Embed Size (px)
Citation preview

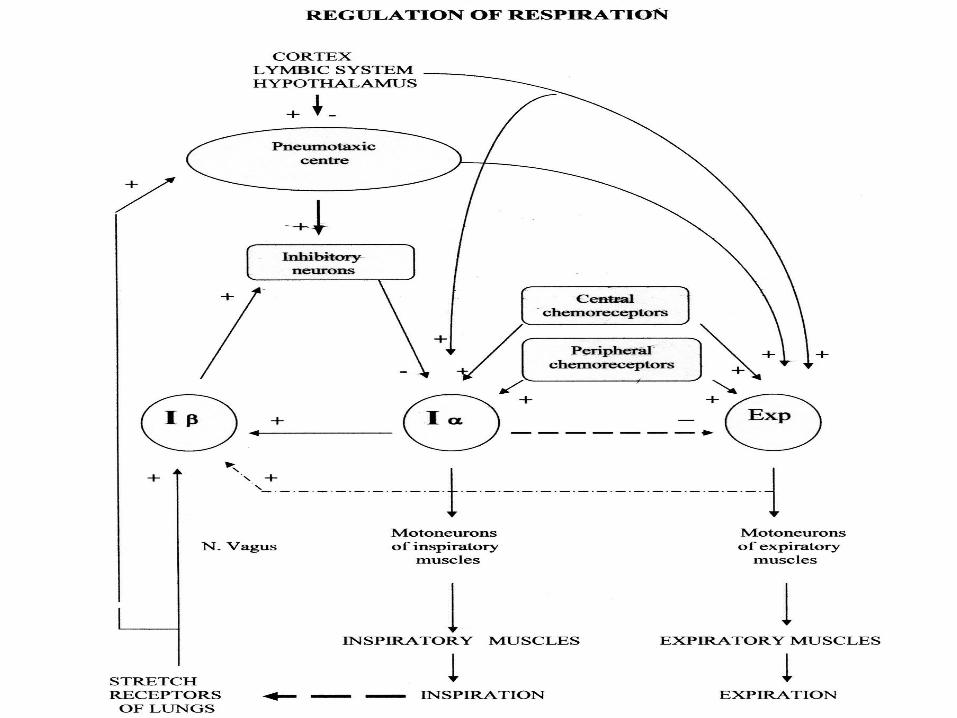
REGULATION OF RESPIRATION

2
What should I know well??

3
• Outstanding features of control of respiration
• Structure of respiratory center In the medullary RC, there are two types of neurons: 1 - inspiratory I neurons 2 - expiratory E neurons •Cause of rhythmicity
• Factors influencing respiratory center These are: 1 - peripheral reflexes, 2 - chemical control 3 - influences from the higher center
37

Outstanding features of control of respiration
1. Respiration occurs automatically
2. Respiratory movements are rhythmic
3. The respiratory excursions are finely regulated to the needs of the body
4. The cost benefit ratio of respiration, particularly at resting level, is small

