Embed Size (px)
Citation preview
SIROLIMUS THERAPY IN INFANTS WITH SEVERE HYPERINSULINEMIC HYPOGLYCEMIA:
TH E NEW ENGLAND JOURNAL O F MEDICINEPUBLISHED ON MARCH 20, 2014
THE CAUSES OF HYPOGLYCEMIA IN INFANTS: Hyperinsulinism. Ketotic hypoglycemia. Hormone deficiency. Glycogen storage disease. Disorder of gluconeogenesis. Defect in fatty acid oxidation. Nonpancreatic tumor hypoglycemia. Late dumping(alimentary hypoglycemia). Reactive hypoglycemia.
synonyms:
PHHI (Persistent hyperinsulinemic hypoglycemia in infants)
Familial hyperinsulinemiaCongenital hyperinsulinemia Primary islet cell hypertrophy(nesidioblastosis)
Histology: Two types:
1.Focal adenomatous hyperplasia
2.Diffuse abnormality
PATHOGENESIS: Genetic bases can be identified in about 50% of
cases. Discovered at least 8 genes: ABCC8 gene (ATP-binding cassette, subfamily C,
member 8), which encodes the SUR1 subunit of the KATP channel
●KCNJ11 gene, which encodes the Kir6.2 subunit of the KATP channel
●GLUD1 gene (glutamate dehydrogenase) ●GCK gene (glucokinase) ●HADH gene (3-hydroxyacyl CoA dehydrogenase
gene) ●HNF1A gene (hepatocyte nuclear factor 1-alpha) ●HNF4A gene (hepatocyte nuclear factor 4-alpha) ●SLC16A1 gene (solute carrier family 16, member 1) ●UCP2 gene (uncoupling protein 2
ABCC8 and KCNJ11 are the most common gene to be affected and are responsible for encoding K+ ATP dependent channel :
The ATP-sensitive potassium channel (KATP channel) regulates the release of insulin from pancreatic beta cells. Inactivating mutations in either of these genes reduce the number of open KATP channels, resulting in depolarization of the beta cells and persistent hypersecretion of insulin .There is some evidence that these mutations also lead to constitutive activation of the mTOR pathway which promotes beta cell proliferation . It provides a mechanistic basis for treatment of PHHI with the mTOR inhibitor, sirolimus (rapamycin)
Paternal uniparental disomy — A form of PHHI
characterized by focal adenomatous islet cell hyperplasia can be caused by focal loss of the maternal allele and replacement with the paternal allele (paternal disomy) from chromosome 11p15 can lead to a clone of B-cells which can develop into a focal lesion in the pancreas . If patients who have lost the maternal allele also harbor a paternally inherited mutation in ABCC8 or KCNJ11 gene. the resulting hemi- or homozygosity of the abnormal paternal gene leads to somatic recessive beta cell hyperplasia and hyperinsulinemia in the focal lesions
Epidemiology: An estimated incidence of 1 in 50,000 live births in a random-mating US population
M to F is 1,3:1
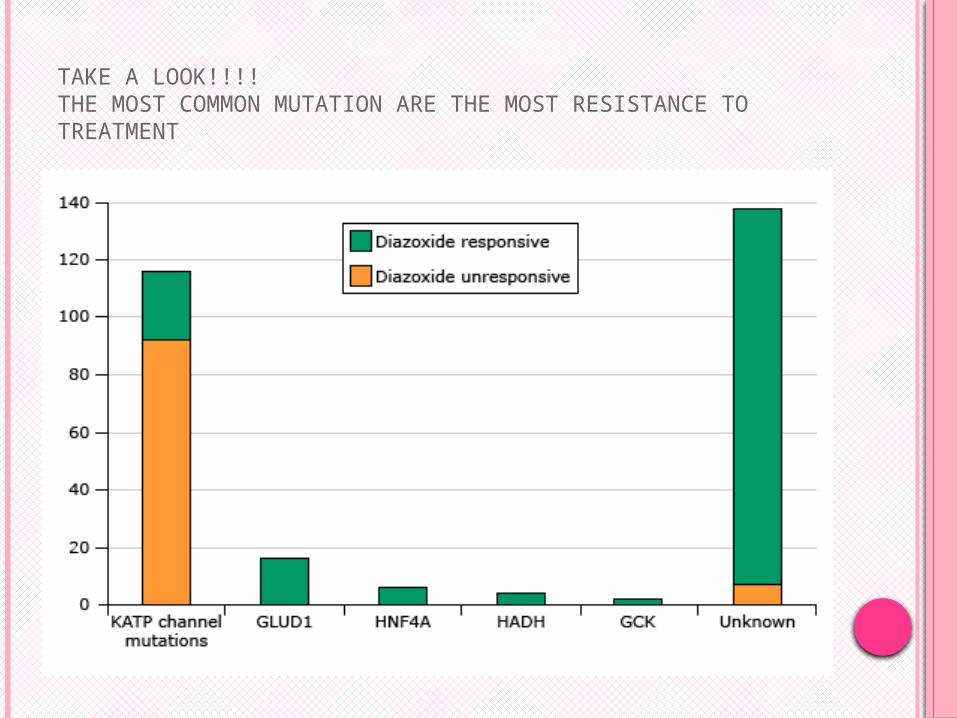
TAKE A LOOK!!!!THE MOST COMMON MUTATION ARE THE MOST RESISTANCE TO TREATMENT
CLINICAL MANIFESTATION:
macrosomia (large for gestational age) seen in one-third of neonates with PHHI, caused by inappropriate hyperinsulinemia
Most infants with PHHI have SYMPTOMS OF HYPOGLYCEMIA (eg, poor feeding, lethargy, jitteriness, and hypotonia) within the first few hours to days of life.
