Embed Size (px)
Citation preview
presented by:Dr. Muntather M. Hassan
Pain: is unpleasant sensory and
emotional experience associated with
actual and potential tissue damage.
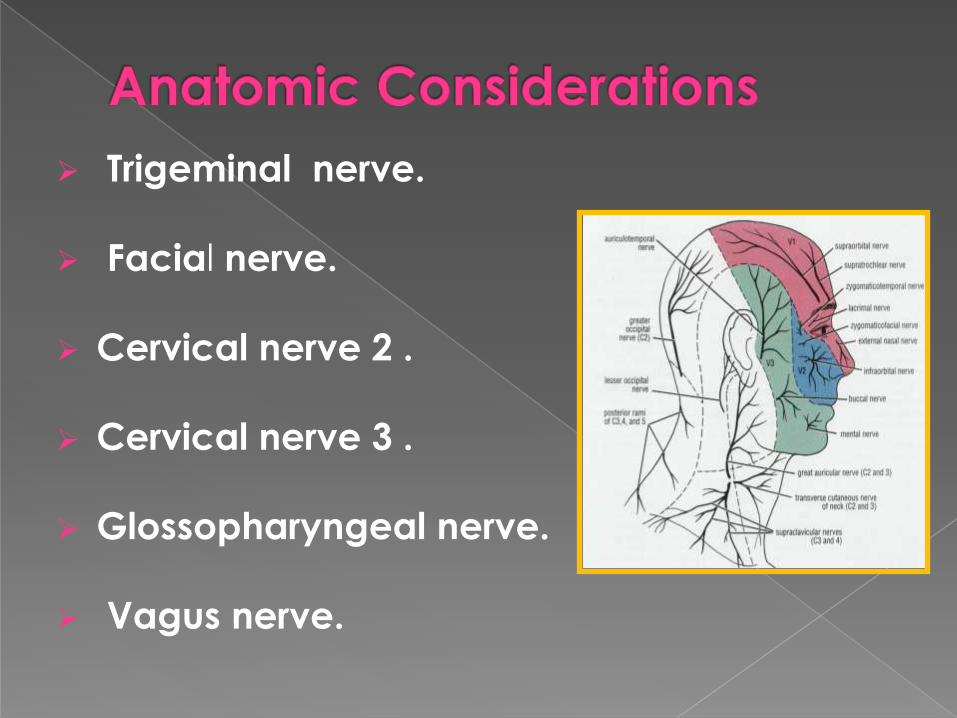
Trigeminal nerve.
Facial nerve.
Cervical nerve 2 .
Cervical nerve 3 .
Glossopharyngeal nerve.
Vagus nerve.
1- Local pain: Dental : (pulpitis., dentine hypersensetivity
,periapical periodontitis.cracked tooth syndrome
Gingival: (e.g primary herpetic gingivostomatitis,
Mucosal: (e,g ulceration)
Salivary gland: (acute suppurative sialadenitis)
Temporomandibular joint:
Maxillary sinus: (sinusitis,malignancy)

2- Neurological pain: Trigeminal neuralgia
Glossopharyngeal neuralgia
Ramsy hunt syndrome
Postherpetic neuralgia
3- Vascular :
Giant cell arteritis and variant
Migraine and variant
Cluster headache ,chronic paroxysmal hemicrania
4- Psychogenic pain: Atypical facial pain
Atypical odontalgia
Burning mouth syndrome
5- Referred pain:
Cardiac pain
A-history:1-Chief complaint.
2-History of present illness.
Pain Characteristics
Intensity
Quality
Location
Onset
Associated events at onset
Duration and timing of pain
Course of symptoms since onset
Activities that increase pain
Activities that decrease pain
Associated symptoms (eg, altered sensation, swelling)
Previous treatments and their effects
Referral
-Connective tissue disease.
-Demylination disorder.
-Metastatic disease.
-Ischemic heart disease.
4-Social history:
-History of traumatic event prior to onset of pain.
-Change in work, or problem regarding marital
state.
3-Past medical history
B-physical examination:
1. Inspection of the head and neck skin, 2. Palpation of masticatory muscles,
3. Assessment and measurement of the range of mandibular movement.
4. Palpation of soft tissue .
5. Palpation of the temporomandibular joint6. Palpation of cervical muscles and assessment of
cervical range of motion.
