Embed Size (px)
Citation preview
PEDIATRIC ANAPHYLAXIS
PEDIATRIC STAGEFACULTY OF MEDICINE CHRISTIAN UNIVERSITY OF
INDONESIA23 SEPTEMBER – 16 NOVEMBER
PHILJEUWBENS ADITYA RAHANTOKNAM0761050016
Definition
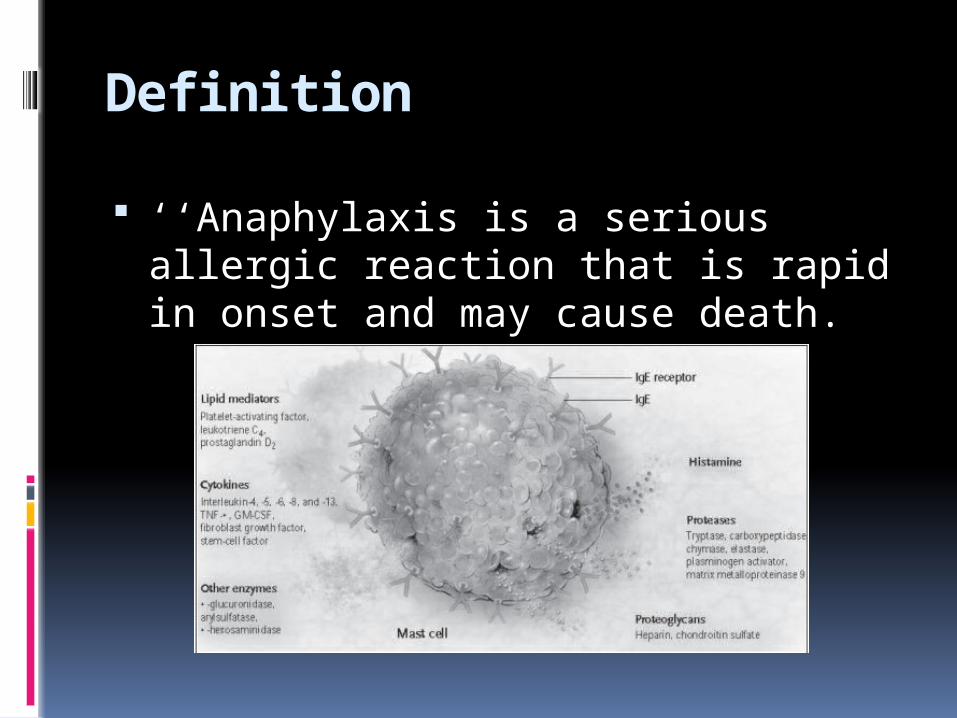
‘‘Anaphylaxis is a serious allergic reaction that is rapid in onset and may cause death.
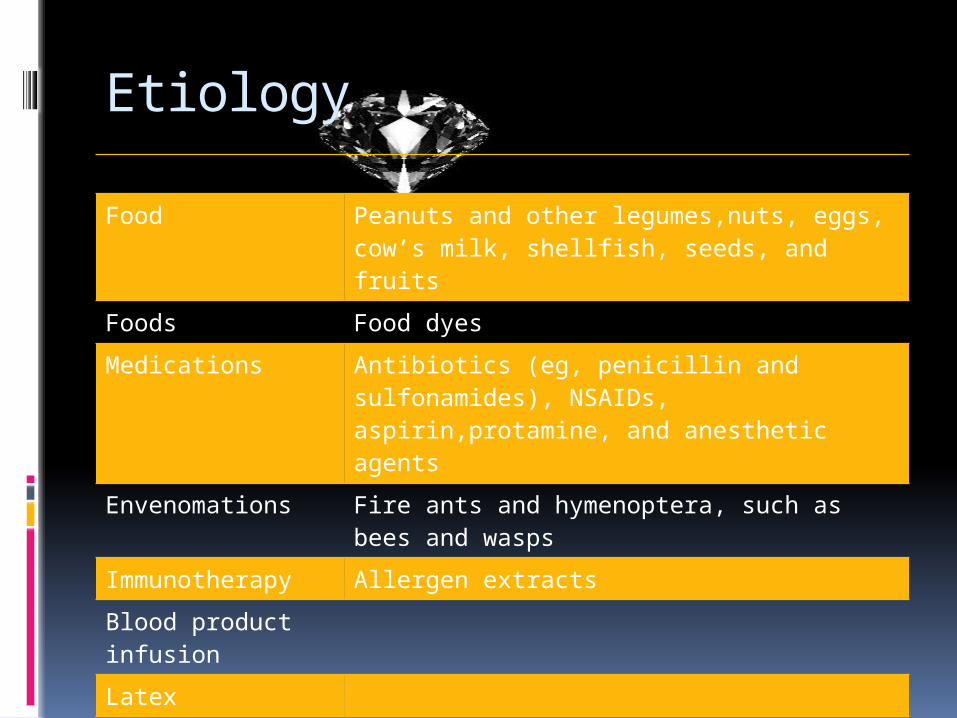
Etiology
Food Peanuts and other legumes,nuts, eggs, cow’s milk, shellfish, seeds, and fruits
Foods Food dyesMedications Antibiotics (eg, penicillin and sulfonamides),
NSAIDs, aspirin,protamine, and anesthetic agents
Envenomations Fire ants and hymenoptera, such as bees and wasps
Immunotherapy Allergen extractsBlood product infusion Latex Vaccines Radiographic mediaIdiopathic Exercise
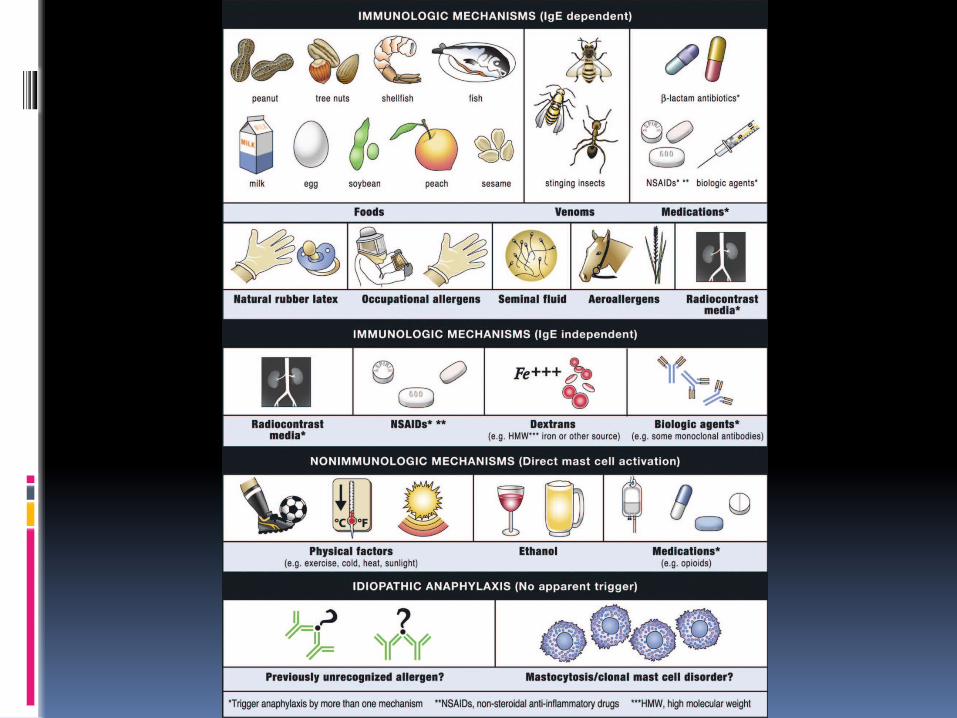
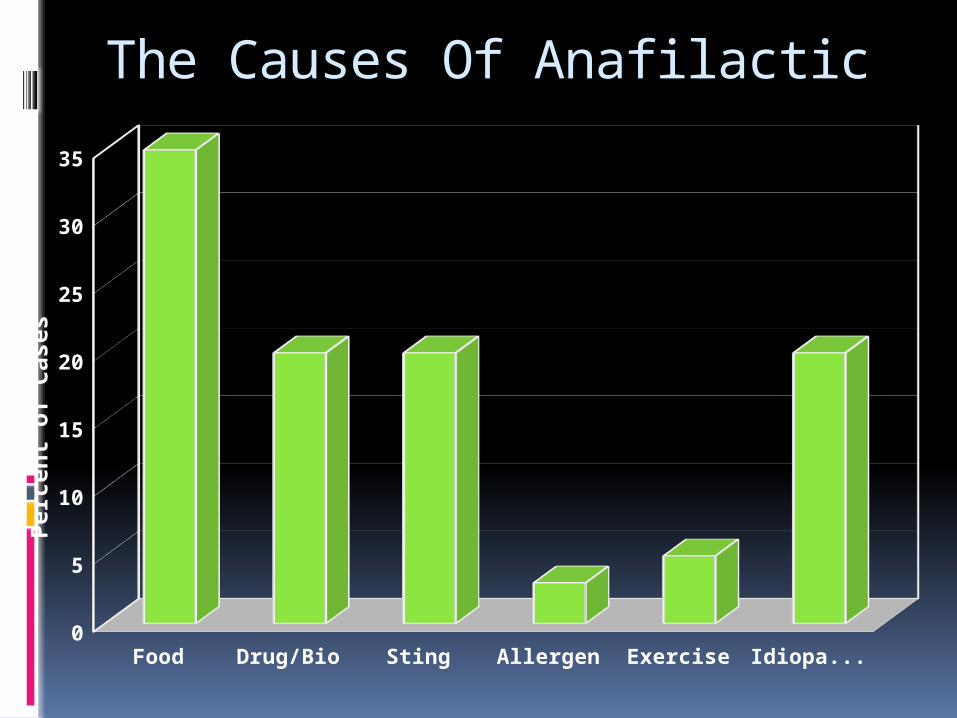