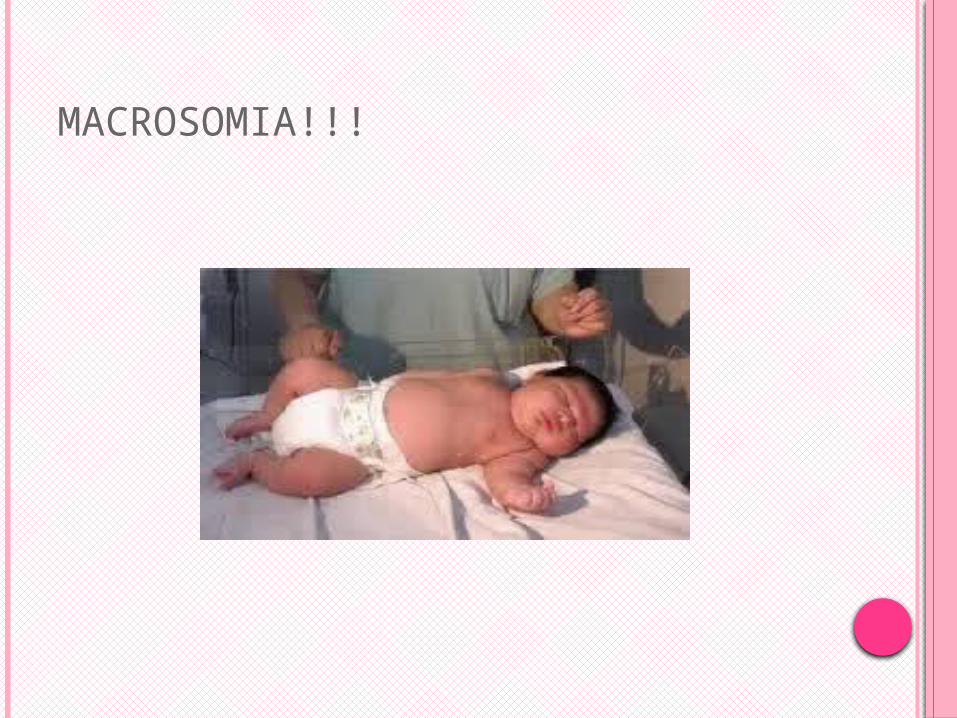
MACROSOMIA!!!