7. Cranial nerve examination.
8. General inspection of the ears, nose, and oropharyngeal areas.
9. Examination and palpation of intraoral soft tissue.
10. Examination of the teeth and periodontium (including occlusion.
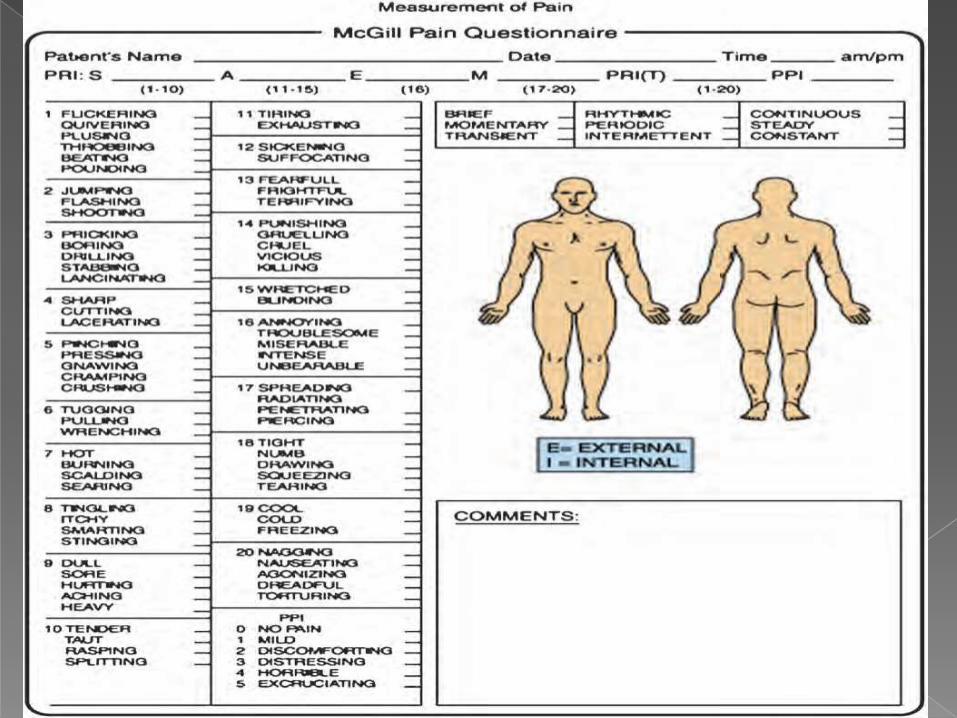
Methods of pain measurement:
1-visual analog scale (VAS)
0 -----------------------------------10
no pain worst possible pain
2-Descriptive rating scales (eg, no pain, mild, moderate, severe pain).
3-Faces rating scale.
4-The McGill Pain Questionnaire (MPQ) .
-Used to confirm the diagnosis or rule out
serious disease.
-Extent of an identified disorder.
-Most OFP not produce abnormality.

1-Myofascial pain.
2-Traumatic injuries.
3-Arthritis &Arthrosis:
(a)infective .
(b) systemic.
(c) degenerative.
4-Internal derangement.
Myofascial pain
diffuse poorly localized periauricular pain.
May associated with parafunctional habits .
the pain may be severe in morning.
the pain is more severe during periods of
tension and anxiety.
the range of mandibular movement decrease .
"trigger points," where muscles have taut,
palpable band regions that twitch when
manually percussed.
-Education of patient and explanation .
-Self care to eliminate oral habit such as gum
chewing , clenching of teeth.
-thermal therapy(U/S, laser ).
-Intraoral appliance.
-Pharmacotherapy:
-NSAID.
-Muscle relaxant drugs ,
-Antianxiety drugs.
-TCAs.
Botox injection.
Trigger point block therapies, using local anesthetic in
combination with corticosteroid.
Pain on palpation directly over TMJ.
Limitation in joint range of motion.
Deviation on opening.
Joint noises consistently associated
with pain.
Joint crepitus.