The Causes Of Anafilactic
Food Drug/Bio Sting Allergen Exercise Idiopathic0
5
10
15
20
25
30
35
Perc
ent o
f Cas
es
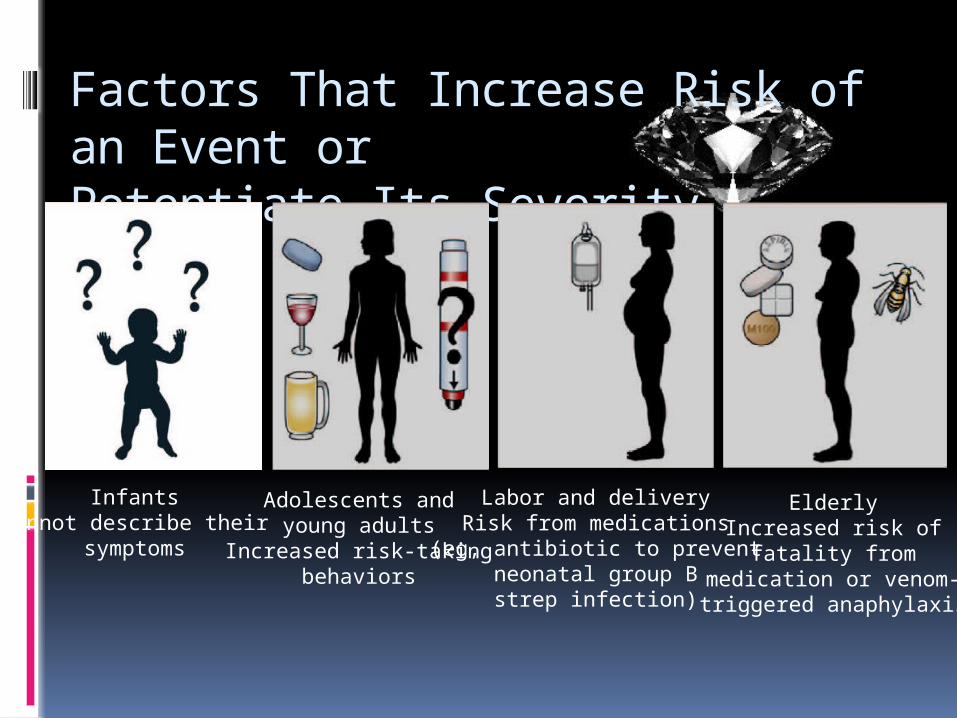
Factors That Increase Risk of an Event or Potentiate Its Severity
InfantsCannot describe their
symptoms
Adolescents andyoung adults
Increased risk-takingbehaviors
Labor and deliveryRisk from medications
(eg, antibiotic to preventneonatal group Bstrep infection)
ElderlyIncreased risk of
fatality frommedication or venom-triggered anaphylaxis
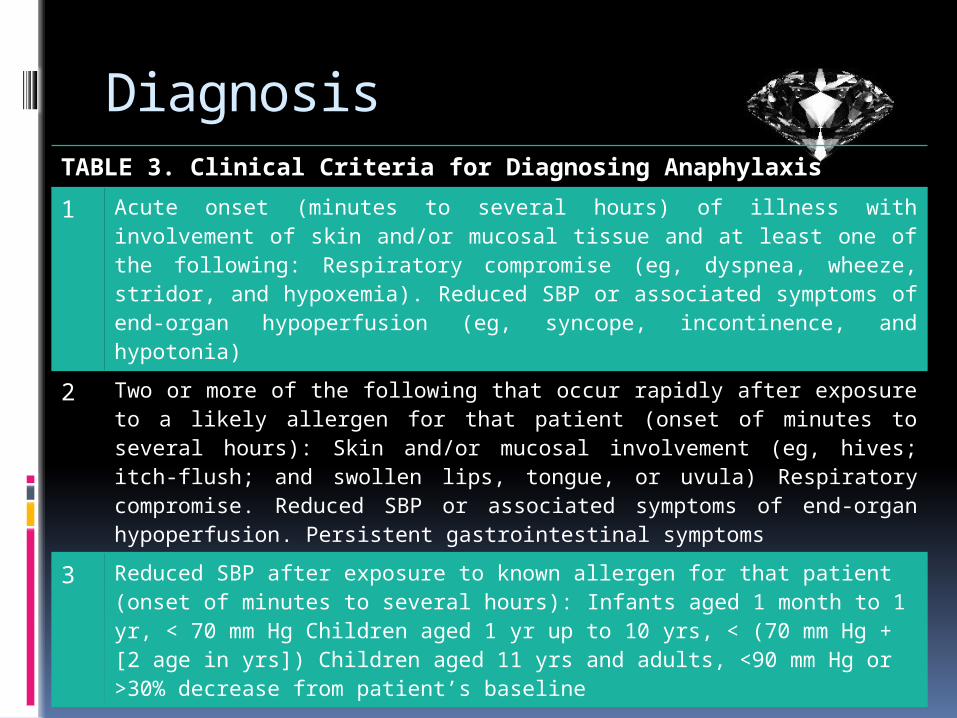
DiagnosisTABLE 3. Clinical Criteria for Diagnosing Anaphylaxis1 Acute onset (minutes to several hours) of illness with involvement of skin
and/or mucosal tissue and at least one of the following: Respiratory compromise (eg, dyspnea, wheeze, stridor, and hypoxemia). Reduced SBP or associated symptoms of end-organ hypoperfusion (eg, syncope, incontinence, and hypotonia)
2 Two or more of the following that occur rapidly after exposure to a likely allergen for that patient (onset of minutes to several hours): Skin and/or mucosal involvement (eg, hives; itch-flush; and swollen lips, tongue, or uvula) Respiratory compromise. Reduced SBP or associated symptoms of end-organ hypoperfusion. Persistent gastrointestinal symptoms
3 Reduced SBP after exposure to known allergen for that patient (onset of minutes to several hours): Infants aged 1 month to 1 yr, < 70 mm Hg Children aged 1 yr up to 10 yrs, < (70 mm Hg + [2 age in yrs]) Children aged 11 yrs and adults, <90 mm Hg or >30% decrease from patient’s baseline
SBP indicates systolic blood pressure. Adapted from Sampson et al.4 Copyright 2006, with permission from American Academy of Allergy, Asthma and Immunology.