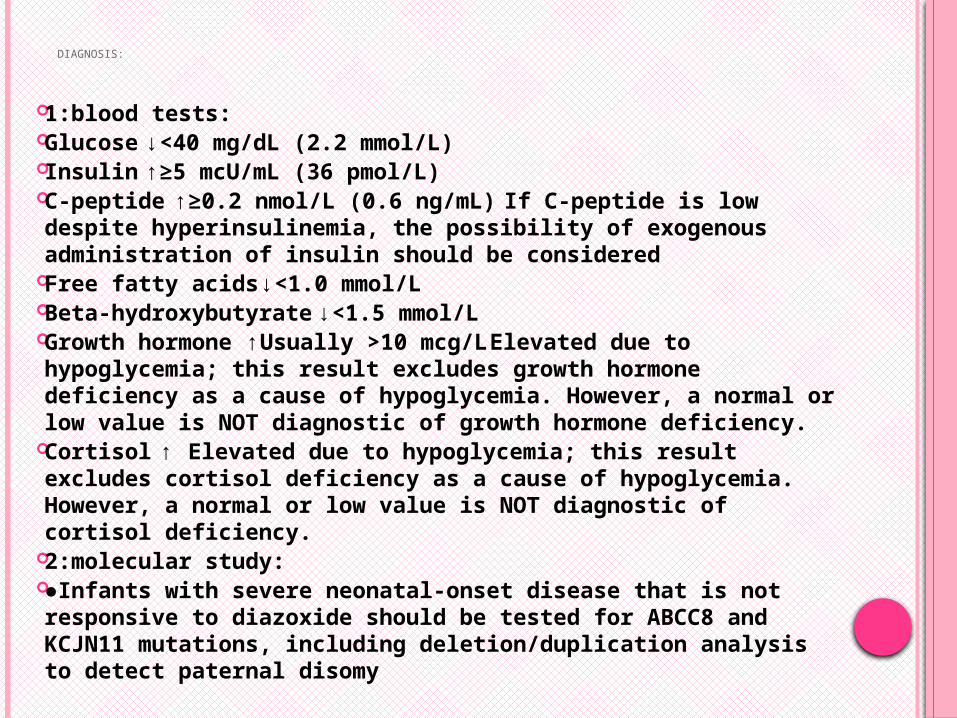
DIAGNOSIS:
1:blood tests: Glucose ↓ <40 mg/dL (2.2 mmol/L) Insulin↑ ≥5 mcU/mL (36 pmol/L) C-peptide ↑ ≥0.2 nmol/L (0.6 ng/mL) If C-peptide is low
despite hyperinsulinemia, the possibility of exogenous administration of insulin should be considered
Free fatty acids ↓ <1.0 mmol/L Beta-hydroxybutyrate ↓ <1.5 mmol/L Growth hormone ↑ Usually >10 mcg/L Elevated due to
hypoglycemia; this result excludes growth hormone deficiency as a cause of hypoglycemia. However, a normal or low value is NOT diagnostic of growth hormone deficiency.
Cortisol ↑ Elevated due to hypoglycemia; this result excludes cortisol deficiency as a cause of hypoglycemia. However, a normal or low value is NOT diagnostic of cortisol deficiency.
2:molecular study: ●Infants with severe neonatal-onset disease that is not
responsive to diazoxide should be tested for ABCC8 and KCJN11 mutations, including deletion/duplication analysis to detect paternal disomy
3.FOCAL VS DIFFUSE:
Several tests have been used preoperatively to help differentiate focal from diffuse disease. These include pancreatic arterial calcium stimulation (PACS) of insulin secretion, percutaneous transhepatic pancreatic venous sampling (PVS) of insulin [73], and, most recently, 18F-DOPA positron emission tomography (PET).
Why ????? Because the focal disease responds well to
partial pancreatectomy.
TREATMENT:1.HYPOGLYCEMIA
Intravenous therapy — Parenteral glucose usually is required to maintain the plasma glucose concentrations in a normal range (80 to 130 mg/dl or 4.4 to 7.0 mmol/l)
Dietary therapy — Dietary therapy consisting of frequent and consistent feedings in infants may be helpful to reduce the frequency and severity of hypoglycemic
2.HYPERINSULINEMIA:
1.Diazoxide — Diazoxide is the first-line therapy. It works by blocking the sulfonylurea receptors on the beta cells, resulting in opening of the KATP channels, and decreasing insulin release. Diazoxide is administered in doses of 5 to 15 mg/kg per day divided into three doses.
if a child does not respond at 15 mg/kg per day, he or she will not respond at ≥20 mg/kg per day, and increasing the dose only increases the risks of medication-related complications. Defining a clear clinical response in this situation frequently is difficult. If no clear response is observed within 48 hours of the initiation of a dose, diazoxide will probably not be effective
The most common side effects include hypertrichosis and sodium and water retention. Other side effects include advanced bone age, mild hyperuricemia .
2.octreotide:The second line therapy if diazoxide is unsuccessful
WHY IS THERE THE NEED FOR THE NEW TREATMENT???
The most common mutations in ABCC8 and KCNJ11 are associated with severe hyperinsulinemic hypoglycemia that is unresponsive to medical treatment with diazoxide and octreotide.
The only treatment option currently available for patients with medically unresponsive forms of diffuse hyperinsulinemic hypoglycemia is a subtotal pancreatectomy
However, some patients who have undergone surgery continue to have recurrent hyperinsulinemic hypoglycemia, whereas diabetes mellitus and exocrine pancreatic insufficiency develop in others.