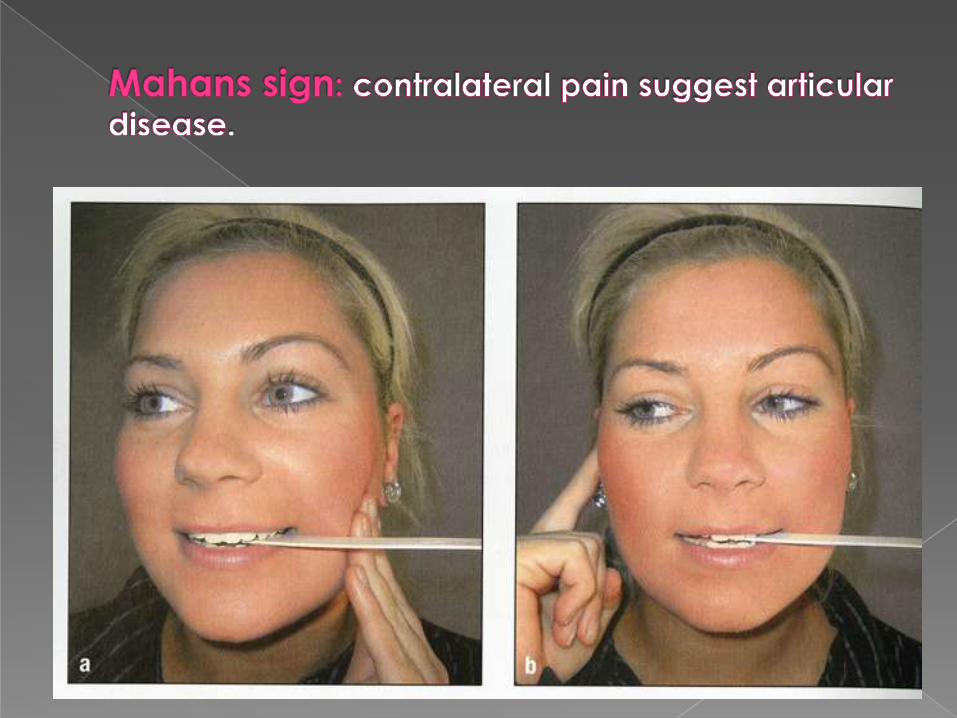
Mahan sign (+ve in Wilkes II,III and IV).

Soft laser apparatus in useultrasound apparatus in use
Rare pain disorder characterized by
continuous lancinating like pain in site of
previous tooth extraction.
Usually in lower 3rd molar region.
Pain not interfere with sleep.
Radiographically appear as moth eaten or
soap bubbles in site of previous extraction.
Treated by resection of bone area with
pain ,
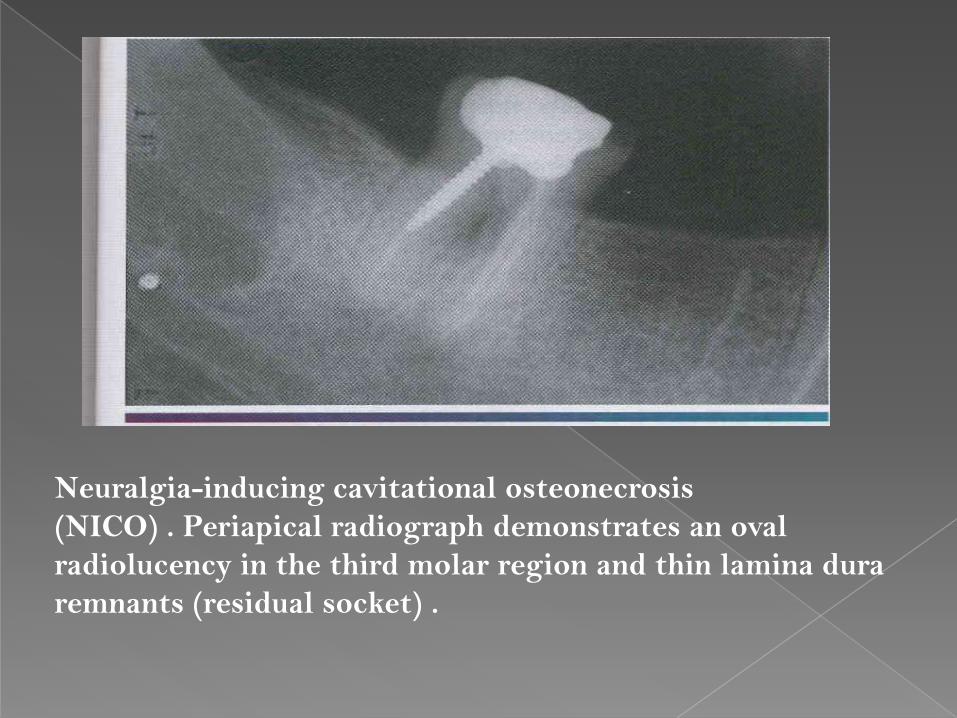
Neuralgia-inducing cavitational osteonecrosis
(NICO) . Periapical radiograph demonstrates an oval
radiolucency in the third molar region and thin lamina dura
remnants (residual socket) .