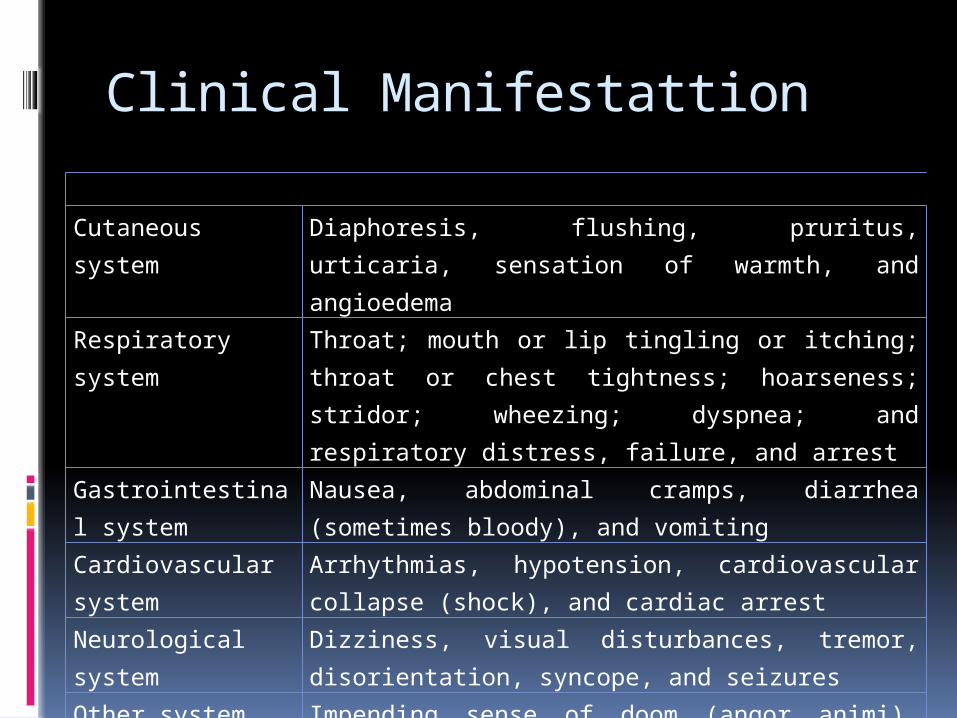
Clinical Manifestattion
Cutaneous system
Diaphoresis, flushing, pruritus, urticaria, sensation of warmth, and angioedema
Respiratory system
Throat; mouth or lip tingling or itching; throat or chest tightness; hoarseness; stridor; wheezing; dyspnea; and respiratory distress, failure, and arrest
Gastrointestinal system
Nausea, abdominal cramps, diarrhea (sometimes bloody), and vomiting
Cardiovascular system
Arrhythmias, hypotension, cardiovascular collapse (shock), and cardiac arrest
Neurological system
Dizziness, visual disturbances, tremor, disorientation, syncope, and seizures
Other system Impending sense of doom (angor animi), uterine cramps, metallic taste, rhinorrhea, and increased lacrimation

SKIN
ITCHING FLUSHING
HIVES (URTICARIA) SWELLING

Eye
ITCHING CRY (TEARS)
REDNESS SWELLING
Nose and Mouth
SNEEZING RUNNY NOSE NASAL CONGESTION
SWELLING OF TOGUE METALIC TASTE
Lungs and Throat
DIFFICULTY BREATHING COUGHING CHEST TIGHTNESSWHEEZING OR OTHER SOUND
INCREASED MUCUS PRODUCTIONTHROAT SWELLING
OR ITCHINGCHANGE IN VOICES OR
SENSATION OF CHOCKING
Heart and circulation
DIZZINESS FAINTINGWEAKNESS
RAPID, SLOW, IRREGULERHEART RATE
LOW BLOOD PRESSURE
Digestive System
NAUSEA VOMITTING
CRAMPS DIARRHEA
Nervous System
ANXIETY CONFUSION
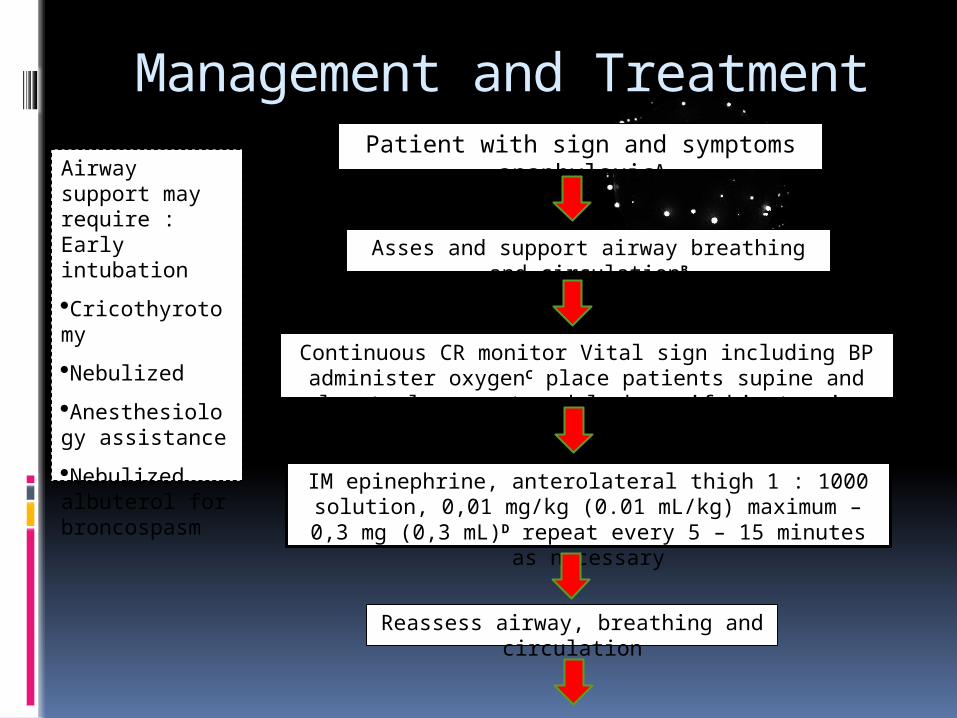
Patient with sign and symptoms anaphylaxisA
Asses and support airway breathing and circulationB
