Embed Size (px)
Citation preview

OPTICS OF EYES 2

CYLINDRICAL LENS BENDS LIGHT RAYS IN ONLY ONE PLANE- COMPARISION WITH SPHERICAL
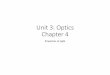
LENSES• The following diagram shows both a convex spherical
lens and a convex cylindrical lens.• The cylindrical lens bends light rays from the two
sides of the lens but not from the top or the bottom; that is bending occurs in one plane but not the other. Thus, parallel light rays are bent to a focal line.
• Light rays that pass through the spherical lens are refracted at all edges of the lens (in both planes) towards the central ray and all the rays come to a focal point.

A, point focus of parallel light rays by a spherical convex lens. B, line focus of parallel light rays by a cylindrical convex lens.

COMBINATION OF TWO CYLINDRICAL LENSES AT RIGHT ANGLES EQUALS A SPHERICAL LENS
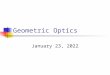
• The following diagram shows two convex cylindrical lenses at right angles to each other.
• The vertical cylindrical lens converges the light rays that pass through the two sides of the lens, and the horizontal lens converges the top and bottom rays.
• Thus all the light rays come to a single point focus. In other words, two cylindrical lenses cross at right angles to each other perform the same function as one spherical lens of the same refractive power.

A, focusing of light from a point source to a line focus by a cylindrical lens. B, Two cylindrical convex lenses at right angles to each other, demonstrating that one lens converges light rays in one plane and the other lens converges
light rays in the plane at a right angle. The two lenses combined give the same point focus as that obtained with a single spherical convex lens.

FOCAL LENGTH OF A LENS
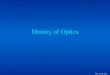
The upper most diagram• The distance beyond a convex lens at which
parallel rays converge to a common focal point is called focal length of the lens. The following diagram the top one demonstrates this focusing of parallel light rays.

FOCAL LENGTH OF A LENS
Middle diagram• The light rays that enter the convex lens are not
parallel but are diverging because the origin of light is a point source not far away from the lens itself.
• Because these rays are diverging outwards from the point source, it can be seen from the diagram that they do not focus at the same distance away from the lens as do parallel rays.

Middle diagram
• In other words, when rays of light that are already diverging enter a convex lens, the distance of focus on the other side of lens is farther from the lens than is the focal length of the lens for parallel rays.
FOCAL LENGTH OF A LENS

FOCAL LENGTH OF A LENS
The bottom diagram• This diagram shows light rays that are diverging
toward a convex lens that has far greater curvature than that of the other two lenses in the other two diagrams. In this diagram, the distance from the lens at which the light rays come to focus is exactly the same as that from the lens in the first diagram in which the lens has less curvature but the rays entering it are parallel.

FOCAL LENGTH OF A LENS
The bottom diagram• This demonstrates that both parallel rays and
diverging rays can be focused at the same distance beyond a lens, provided the lens changes its convexity.

The two upper lenses of this figure have the same focal length, but the light rays entering the top lens are parallel, whereas those entering the middle lens are diverging ; the effect of parallel verses diverging rays on
the focal distance is shown. The bottom lens has far more refractive power than either of the other two lenses (i.e., has a much shorter focal
length), demonstrating that the stronger the lens is, the nearer to the lens the point focus is.

ERRORS OF REFRACTION
• These are conditions in which vision is defective due to some fault in the; refractive medium especially;
i. The cornea or ii. The lens or iii. When there is an abnormality of the eyeball.

ERRORS OF REFRACTION
• Light rays from an object situated more than 6 meters (20 feet) are considered to be parallel.
• Light rays coming from an object closer than 6 meters are divergent.
• Emmetropic eye (the eye with normal refractive power)
This means that with relaxed accommodation parallel rays from infinity are focused on the retina where an image is produced.

ERRORS OF REFRACTION
The image is f focused to b real, inverted and diminished. The connections of retinal receptors are such that although the image of the object produced on the retina is inverted (upside down), but the object is seen in its true form (upside up).the mind is trained to consider an inverted image as normal.
With relaxed accommodation light rays from an object less than 6 meters from the eye will be focused behind the retina and therefore the object will be seen as a blurred object.