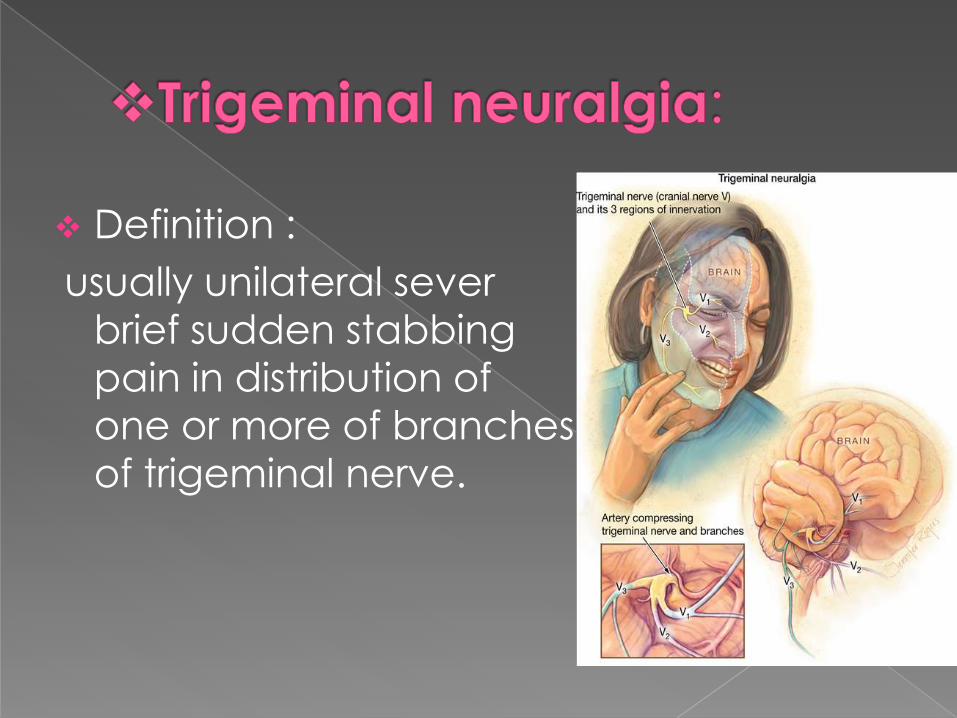
Definition :
usually unilateral sever
brief sudden stabbing
pain in distribution of
one or more of branches
of trigeminal nerve.
TN divided to primary and secondary(symptomatic)
the primary TN are result of vascular
compression of trigeminal nerve near its entry
into the pons (superior cerebellar artery).
Secondary TN causes include :multiple sclerosis,
tumors ,basilar artery eneurysim or actasia.
It presents as episodic ,recurrent unilateral
facial pain, described as sudden high intensity
stabbing or electric like shock.
lasts for a few seconds to minutes ,
Pain is frequently triggered by trivial stimulation:
such as touching of face, washing ,shaving ,
chewing and talking.
It occurs mostly after 5th decade.
Clinical examination of face is nearly always
normal.
If sensory loss is present a mass lesion is more likely
In young patients with TN, multiple sclerosis should
be considered.
Diagnosis depend on history and
clinical examination.
A careful search for ipsilateral
dental pathology should be
undertake
MRI and MRA and performed if
there is suspicion of underlying
pathology.
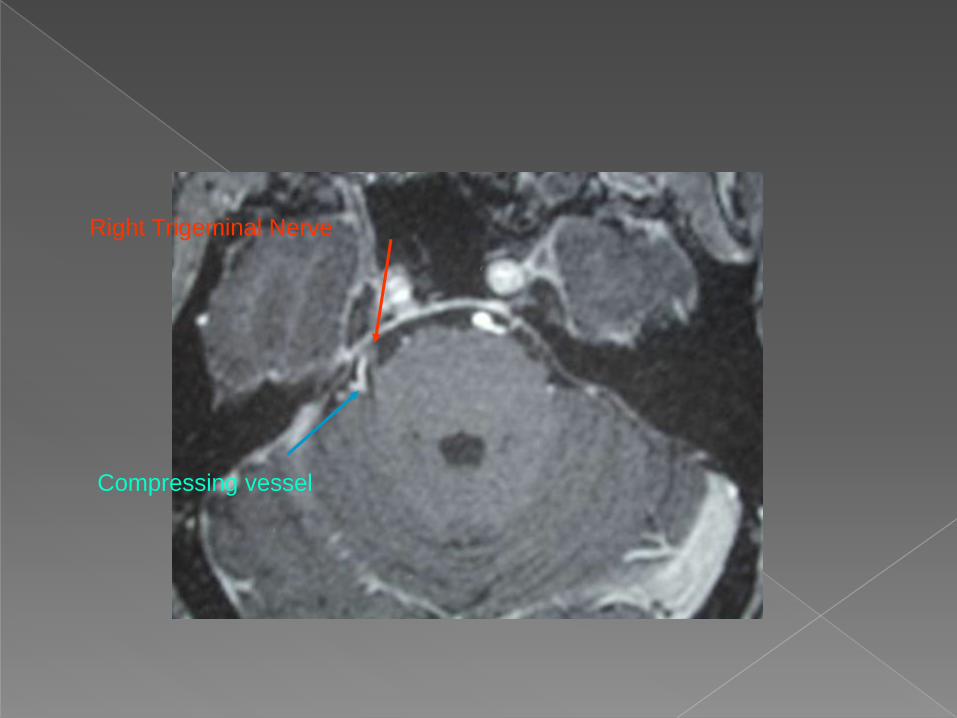
Right Trigeminal Nerve
Compressing vessel
1- Medical treatment: Carbamazepine 200 mg _ 1600mg bid .(effective
in 75% as first line of treatment)
Oxcarbazepine 600mg _3000mg It used in patients
who are sensitive to Carbamazepine.
