuals.
Intoxication associated with belligerence.

Uncomplicated Withdrawal:
Coarse tremors of hands, tongue, eyelids andat least one of the following:
Nausea or vomiting.
Malaise or weakness.
Autonomic hyperactivity.
Anxiety, Depressed mood or irritability.
Transient hallucination or illusions.
Headache , insomnia.
Withdrawal complication:
Seizures.
Hallucination.
Delirium.

Management:
I. Avoid aspiration by placing patient’s face down or on one
side. Hospitalization is usually necessary.
II. Parenteral sedatives or physical restrains.
III. Low dose sedative ; Lorazepam 1-2 mg, physical
restrains or further sedation by Haloperidol IM 5 mg.
IV. Parenteral dose of Thiamine 100 mg.
V. Benzodiazepine tapering.
VI. Thiamine 50 mg PO.
VII. Multivitamin PO.
VIII.Folate 1 mg PO.
Over a week for uncomplicated withdrawal.

Opiate:Patients rarely seek treatment for intoxication.
Overdose :
I. Respiratory and CNS depression.
II. Depression.
III.Gastric hypomotility with ileus.
IV. Non-cardiogenic pulmonary edema.
Withdrawal:
I. Lacrimation, rhinorrhea.
II. Diaphoresis, yawing, sneezing.
III. Malaise, irritability, nausea and vomiting.
IV. Diarrhea, myalgia, arthralgia, bone ache.

Management of Opiate overdose:
I. Respiratory depression : air way support
II. Cardiopulmonary suppression: NaloxoneHydrochloride 0.4 mg or 0.01 mg\ kg IV,repeated dose of Naloxone infusion0.4 mg\ hr. for 12 hrs. subsequent to theinitial boluses.
III. Pulmonary edema : Intubation and pressureventilation ;ICU admission.
IV. Gastric lavage or induced emesis followedby activated Charcoal for orally ingestedoverdose.