ON A BASIS: A possible mechanism of hyperinsulinism and beta-cell
hyperplasia in diffuse hyperinsulinemic hypoglycemia involves the constitutive activation of the mTOR pathway.
The use of the mTOR inhibitor sirolimus (formerly called rapamycin) in a patient with an insulinoma suggested a potential role for mTOR inhibitors in
both the reduction of beta-cell proliferation and the inhibition of insulin production.
therapy with everolimus, an mTOR kinase inhibitor, was reported to result in a clinically significant glycemic response and regression in tumor size in four patients with metastatic insulinoma
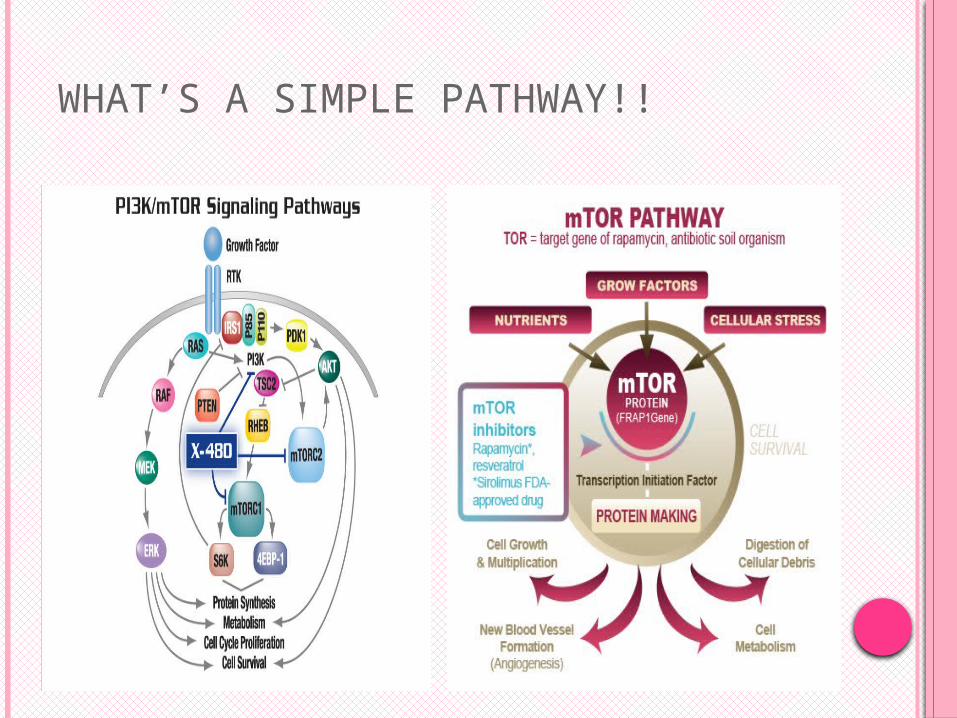
WHAT’S A SIMPLE PATHWAY!!
THE STUDY : HERE WE CAN START
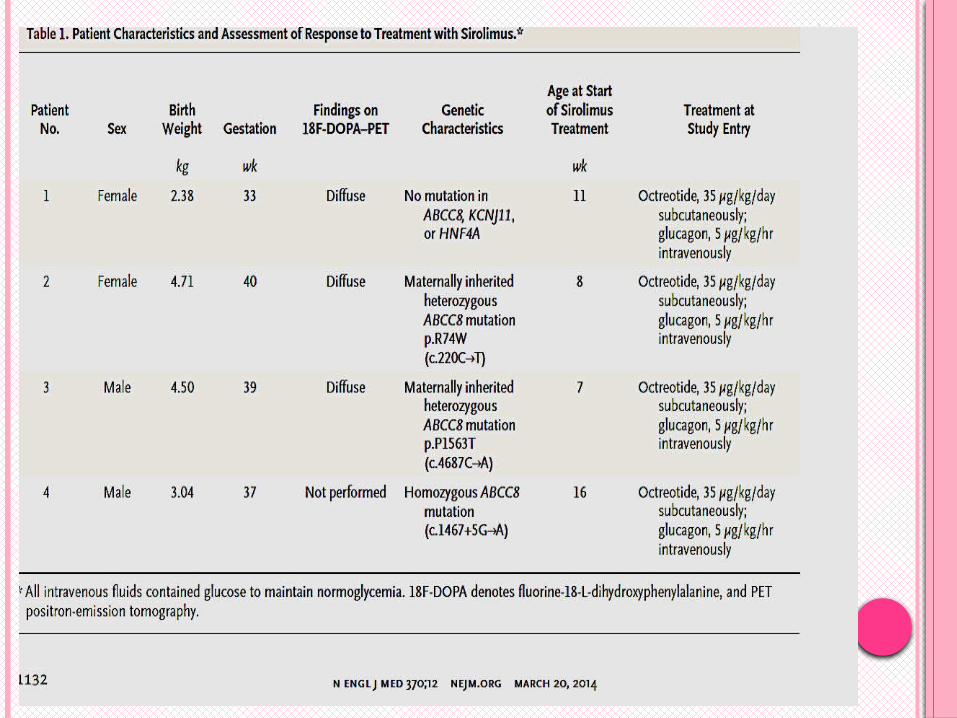
Methods: Four consecutive patients with severe hyperinsulinemic hypoglycemia that was unresponsive to maximal doses of diazoxide (20 mg per kilogram per day) and octreotide (35 μg per kilogram per day) were recruited to participate in the study.