Baclofen 15mg _80mg tid.
Gabapentine 900mg _3600mg tid.
Lamotrigine 25mg _300mg.
Clonazepam 1.5 mg _ 6mg
Phenytoin 300 mg
Valproate sodium 500mg _1500mg
2- Surgical treatment(invasive):indicated If medical treatment (carbamazepine) has
been ineffective after 4 weeks at maximum
tolerated dose .
Surgical treatment divided into 3 groups:
a) peripheral procedures :include alcohol injection, cryosurgery
,nerve avulsion
a) Percutaneous ganglion procedure: include radiofrequent
thermocoaglation ,glycerol injection , balloon
compression,Gamma knife.
b) Open operations : microvascular decompression ,trigeminal root section,
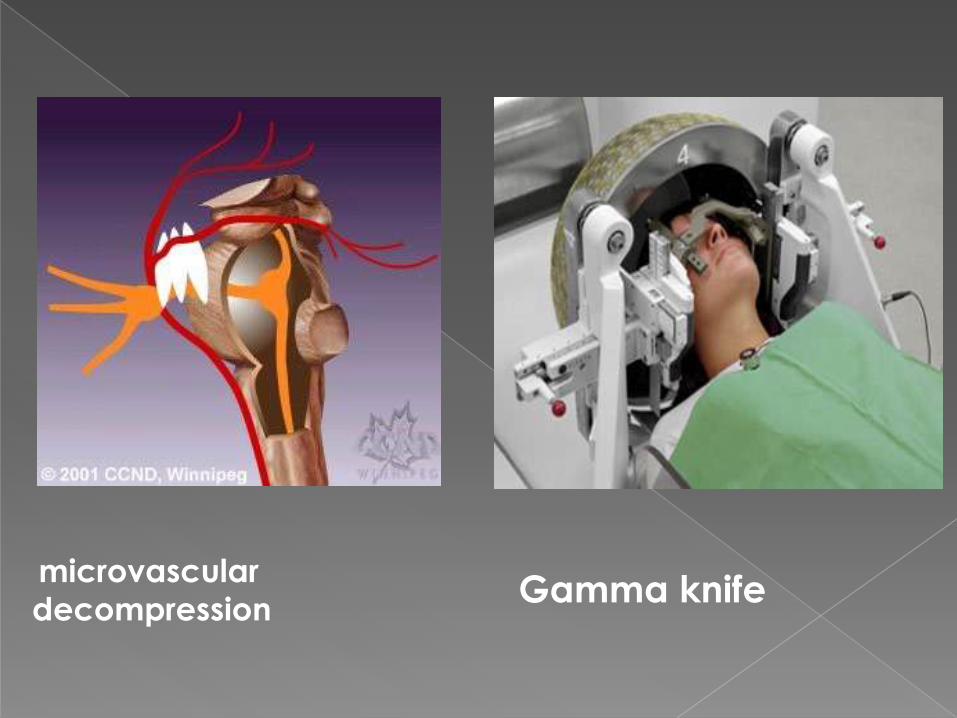
Gamma knifemicrovascular
decompression
-Pain is typically aching,buring,or shock
like.
-Potential sequela of infection with
herpes zoster.
Pain persist longer than one month after
healing vesicle classified as PHN.
Post-herpetic neuralgia
-Antiviral and corticosteroids after
presentation of rash reduce incidence of
postherptic neuralgia.
-Anticonvulsant drugs
-Local anesthesia injected to painful site.
Clinical features : Pain similar to character of TN.
Affect tonsil ,tongue base, ear,and intra articular
area.
Patient often point just to behind mandible angle.
Triggered by yawing and swallowing.
may be associated with a vasovagal reflex,
The application of a topical anesthetic to the
pharyngeal mucosa eliminates glossopharyngeal
nerve pain.
Glossopharangeal neuralgia

Management:
-Anti convulsion drugs,carbamezipine.
-Vascular decompression.
-Percutaneous R.F. at the jugular foramen.
-Intracranial or extra cranial neuroectomy.