AP of inspiratory & exspiratory neurons

Respiratory nuclei of the medulla
1. Dorsal respiratory nucleus2. Ventral respiratory nucleus
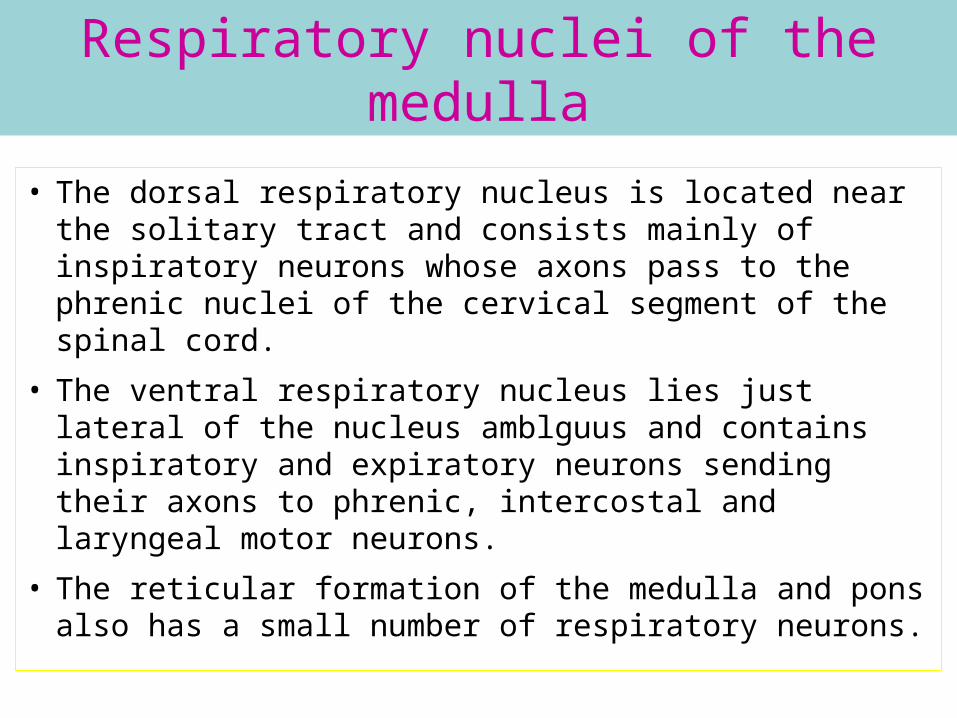
Respiratory nuclei of the medulla
• The dorsal respiratory nucleus is located near the solitary tract and consists mainly of inspiratory neurons whose axons pass to the phrenic nuclei of the cervical segment of the spinal cord.
• The ventral respiratory nucleus lies just lateral of the nucleus amblguus and contains inspiratory and expiratory neurons sending their axons to phrenic, intercostal and laryngeal motor neurons.
• The reticular formation of the medulla and pons also has a small number of respiratory neurons.

INHALATION
INSPIRATORY MUSCLES
MOTONEURONS OF INSPIRATORY MUSCLES
Iα
LSR
Iβ
Inh
PTC
N.vagus
Centr. chem.
Periph. chem
exp
EXSPIRATORY MUSCLES
MOTONEURONS OF EXSPIRATORY MUSCLES
ACTIVE EXHALATION

Cause of rhythmicity

FACTORS INFLUENCING RESPIRATORY CENTER
1. Peripheral reflexes
2. Chemical control
3. Influences from the higher center
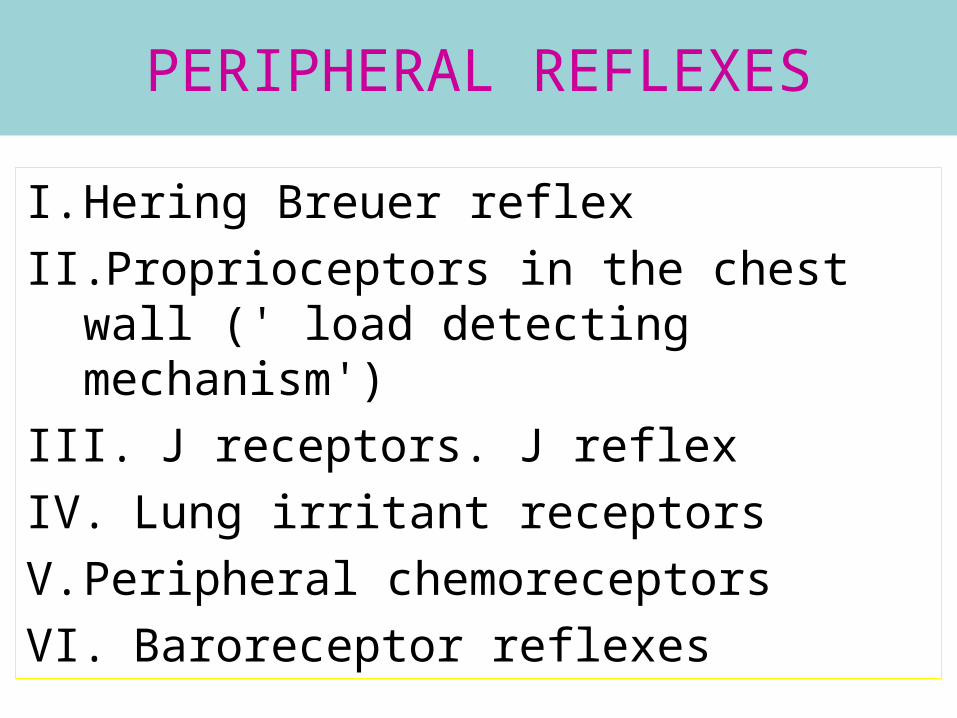
PERIPHERAL REFLEXES
I. Hering Breuer reflex
II. Proprioceptors in the chest wall (' load detecting mechanism')
III. J receptors. J reflex
IV. Lung irritant receptors
V. Peripheral chemoreceptors
VI. Baroreceptor reflexes