ERRORS OF REFRACTION
Normally the lens becomes more globular under these conditions by the process called accommodation. This results in a raised diopteric power of the eye and the image of the object can be produced on the retina.
• The non- emmetropic eye is called ammetropic eye and this condition lead to various errors of refraction which are described below;

ERRORS OF REFRACTION
MYOPIA, (NEAR SIGHTEDNESS)• The patient complains of difficulty in seeing distant objects
which appear blurred.• In this case the image of a distant object is focused in front
of the retina. It results;i. Either from an increased anterior posterior axial length of
the eye (axial myopia) orii. The eyeball is normal but the refractive power of the eye
is increased (refractive myopia). The refractive power of the eye may be due to an increased curvature of cornea or lens.

MYOPIA, (NEAR SIGHTEDNESS)iii. In some cases the lens is present anterior to the normal position. The result is that a point will focus on the retina not as a point but as a round spot.• Near vision is not as defective as distant
vision. This is because the diverging rays from a nearby object are focused behind the focus of parallel rays from a distant object. Myopia is therefore also called near sightedness.

Clinical types of myopia1. Congenital (present at birth)2. Developmental (precocious neurological
growth, nutritional disorders and excessive dose work involved in activities such as studies during childhood).
3. Drugs including sulfonamides and steroids.4. It is also seen in diabetes mellitus and in children who are made to sleep in lighted rooms before the age of two.

Treatment of myopia• Myopia is treated with concave lenses of
suitable strength which diverge light rays before they strike the cornea; this enables the light rays to focus on the retina. Contact lens is an ideal substitute in high myopia.

Hypermetropia (hyperopia, far sightedness).• In this case the subject’s distance vision
is better than near vision. However, the distant vision of a hypermetrope is poorer than a normal person.

Hypermetropia (hyperopia, far sightedness).• The image of the near object is focused
somewhere behind the retina.• Hypermetropia may be axial (the eyeball is
smaller resulting in decreased axial length) or refractive (decreased refractive power of the eye).
• If hypermetropia is slight, it may be compensated by accommodation which by increasing the diopteric power of the lens may result in focusing the rays of light on the retina.

Hypermetropia (hyperopia, far sightedness).• However, even accommodation may not
succeed in compensating the visual defect for close vision as the image of diverging light rays from a close object is produced too much behind the retina.
• The constant accommodation may lead to hypertrophy of ciliary body and the subject may complain of headache.

Hypermetropia (hyperopia, far sightedness).• The prolonged convergence of a visual axes
associated with accommodation may lead to strabismus (squint).
• All new born infants have hypermetropia of +4 diopter but the eyeball grows rapidly after birth resulting in disappearance of this defect in most children

Hypermetropia (hyperopia, far sightedness).• Delayed development of eyeball will result in
the persistence of hypermetropia. The child complains of frontal and occipital headache.
• Aphakia (removal of the lens) also results in a decreased diopteric power of eye.

Treatment of hypermetropia• It is treated with suitably powered convex
lenses placed extraocularly (spectacles) or intraocularly.


ASTIGMATISM( A= not ; stigma= Point)As the name suggests this is a refractive
error of vision.
In Astigmatism the light rays are not
brought to a point of focus on the retina.
The focus for horizontal rays different from that
for vertical rays.
Hence an astigmatic person looking at a piece of
graph paper may focus on the vertical lines and
may fail to focus the horizontal line and vice versa.
The defect is mostly due to a difference in
the horizontal and vertical curvatures of the cornea.,
occasionally the same abnormality affects the lens.

Astigmatism is of two types(i) With the rule : the curvature is greater
in vertical meridian it is more common.
(ii) Against the rule . The curvature is greater in horizontal meridian
Treatment ( Correction)
It is corrected with cylindrical glasses which have the property of bending the light rays in one plane more than in the other so that refraction in all meridians is equalized.



PRESBYOPIA ( Eyesight of old age)
> It is not an error of refraction but condition of physiological insufficiency of accommodation leading to failing vision for near.> Since, we usually keep the book at about 25cm, so we can read comfortably up to the age of 40 years.> after the age of 40 years, the near point of accommodation recedes beyond the normal reading or working range > This condition of failing near vision due to age related decrease in the amplitude of accommodation or increase in punctum proximum is called persbyopia.

Presbyopia accurs due to;1. Decrease in the elasticity and plasticity of
the crystalline lens ( which results from age- related sclerosis)
2. Age- related decrease in the power of ciliary muscles
Symptoms.Difficulty in near vision ( to start with in the evening & in dim light and later even in good light )
Treatment. ( Correction)Convex glasses (plus) for near vision.

THE END