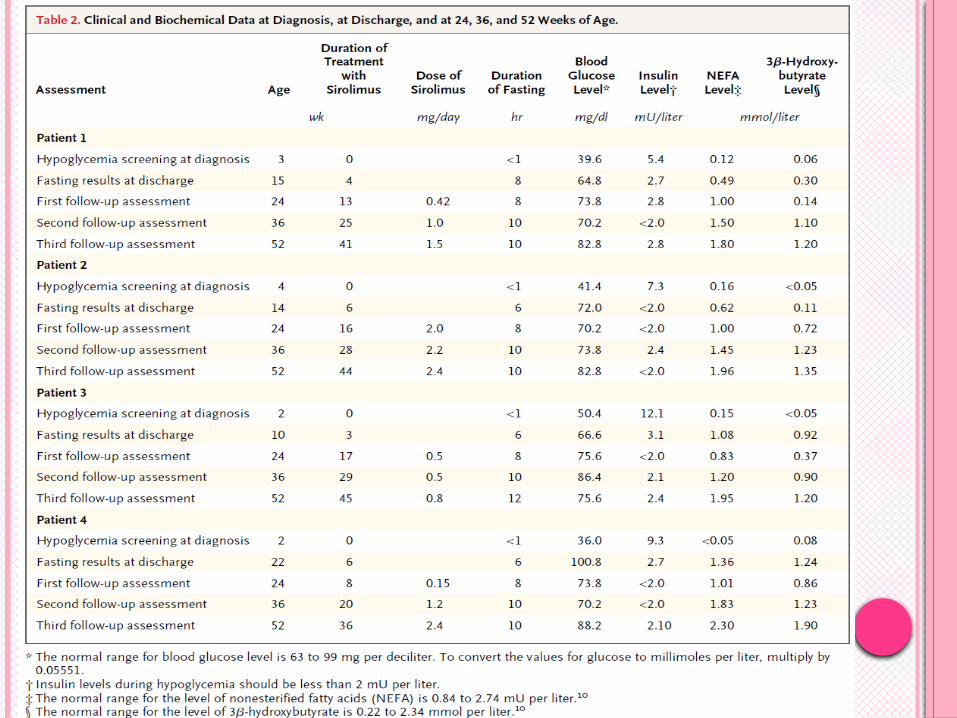
Look for next table
J
SO !!!
All the patients had severe symptomatic hypoglycemia (associated with seizures, poor feeding, and irritability) on day 1 of life in a local hospital, necessitating transfer to center for further care. A central venous catheter was inserted,
and high doses of dextrose and intravenous glucagon were administered to stabilize blood glucose levels at more than 63 mg per deciliter. Since there had not been a response to
maximal doses of diazoxide and octreotide in any of the four
patients, our standard protocol would have called for subtotal pancreatectomy for all of them. We therefore recruited these infants for the study.