MECHANORECEPTORS of lungs & respiratory pathways (1000 receptors in each lung)
• HIGHTHRESHOLD – EXCITED IN DEEP INHALATION
• LOWTHRESHOLD ––
• Increased impulsation on inhalation
• Decreased impulsation on exhalation

Hering Breuer reflex
- Breuer inflation reflex:When the lung is inflated → these (stretch) receptors are
stimulated → impulse generated → these impulses are carried by the vagal nerve fibers which emerge from these receptors → impulses ultimately cause inhibition of the inspiratory center (I neurons) → inspiration stops and expiration starts → no stretching of these receptors now → therefore, no inhibition on the neurons now → inspiratory center again begins to send impulse → the next cycle begins.

Hering Breuer reflex
- Breuer deflation reflex:If the lungs are greatly deflated, impulses are set up in
another type of receptors, which travel up via vagus to stimulate inspiration. In ordinary tidal air volume breathing (eupnea) this is not called into action but in such conditions like collapse of the lung (atelectesis) this reflex is activated and inspiratory drives are increased. In a case of collapse of the lung, increase in inspiratory drive will cause more air entry into the healthy parts of the lung, and will thus compensate for the functional loss of lung tissue.

Proprioceptors in the chest wall (' load detecting mechanism')
The organs like muscle spindles detect the fact
that contraction of the muscles of inspiration is
not adequate → send the information to the
anterior horn of the spinal cord → collaterals
arising from these nerve fibers go to the
cerebral cortex

It is possible, one of the mechanisms by which we become conscious to the need of more sustained effort to inspire (dyspnea) is the firing of these collaterals to the cerebral cortex. Activation of these corticopetal fibers is one of the mechanisms of dyspnea.

J receptors. J reflex
J reflex = stimulation of J receptor →
bradycardia + hypotension + hyperpnea +
weakness of skeletal muscles

j receptors and muscular exercise
Fatigue in intact man is caused by central
mechanism. During muscular exercise,
congestion of the pulmonary capillaries lead to
slight accumulation of interstitial fluid → this in
turn leads to stimulation of J receptors →
muscular weakness.

Lung irritant receptors
These are present in the epithelial layer throughout the tracheobronchial tree.
Effects may be of two types :
1. if the receptors of trachea/bigger bronchi are stimulated the response is cough.
2. if the receptors of smaller or smallest bronchi are stimulated, the effect is bronchospasm.

During cough, owing to great
rise of intrapleural veins are compressed →cessation of blood flow through them → no cardiac inflow → no cardiac outflow (output) →
cerebral ischemia. So a severe and prolonged attack of cough may be associated with visual black outs and even fainting due to lack of brain blood supply.

Dependence of Activity of Respiratory Centre on Blood Gas Content
• Fredericq (1890) experiments with cross-circulation.
• The carotid arteries of anaesthetized dogs were cut and then connected cross-wise and the jugular veins were connected separately