Continuous CR monitor Vital sign including BP administer oxygenC place patients supine and elevate legs or trendelenberg if hipotensive
IM epinephrine, anterolateral thigh 1 : 1000 solution, 0,01 mg/kg (0.01 mL/kg) maximum – 0,3 mg (0,3 mL)D repeat every 5 – 15
minutes as necessary
Reassess airway, breathing and circulation
Airway support may require : Early intubation
·Cricothyrotomy
·Nebulized
·Anesthesiology assistance
·Nebulized albuterol for broncospasm
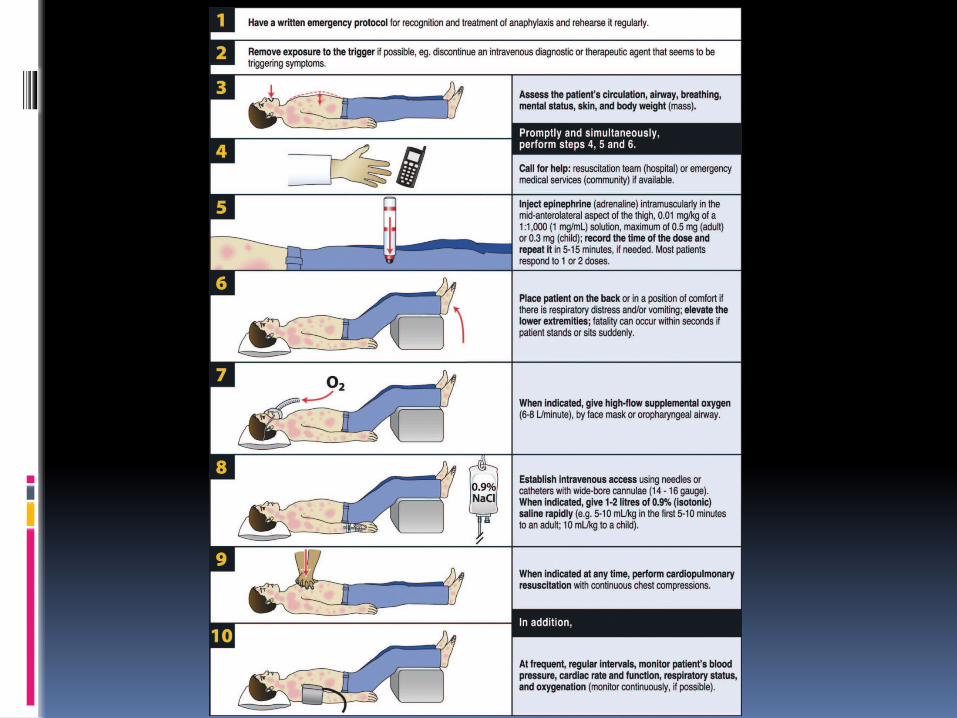
Management and Treatment
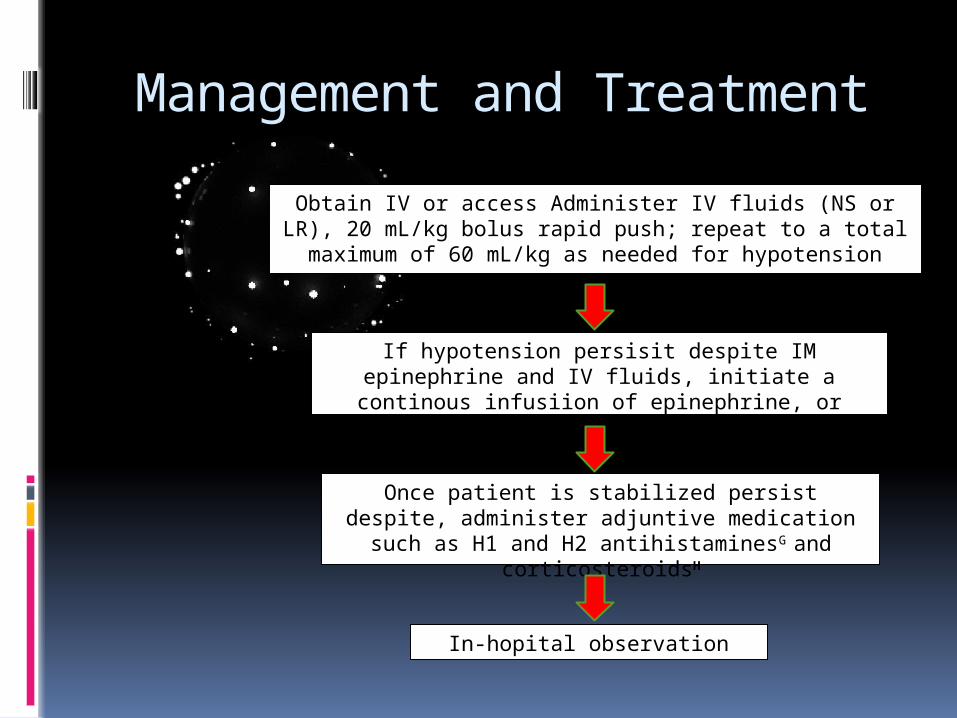
If hypotension persisit despite IM epinephrine and IV fluids, initiate a continous infusiion of epinephrine, or vasopresor
agentE, or glucagonF
Once patient is stabilized persist despite, administer adjuntive medication such as H1 and H2 antihistaminesG and
corticosteroidsH
In-hopital observation
Obtain IV or access Administer IV fluids (NS or LR), 20 mL/kg bolus rapid push; repeat to a total maximum of 60 mL/kg as needed for
hypotension
Management and Treatment
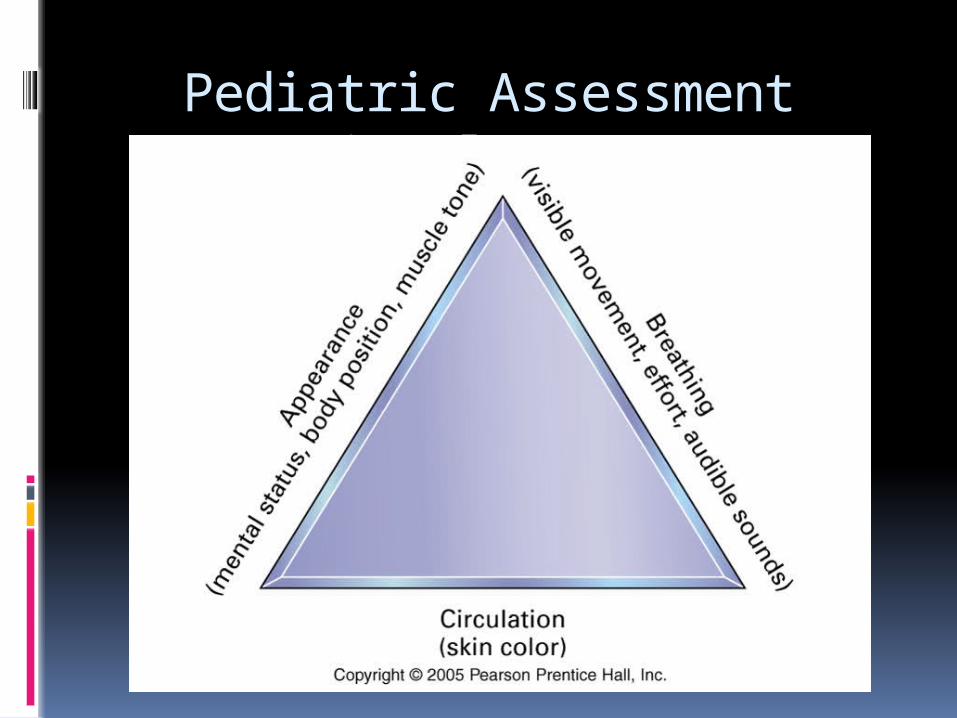
Pediatric Assessment Triangle (PAT)
Assessing Mental Status
Use the AVPU method of assessing mental status, taking the child’s age and developmental characteristics into account. You may need to raise your voice to elicit a response to verbal stimuli. Tap or pinch the patient to test for response to painful stimulus. Never shake and infant or child.