AFTER A WRITTEN CONSENT FROM FAMILIES: Genetic tests were done to identified a possible
mutation. To confirm diffuse disease, scanning with
fluorine-18-L-dihydroxyphenylalanine (18F-DOPA)
positron-emission tomography (PET) was performed in three of the four patients. All the patients received sirolimus at an initial dose of
0.5 mg per square meter of body-surface area per day (in one or two doses). The dose was gradually increased with the goal of reaching aserum trough level of 5 to 15 ng per milliliter.The serum trough level of sirolimus was measure every 5 days. Once the desired serum drug level had been reached and blood glucose levelswere stable, intravenous glucose and glucagon infusions were gradually tapered. Regular monitoring was performed, including a complete blood count, measurement of serum lipid levels, and analysis of renal and liver function
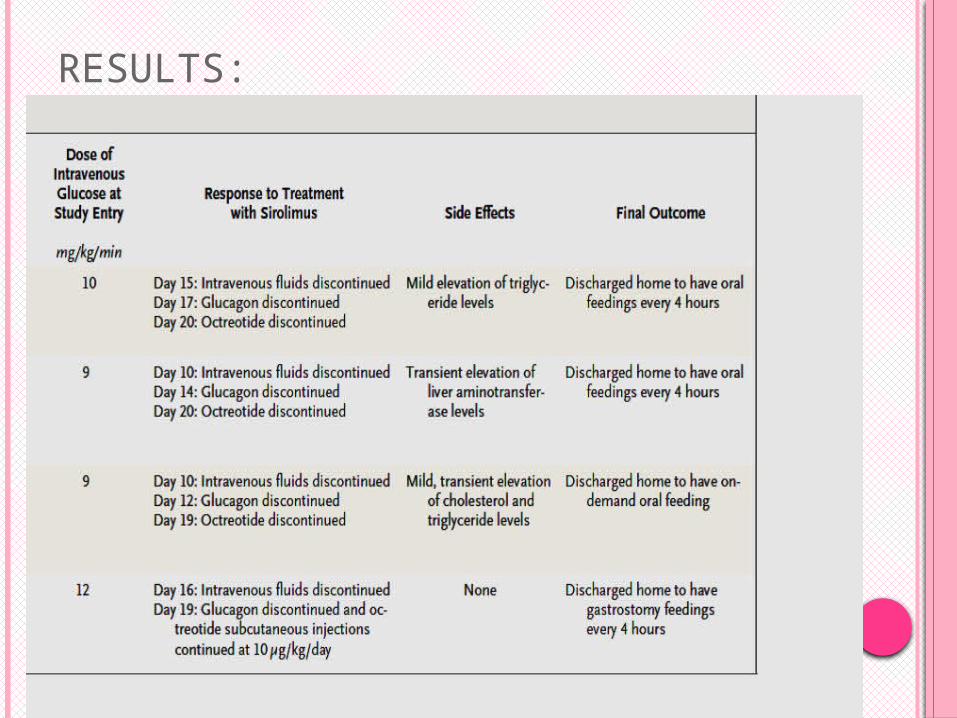
RESULTS:
RESPOND TO TREATMENT!! Over a period of 2 to 3 weeks,each infant
maintained stable blood glucose levels without the need for intravenous glucose infusion.Glucagon and octreotide infusions were then gradually discontinued, since blood glucose levels were stable at more than 63 mg per deciliter.Subsequently, all four infants were able to
receive all their nutrition enterally, and each continued to receive oral sirolimus therapy.The infants were also able to fast for 6 to 8 hours without the development of hypoglycemia. Each patient was discharged when enteral
feedings were established and the infant could fast for 6 to 8 hours without the development of hypoglycemia.
K Parents were instructed to monitor blood glucose levels at least three times a day before feeding. A review of the records of parental monitoring of blood glucose levels did not reveal any episode of hypoglycemia during treatment with sirolimus.
Follow-up assessments conducted until the infants reached 1 year of age indicated good glycemic control.
The side effects observed included transient elevation of aminotransferase levels, which resolved spontaneously, and mild elevation of triglyceride levels. The results of liver function studies have otherwise been normal. Neither sepsis nor any other serious infection developed in any of the infants.
A TRIAL:
Sirolimus was discontinued in one of the patients at 7 months of age; within 3 days, severe hypoglycemia developed, requiring intravenous infusion of glucose and subcutaneous administration of octreotide. Sirolimus was reinitiated, and during the next 3 to 4 weeks the glucose infusion and the octreotide were tapered and then discontinued.
J
AT THE END:
In summary, we report a therapeutic strategy in which we used mTOR inhibitors to treat patients with hyperinsulinemic hypoglycemia who otherwise would have required subtotal pancreatectomy.Treatment with mTOR inhibitors, alone or in combination with somatostatin analogues, may be a feasible option for selected patients with no contraindication, although the long term adverse effects and efficacy of such treatment require further study.
THAT IS THE
WAR!!!!!!!
THANK YOU FOR LISTENING
NAWAL MERJANEH………