• If occlusion of the trachea of the first dog, for example, caused asphyxia, then hyperpnoea developed in the second dog.
• The first dog experienced apnoea some time later, despite increase in the arterial CO2 and decrease in O2 tension.
• This is explained by the fact that the carotid artery of the first dog received blood of the second dog in which hyperventilation caused decrease in the arterial CO2 tension.
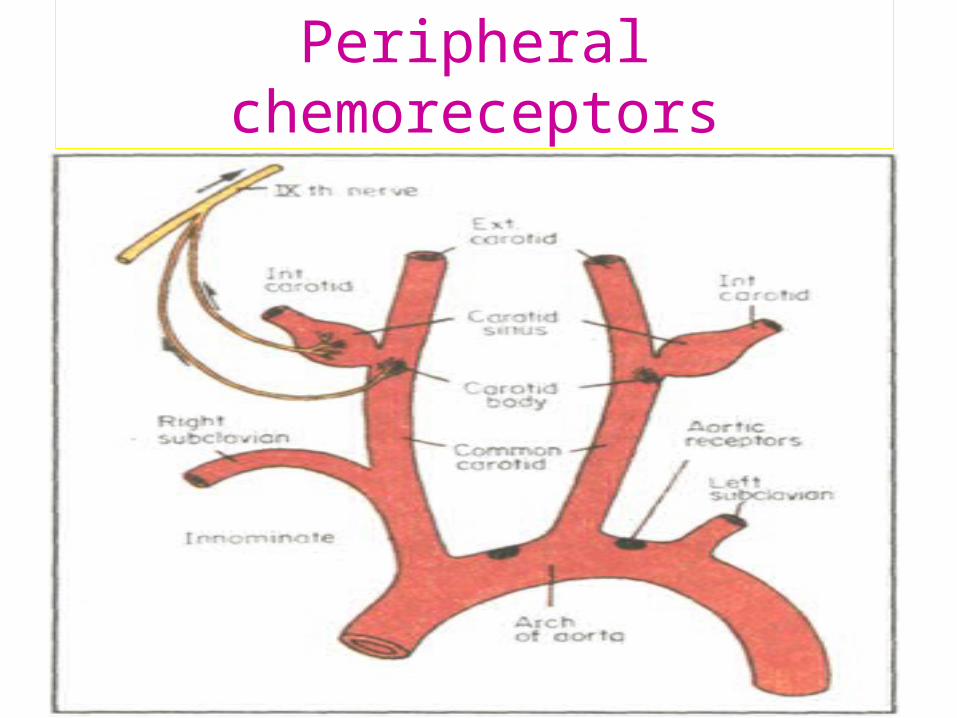
Peripheral chemoreceptors

Peripheral chemoreceptors include two sets,
carotid body (present at the root of external
carotid artery) and aortic bodies (present in
the arch of aorta). They are so placed in the
vascular endothelium. They can detect the
arterial blood PO2, PCO2 and pH.

Baroreceptor reflexes
When blood pressure in the common carotid
artery or arch of aorta rises, these
baroreceptors are stimulated and act in a way
that blood pressure becomes normal.
Conversely, if the blood pressure falls, they act
in the opposite way and the result, again, is
normotension.

CHEMICAL CONTROL OF RESPIRATION
This includes, CO2, O2 and H+ concentrations
of blood and are generally expressed by,
(blood), PCO2, PO2and pH.

Role of Carbon dioxide
Rise of tension of arterial blood CO2 or of
alveolar CO2 causes stimulation of respiration.
Both the rate and depth of respiration are
increased → this leads to washing out of CO2
from the body → abnormal CO2 concentration
of the body tissues are corrected (homeostasis
regained).

TYPES OF RECEPTORS involved in regulation of respiration
• Central chemoreceptors
Н+Extracellular fluid
Spino-cerebral fluid(SCF)
СО2

Central chemoreceptors ('CC')
In the brain tissue fluid as well as in the CSF,
the CO2 is converted into H2CO3 → then H+
ions are liberated → H+ stimulate the CC cells
→ stimulus from CC cells go to the DRG of
medullary RC (respiratory center ) →
stimulation of inspiration.

TYPES OF RECEPTORS involved in regulation of respiration
• PERIPHERAL CHEMORECEPTORS
CAROTID SYNUS AORTHIC ARC
DECREASE 0F О2 PARTIAL PRESSURE
RC СC

Role of Oxygen
A moderate fall of O2 tension of the inspired air or O2 tension of arterial blood unlike those with CO2, has no appreciable effect.
Gross fall of O2 tension of the inspired air or O2 tension of arterial blood (hypoxia) causes stimulation of peripheral chemoreceptors (PC) → neural impulses arising from these PC cells go to the respiratory center → respiration stimulated (hyperpnea).

Role of H+ ion concentration
Rise of H+ ion concentration in the blood (= fall
of blood pH) causes hyperventilation.
Hyperventilation → removal of body CO2 →
reduction of H2CO3 and thus of H+. Thus,
hyperventilation is a compensatory mechanism
against acidosis.

• Decrease of РН=7,32 by 0,01 in the cerebro-spinal fluid causes the 4 l increase in the minute volume of respiration
• Decrease of РО2 below 100mm Hg increases impulsation from peripheral receptors
INFLUENCE FROM THE HIGHER CENTERS
1. The cerebral cortex is able to influence the respiration. Thus, stimulation of premotor cortex leads to tachypnea.
2. Injuries in the lateral part of the hypothalamus produces a depression of respiration.
3. Activities of the limbic system also influence respiration. Limbic system are areas of the brain whose activities produce various emotional changes.