Rapid Cardiopulmonary Assessment
AirwayBreathingCirculation
Should take less than 30 seconds to complete
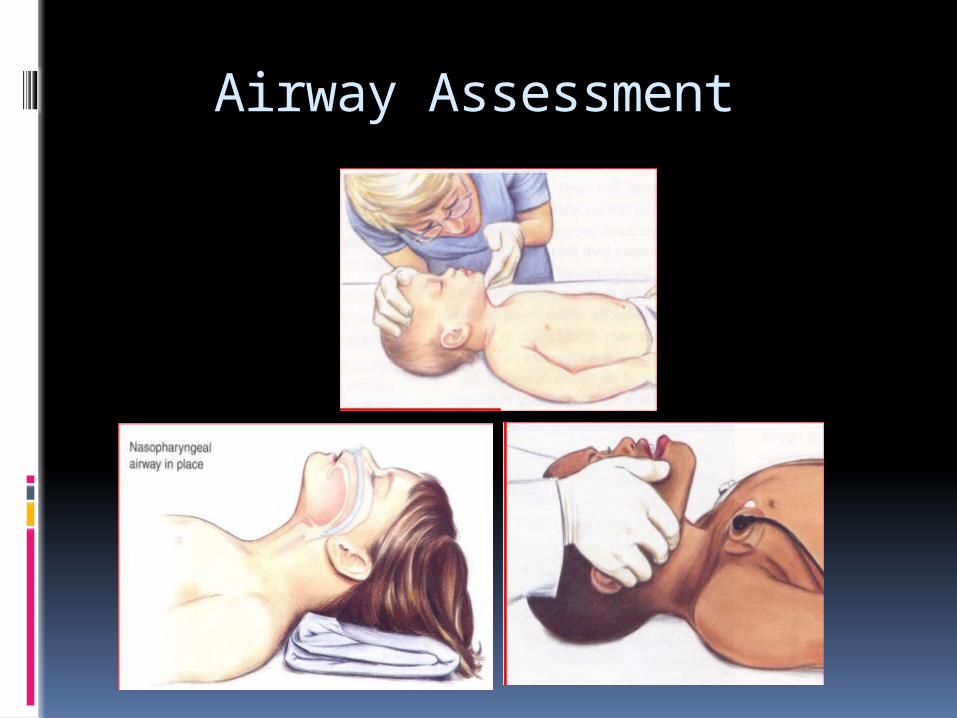
Airway Assessment
Breathing
RR Respiratory
Mechanics Retractions,
Accessory Muscles use and NasalFlaring
Head Bobbing Grunting Stridor Wheezing
Air Entry Chest Expansion Breath Sounds
Color
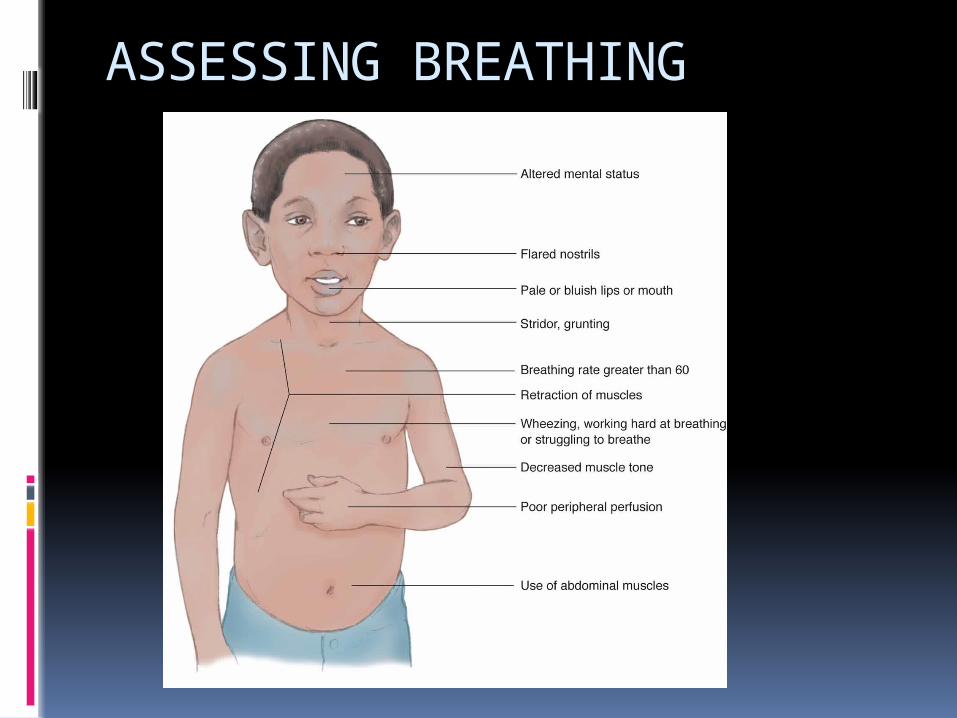
ASSESSING BREATHING
Color – cyanosis indicates poor oxygenation
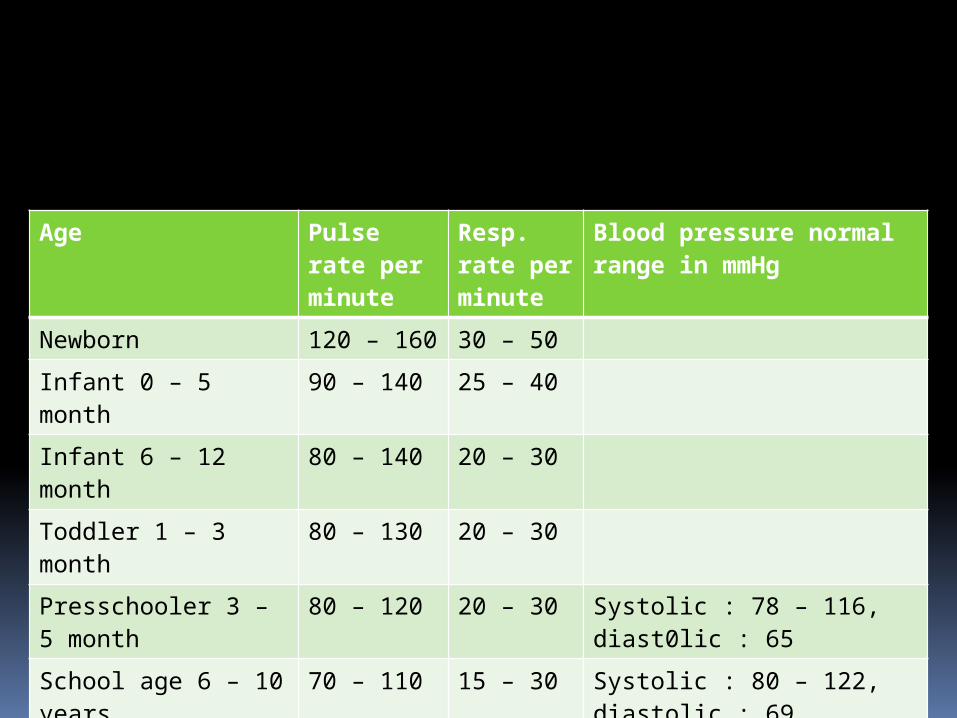
Age Pulse rate per minute
Resp. rate per minute
Blood pressure normal range in mmHg
Newborn 120 – 160 30 – 50 Infant 0 – 5 month 90 – 140 25 – 40Infant 6 – 12 month 80 – 140 20 – 30 Toddler 1 – 3 month 80 – 130 20 – 30Presschooler 3 – 5 month
80 – 120 20 – 30 Systolic : 78 – 116, diast0lic : 65
School age 6 – 10 years
70 – 110 15 – 30 Systolic : 80 – 122, diastolic : 69
Adolescent 11 – 14 years
60 – 105 12 – 20 Systolic : 88 – 140, diastolic : 76