Etiology:
The most common causes of glossopharyngeal
neuralgia areintracranial or extracranial tumors and
vascular abnormalities that compress CN IX.
Glossopharangeal neuralgia
presents as a paroxysmal stabbing pain in the
distribution of the greater or lesser occipital nerves. It may be caused by trauma,
Palpation below the superior nuchal line may
reveal a tender spot .
Treatment has included occipital nerve block,
neurolysis, C2 dorsal root gangionectomy ,
Its caused by Trigeminal nerve injuries may result
from facial trauma or from surgical procedures,
such as the removal of impacted third molars, the
placement of dental implant
Clinical Manifestations: The pain may be persistent
or occur only in response to a stimulus, such as a
light touch.
Patients with nerve damage may experience
anesthesia , paresthesia, allodynia , or
hyperalgesia .

Treatment: may be surgical ,nonsurgical, or both,
Systemic corticosteroids a when administered
within the first week after a nerve injury.
TCAs
Anticonvulsant drugs, Gabapentin.
Topical capsaicin .
chronic pain conditions that develop as a result of
injury.
patients suffer from allodynia, hyperalgesia, and
spontaneous pain that extends beyond the
affected nerve dermatome.
it accompanied by motor and sweat
abnormalities, atrophic changes in muscles and
skin, edema,
Types of CRPs :
1- CRPS I was previously termed reflex sympathetic
dystrophy (RSD),
2- CRPS II was previously termed causalgia.
Etiology and Pathogenesis:
believed to result from changes after trauma that
couples sensory nerve fibers with sympathetic
fibers.
Treatment: physical therapy.
block of regional sympathetic ganglia or regional
intravenous blockades with guanethidine
,reserpine, or phenoxybenzamine, Bisphosphonates such as alendronate or
pamidronate.
Paroxysmal pain of facial nerve, may result of
herpes zoster of geniculate ganglion.
-Clinical features:
-Pain at the ear, anterior tongue, soft palate.
-Not intense like T.N.
- Ramsay-hunt syndrome may develop(Facial
paralysis ,vesicle ,tinnitus & vertigo)
Nervous Intermedius (Geniculate) Neuralgia
Management:
-High dose of steroid for 2-3weeks.
-Acyclovir is significant in reduce the
duration.
-Anti convulsion ,Carbamezipine.
-Surgery: section of nerve intermedius.
Condition secondary to damage caused by
a cerebrovascular accident .
its is characterized by constant or paroxysmal
pain accompanied by sensory abnormalities ,
Treatment:
anticonvulsant ( Lamotrigine,Gabapentine)
sodium channel blocker(Mexiletine).
TCAs (Amitriptyline).
Short-term relief may be obtained with intra
venous lignocaine or propofol .
Note: the anticonvulsants are preferred
In about 50% of patient with Bell's palsy,
pain occur in or near the ear but sometimes
spreading down the jaw, either precedes or
develops at the same time as the facial
palsy.
Treatment: prednisolone 60-80 mg per day,
acyclovir.
Constant dull aching pain , deep ,diffuse
variable intensity in absence of identifiable
organic disease.
Its more common in female .
Most patient middle age and elderly .
Clinical features:
Often difficult for patients to describe their symptoms .
Most frequently described as deep , constant ache or
burning .
Doesn't awake patient.
Doesn't follow anatomical pattern and may be
bilateral.
Affect maxilla more than mandible.
Often initiated or exacerbated by dental treatment .
Examination entirely normal .
Often have other complaints such as IBS ,dry mouth and chronic pain syndrome .
Treatment :
Often rewarded with limited response.
Tricyclic antideprssant drugs have some
effect in some patients .
30% of patient respond to Gabapentine
Cognitive behavior therapy
occurs most frequently in women in the fourth and
fifth decades of life,
constant dull, aching pain without an apparent
cause that can be detected by examination ,
it occur after dental extraction or endodontic
treatment ,
Period of pain free after secondary dental
management.
Atypical odontalgia(phantom)
-Management:
patient reassurance ,consultation to
other specialty
-T.C.A. like amitriptyline , nortriptyline at
low dose. 10 -25 mg at night
-Anti convulsant drugs.
Burning sensation of oral mucosa , usually
tongue, in absence of any identifiable
clinical abnormality or cause.
Epidemiology: 5 per 100,000 ,higher in
middle age and elderly, affect female
more than male .
Causes: unknown but hormonal factors ,
anxiety ,and stress have been implicated.
Burning mouth syndrome
Complain of dry mouth with altered or
bad taste.
Burning sensation affecting tongue ,
anterior palate and less common lips.
May be aggravated by certain foods.
Usually bilateral.
Doesn't awake patient . But may present at
awaking
Examination entirely normal .
