Pancreas; complex gland ( similar to salivary glands) Except of
having anEndocrinepart(secreting insulin& glucagons)
Digestivepart which consist of acini secreting digestive
enzymes :
1.Pancreatic lipase:for digesting fats.2.pancreaticAmylase :
for digesting
carbohydrates.3.PancreaticTrypsin,chymotrypsin,carboxypolypeptidase,elastase
& neuclease : for digesting proteins.
secreted in aninactiveform in the acini :
(trypsinogen,chymptrypsinogen,procarboxypolypeptidase)
toprevent autodigestionof pancreas & this inactivation is
facilitated by a substance calledtrypsin inhibitor.
3. Pancreas
Endocrine
Insulin,glucagon
Exocrine
Enzymes (acini)
Bicarbonate (ducts)
4.
Pancreatic secretions:
when this trypsin inhibitor isoverwhelmedby pancreatic duct
obstruction or pancreatic diseases or damage the proteolytic
inactive enzymes are activated inside pancreatic acini leading to
acute pancreatitis causing death or pancreatic insufficiency.
Inactive panc enzymes areonly activatedwhen they reach the SI ,
by an enzyme released from SIenterokinasestimulated by the presence
of chyme.1 stenzyme activated is trypsinogen to active trypsin
& trypsin in turn activates the other enzymes:
CTP&PCP.
Pancreatic ductioles & ductssecreting HCO3 important for
neutralizing the acid of the chyme coming to the upper SI from
stomach & for preparing the optimal alkaline medium essential
for digestion in SI.
Regulation of pancrearic secretion:
Iby ACH, Cholycystokinin(CCK) & Secretin.
ACH, Cholycystokinin(CCK) :cause secretion of mainly digestive
enzymes while Secretin causes mainly secretion of large amounts of
HCO3.
5.
Phases of pancreatic secretion: The same for of gastric acid
secretion:1.cephalic phase. 2.gastric phase. 3.intestinal
phase.
stimulated by vagi,secretin & CCK.secretin released from
upper SI cells ( S cells) in the presence of acidic chyme causes
secretion of large amounts of HCO3 from pancreatic ducts( for
neutralization of acidic chyme coming from stomach resulting in
formation of Nacl & water)
Secretion of pancreatic enzymes mainly under the control of CCK
which is secreted by SI cells (I-cells) in response to the presence
of food in upper SI specially protein digestion end
products(peptones, proteoses & long chain fatty acids. )
vagal stimulations helps both processes but the effects of
Secretin & CCK are more pronounced.
6. 7. Bile secretion: It helps : fat digestion by saponification
& emulsification of fats. Essential for excretion of several
important waste products from blood as billirubin &
cholesterol. The amount is 1000ml./day.Composition of bile:about
50% are bile salts + billirubin,cholesterol,lecithin & plasma
electrolytes. In the gall bladder water & large amounts of
electrolytes except Ca++ are reabsorbed by gall bladder mucosa, but
the other constituents bile salts,cholesterol & lecithin are
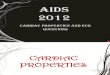
not reabsorbed so become highly concentrated . 8. The Gallbladder
Figure 24.21a, b 9. Figure 24.21a, b Bile Salts and Emulsification
fat globule Water (polar) bile salts fat droplets bile salt
phospholipids triglycerides Increases surface area for attack by
lipases. polar coating 10.
Emptying of gall bladder:
Needs:
contraction of gall bladder wall & relaxation of sphincter
of oddi(SOO)
CCKplays an important role in contraction of gall bladder wall
& to less degree relaxation of (SOO)
Relaxation of (SOO)mainly in response to movement of the wall
of upper SI.
11. 12.
Bile salts & their functions:
0.6gms. is secreted /day.
Synthesized from cholesterol which is converted to cholic acid
& chenodeoxycholic acid & both combine with glycin or
taurin to form glyco or tauro conjugated bile acids.
Functions:
The main functions is :
1.Emulsificatin of fats to form micelles to facilitate Fat
absorption .
2.Secretion of some important waste products as billirubin and
cholesterol.
The enterohepatic circulation of bile salts from the SI is
through the terminal ileum TI to the liver then to SI again ,so in
TI disease or removal, this enterohepatic circulation of bile salts
is interupted causing bile salts deficiency and so fat
malabsorption.
The hormone Secretin causes secretion of HCO3 & not bile
acids from the bile ductioles for neutralization of excess acid
coming from stomach in cooperation with the pancreatic HCO3.
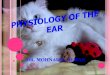
13. Gall bladder Cholesterol Largeintestine Ileum Duodenum Liver
Bilesalts Stomach Bilesalts Bilesalts Bilesalts Bilesalts Bilesalts
Sphincter ofOddi Portal circulation These salts are reabsorbed in
theileumand returned to the liver where they are once again
secreted into bile only 3-4 g ofbile saltsin body, thus highly
recycled = active transport 14.
Gall stones formation:
Is mainly due to imbalance between bile salts & cholesterol
content of bile ,either more cholesterol or less bile salts so
excess cholesterol will precipitate to form cholesterol gall
stones.
Causes of gall stones:
1.Too much absorption of water to form concentrated bile easy
to precipitate.
2.Too much absorption of bile acids.
3.Too much secretion of cholesterol into the bile mainly from
diet.
4.Inflamation of gall bladder epithelium.
Medical therapy of gall stones:
Although the mainstay of gall stones therapy is
surgery,sometimes the patient is given bile salts in form of
ursodeoxycholic acid or chenodeoxycholic acid for at least 1 year,
which help in redissolution of cholesterol gall stones by
increasing the ratio of bile salts in relation of cholesterol.
15.
Secretions of SI:
Of 3 types:
1.Brunner glands for mucose secretion.
2.crypts of Liberkhan for secretion of pure extracellular fluid
to aid absorption of intestinal contents by active secretion of
HCO3 & Cl- into the crypts these cause osmotic movement of
water.
3.SI enzymes present on villi brush border consisting of;
Several different peptidases for splitting peptides into amino
acids.
Several disaccharidases as sucrase,maltase,isomaltase and
lactase.
Small amounts of intestinal lipase for splitting neutral fats
into glycerol & fatty acids.
The regulation of SI secretions is by local enteric stimuli
through local enteric reflexes and hormonal secretions specially
Secretin & CCK.
16.
Large intestinal secretions:
Are:
1.Mucose secreted by mucose cells in colonic wall .
The mucose protects the colonic wall from excoriation &
bacterial activity and provides an adherent medium for holding
feces together.
2.HCO3 by crypts of Liberkhan ,stimulated by tactile stimuli
& pelvic PS nerves.
The HCO3 protects the colonic wall from acids formed deep in
the feces by intestinal flora.