Circulation
Heart rate BP
Vol/strength of central pulses
Peripheral pulses Present/absent Volume/strength
Skin perfusion Cap.refill time
Color Mottling
Temperature CNS perfusion
Responsiveness Recognizes parents Muscle tone Pupil size Posturing
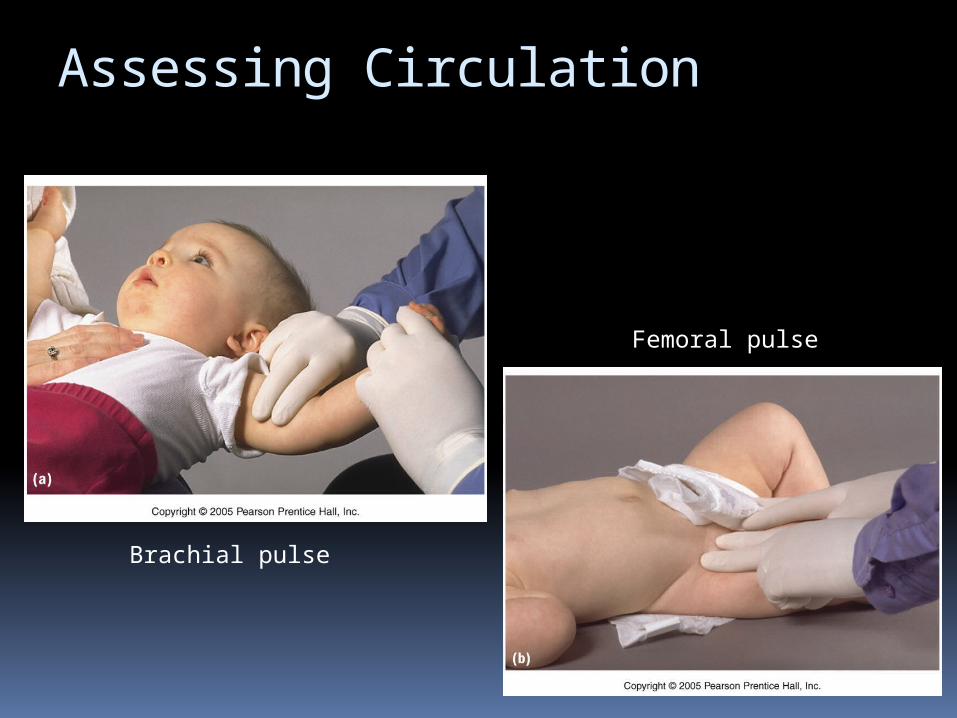
Assessing Circulation
Brachial pulse
Femoral pulse
Treatment and management
Antihistamines Block H1 and H2 receptors
Epinephrine for bronchospasms stimulates the reformation of tight
junctions between endothelial cells IV fluids to support blood pressure Desensitization
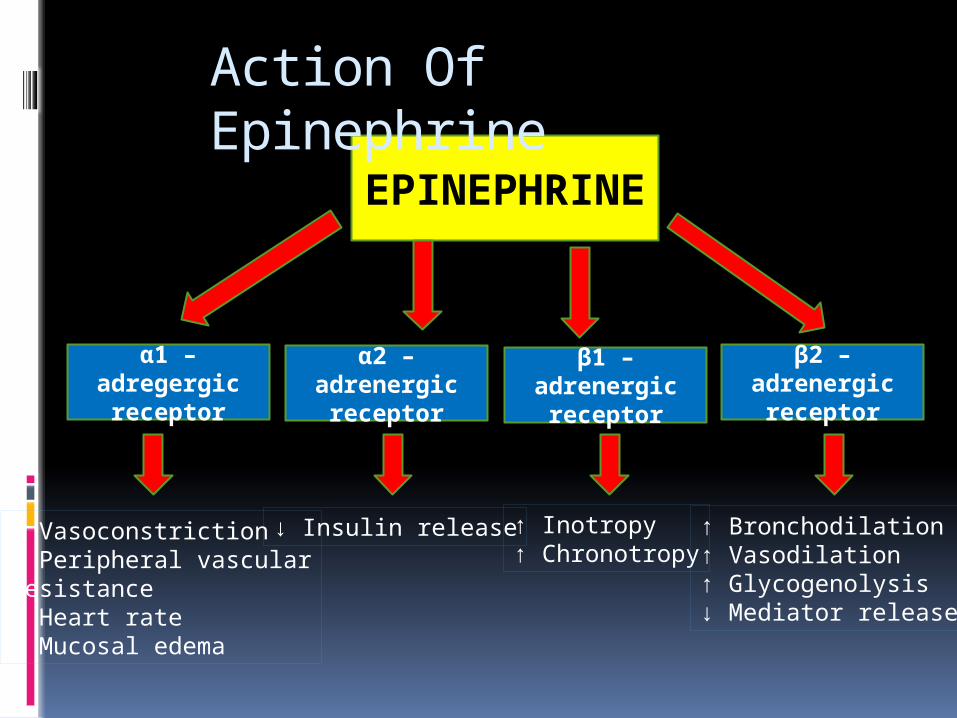
EPINEPHRINE
α1 – adregergic receptor
α2 – adrenergic receptor
β1 – adrenergic receptor
β2 – adrenergic receptor
↑ Vasoconstriction↑ Peripheral vascularresistance↑ Heart rate↓ Mucosal edema
↓ Insulin release ↑ Inotropy↑ Chronotropy
↑ Bronchodilation↑ Vasodilation↑ Glycogenolysis↓ Mediator release
Action Of Epinephrine