Investigation: FBC ,haematinics ,swab for Candida .
Treatment: Reassurance .
Avoidance of stimulating factors.
Some patients may respond to TCA, SSRIs
topical clonazepam, sucking and spitting 1 mg three times daily for 2 weeks.
2-month course of 600 mg daily alfa-lipoicacid.
Cognitive behavior therapy.
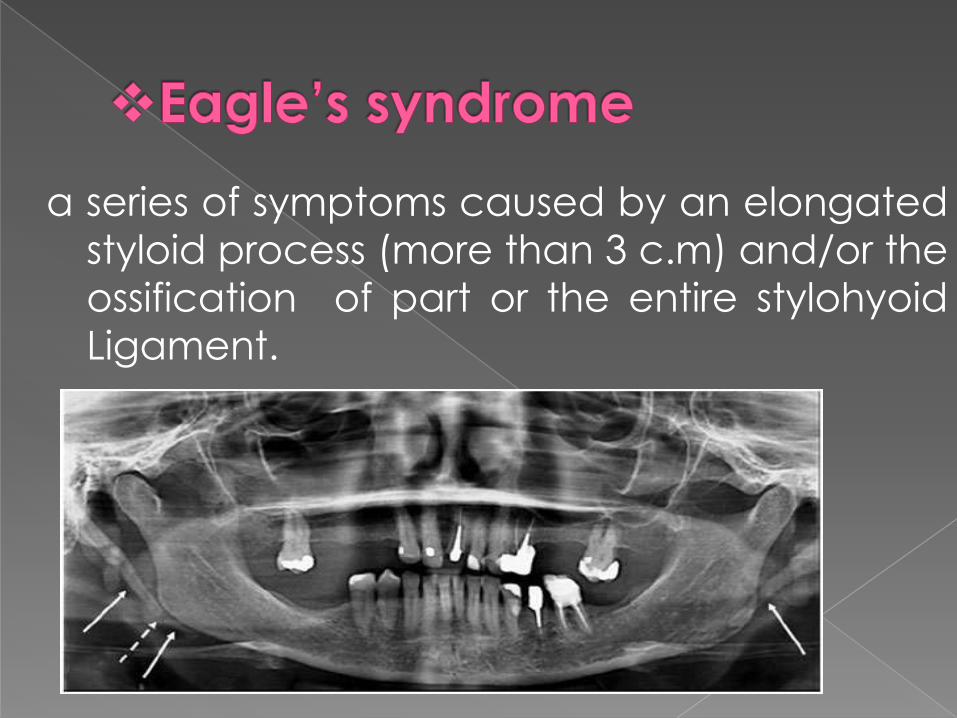
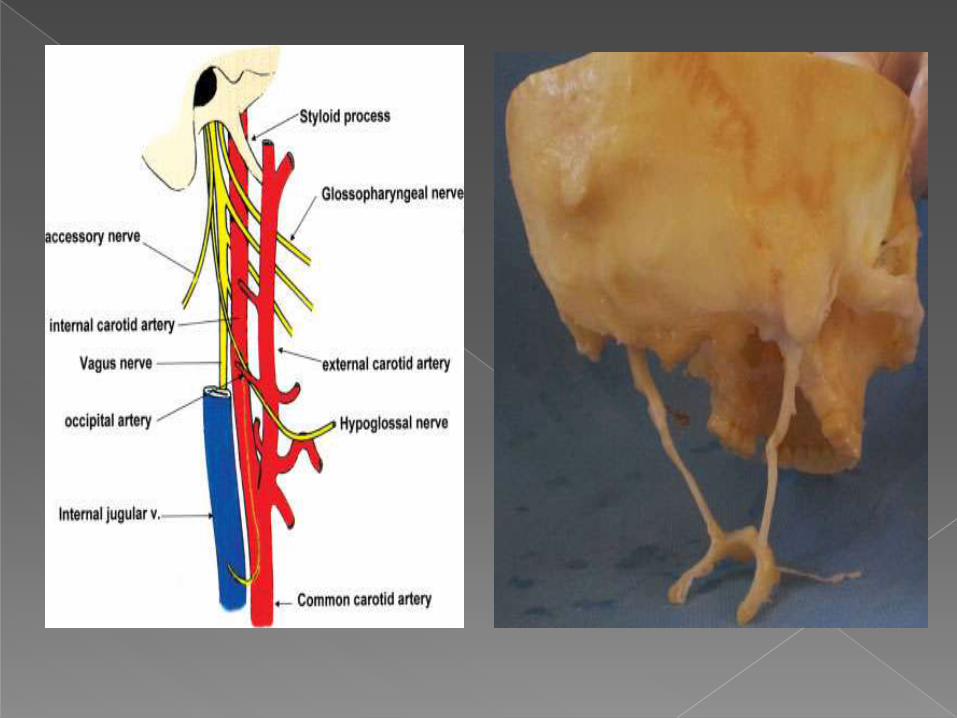
a series of symptoms caused by an elongated
styloid process (more than 3 c.m) and/or the
ossification of part or the entire stylohyoid
Ligament.
1-Classic :
the symptoms are persistent pharyngeal
pain aggravated by swallowing and
frequently radiate to the ear , with sensation
of foreign body within pharynx , This pain
arise following tonsillectomy due to
development of scar tissue around the tip of
the styloid process.
2- stylo-carotid artery syndrome(vascular):
Attributed to impingement of the carotid artery by
the styloid process This can cause a compression
when turning the head resulting in a transient
ischemic accident or stroke.
3-Traumatic Eagle syndrome:
in which symptoms develop after fracture of a
mineralized stylohyoid ligament.
(1)clinical manifestations,
(2) digital palpation of the process in the tonsillarfossa,
(3) radiological findings .
(4) lidocaine infiltration test.
Treatment:COSERVATIVE: involves injecting steroids
or long-lasting anesthetics into the lesser cornu of
the hyoid or the inferior aspect of the tonsillar fossa
I,NSAID
Surgical: intra oral or extra oral styloidectomy
Before puberty , female more than male .
Aura may developed before headache in 40%.
It may be triggered by foods such as nuts, chocolate, and red wine ; stress; sleep deprivation; or hunger.
Migraine
A-classic migraine (start with prodromal aura occurring over 20-30 minutes )
Flashing lights
Scotoma (localized area of vision depression )
Sensitivity to light
Sensory and motor deficit
Aura is followed by severe unilateral throbbing pain. Headaches may last for hours or up to 2 or 3 days.
B-common migraine (not preceded by aura)
Severe unilateral throbbing pain
Sensitivity to light and noise
Nausea and vomiting
30-50 years of age.
Pain last for minutes to hours and recurs several times per week.
Throbbing pain of neck and jaw.
Patients often seek dental consultation,
Tenderness of carotid artery
D-Basilar migraine : The symptoms are primarily neurologic and
include aphasia,temporary blindness, vertigo, confusion, and ataxia.
may be accompanied by an occipital headache.
Treatment :
Avoid trigger factors
Acute attack: analgesics, Sumatriptan (5-HT
agonist) , Ergotamin.
Prophylaxis : pizotifen ,propranolol , ca channel
blockers . TCAs
Clinical Manifestations: 80%of patients with CH are men.
The attacks are sudden, unilateral, and stabbing
,causing patients to pace, cry out, or even strike
objects. Some patients exhibit violent behavior
during attacks. pain as a hot metal rod in or around the eye.
Each attack lasts from 15 minutes to 2 hours and
recurs several times daily.
A majority of the painful episodes occur at night,
often awaking the patient from sleep.
Clinical Manifestations: The pain is associate nasal congestion and tearing
Sweating of the face, ptosis, increased salivation,
and edema of the eyelid. Cluster headache produce pain in posterior
maxilla that mimic dental pain.
Trigger by alcohol.
Treatment:
An acute attack: 100% oxygen (its effectiveness is diagnostic), Injection
of sumatriptan or sublingual or inhaled ergotamine
Prophylaxis : lithium, ergotamine, prophylactic
prednisone, and calcium channel blockers.
is believed to be a form of CH that occurs
predominantly in women between the ages of 30
and 40 years.
The episodes of pain tend be shorter, but attacks
of 5 to 20 minutes’ duration can occur up to 30
times daily.
It responds dramatically to therapy with
indomethacin , which stops the attacks within 1to 2
days.
-Its inflammation(vasculitis) of cranial arterial
tree.secondary to giant cell granulomatous.
Clinical features: most frequently affects adults above the age of
50 years.
Dull aching or throbbing temporal pain. accompanied by generalized symptoms , including fever, malaise, and loss of appetite.
Jaw claudication during mastication.
Diagnosis:
elevated ESR 50-100 .
elevated CRP.
Biopsy.
-Treatment:
high dose of steroid(prednisolone) 60 -100mg daily.
the steroid is tapered once the signs of the disease are controlled.
Patients are maintained on systemic steroids for 1 to 2 years after symptoms resolve.
1-Burket,s oral medicine.
2-Neville , Oral & Maxillofacial PATHOLOGY
3-Fonseca Oral and Maxillofacial surgery.
4- Booth Oral & Maxillofacial surgery.
5-Lecture notes in oral and maxillofacial surgery.
6- Orofacial pain ,from basic to management
References

THANK YOU