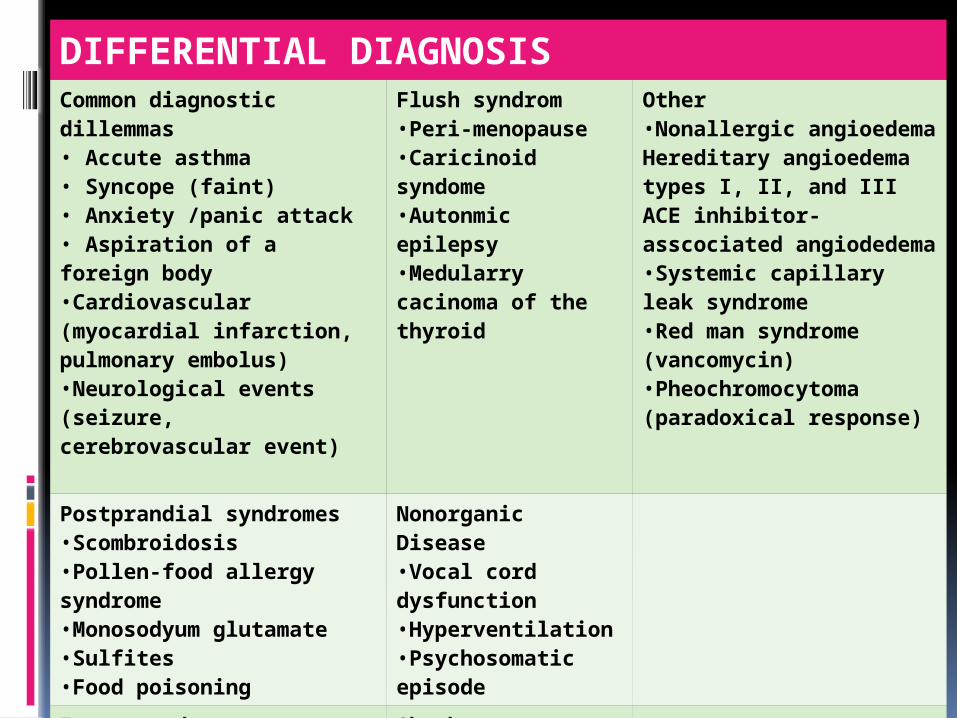
DIFFERENTIAL DIAGNOSISCommon diagnostic dillemmas• Accute asthma• Syncope (faint)• Anxiety /panic attack • Aspiration of a foreign body •Cardiovascular (myocardial infarction, pulmonary embolus)•Neurological events (seizure, cerebrovascular event)
Flush syndrom •Peri-menopause•Caricinoid syndome•Autonmic epilepsy •Medularry cacinoma of the thyroid
Other •Nonallergic angioedema Hereditary angioedema types I, II, and IIIACE inhibitor-asscociated angiodedema•Systemic capillary leak syndrome•Red man syndrome (vancomycin)•Pheochromocytoma (paradoxical response)
Postprandial syndromes•Scombroidosis•Pollen-food allergy syndrome•Monosodyum glutamate•Sulfites •Food poisoning
Nonorganic Disease•Vocal cord dysfunction•Hyperventilation •Psychosomatic episode
Excess endogenous histamin Mastocytosis/clonal mast celldisordersBasophilic leukemia
Shock •Hypovolemik •Cardiogenic•Distributive •Septic

THANK YOU