Embed Size (px)
DESCRIPTION
Citation preview

NUCLEAR MEDICINE:OVERVIEW
Jiraporn Sriprapaporn, M.D.Division of Nuclear Medicine
Department of RadiologySiriraj Hospital

What is What is NNuclear uclear MMedicineedicine??
Nuclear medicine is a medical specialty which uses very small amount of a radioactive substance or a chemical compound labelled with a radioactive substance, called “radiopharmaceutical” or “radiotracers” to image or treat diseases.

NUCLEAR MEDICINENUCLEAR MEDICINE

RADIONUCLIDE THERAPYRADIONUCLIDE THERAPY
ThyroidHyperthyroidismDTC
Myeloproliferative diseasesPolycythemia vera
Joint effusion (RA)
I-131
P-32
Y-90

RADIONUCLIDE THERAPYRADIONUCLIDE THERAPY
Bone metastases
Malignant PheoNeuroblastomaCarcinoid tumoursMTC
Lymphoma
Sr-89, Sm-153EDTMP, Re-186 HEDP
I-131 MIBG
Y-90 Zevalin, I-131 BEXXAR

DIAGNOSTIC NUCLEAR MEDICINEDIAGNOSTIC NUCLEAR MEDICINE
Radionuclide imaging Rdn. non-imaging
Planar gamma camera Uptake tests
SPECT Absorption tests
SPECT/CT Whole body counter
PET Surface counting
PET/CT Breath tests

NM NM atat SirirajSiriraj HospitalHospital
THYROID
NM IMAGING
Dx
Rx

THYROIDTHYROID
Thyroid function testsIn-vitro TFT: serum T3, T4, FT3*, FT4, TSH, Tg*, TgAb**In-vivo TFT: RAIU, thyroid scan, I-131 TBS
Radionuclide therapy of thyroid diseases
HyperthyroidismDifferentiated thyroid cancer (DTC)

AnatomyAnatomy
2 lobes connecting with “isthmus”Anterior to 2nd-4th tracheal rings- C5-T1 vertebraeThyroid tends to increase weight with age (N=20g)Arteries: Superior, inferior thyroid A.Veins: Superior, middle, &inferior thyroid V.

HistologyHistology
Follicular cells: secrete hormones- T3(triidothyronine), T4(thyroxine)
Parafollicular cells (C-cells): secrete hormone-calcitonin
Colloid
F
MTC
DTC

Thyroid Thyroid PhysiologyPhysiology
HypothalamicHypothalamic--pituitarypituitary--thyroid axisthyroid axis
HYPOTHALAMUS
PITUITARY GLAND
THYROID
T3,T4
TRH
TSH
feedback

Thyroid Function
Kondo T, et al. Nature Reviews Cancer 6, 292-306 (April 2006)

Thyroid Hormone SynthesisThyroid Hormone Synthesis
Iodide trapping - into follicular cells Organification - Tyrosine + I-
inactive iodotyrosines: 3-monoiodotyrosine (MIT) & 3,5-diido tyrosine (DIT). incorporated into Tg &stored as colloid.Coupling
MIT + DIT T3DIT + DIT T4
Proteolysis or release - proteolysis of Tg produces the active hormones T4 & T4, then secreted into the blood.
Peroxidase

Common Thyroid DisordersCommon Thyroid Disorders
Thyroid nodules: Solitary vs multipleHypothyroidism: Congenital & acquiredHyperthyroidism
Graves’ diseaseToxic adenomaMultinodular toxic goiter (Plummer’s disease)
ThyroiditisAcuteSubacute (painful)Chronic Hashimoto’s thyroiditis (painless)
Thyroid malignancies : DTC, MTC, Others

Thyroid Function TestsThyroid Function Tests
ININ--VITRO VITRO TTFTFT
ININ--VIVO VIVO TTFTFT

InIn--vitro vitro TTFTFT
T3, FT3*T4, FT4TSH: primary hypothyroidism*Tg*: tumor marker of DTCTgAb** (thyroglobulin Ab)Antimicrosomal Ab (Thyroid peroxidase Ab-TPOAb)Thyroid stimulating hormone receptor Ab -TRAb
Total form = bound form + free form

InIn--vivo vivo TTFTFT
RAIU: overall thyroid gland function
Perchlorate discharge test : Organificationdefect
Thyroid scan: Evaluate thyroid nodules
I-131 TBS: Evaluate DTC patients

Patient PreparationPatient Preparation
RAIU & Thyroid scan: DiscontinueThyroid hormone medications > 2 wksAntithyroid drug > 1 wk ( for I-131)
I-131 Total-body scan (TBS): Thyroid hormone: 50 ug OD for 4 wks & discontinued for 2 wks

RAIU: IndicationsRAIU: Indications
Equivocal invitro TFTDDx hyperthyroidism vs subacutethyroiditisThyroid remnant evaluation (PO.)Pre RAI treatment for hyperthyroidism

Factors Interfering RAIUFactors Interfering RAIU
Iodine load*Iodide-containing drugs eg. Amiodarone, KI in cough remedy, BetadinePrevious contrast studies eg. CT, IVP 4-6 wksSea food or iodine-containing food/supplements

2424--hrhr.. Radioactive Iodine UptakeRadioactive Iodine Uptake
Hypothyroid
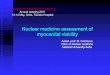
Typical Curves of 24-hr Radioiodine Uptake
Normal
Hyperthyroid
Hours after tracer dose I-131 24 hr
%Uptake 80
0
Rapid Turnover
Normal 24 hr RAIU = 15-45%

Rapid TurnoverRapid Turnover
Isaacson, et al. Rapid turnover of I-131 in subpopulations of hyperthyroid patients: A retrospective data analysis. J Nucl Med. 2009; 50 (Supplement 2):1304 [from NC, USA]N= 963 patientsOnly 4 % had rapid turnover.Uptake at 4 hr/ uptake at 24 hr > 1

Perchlorate Discharge TestPerchlorate Discharge Test
Aim: To identify organificationdefects, most commonly involving the peroxidase enzyme.
Dyshormonogenesis
Indications:Enlarged thyroid gland with hypothyroid or elevated TSHPendred’s syndrome:familial goiter and hearing loss

Perchlorate Discharge TestPerchlorate Discharge Test
Discharge < 5%Normal, no org.defect
Discharge > 5%Positive for org.defect

Thyroid scan & TBS will be discussed in the section of NM imaging.

RRAIAI TreatmentTreatment ffororThyroid DisordersThyroid Disorders
HYPERTHYROIDISMHYPERTHYROIDISMGravesGraves’’ diseasediseaseToxic adenomaToxic adenomaMultinodular toxic goiterMultinodular toxic goiter
THYROID CANCERTHYROID CANCERDTCDTC

RAI TREATMENT FOR RAI TREATMENT FOR HYPERTHYROIDISMHYPERTHYROIDISM

IndicationsIndications
Failed medical/surgical treatment-relapseSerious adverse effects of antithyroid drugs: drug allergy, agranulocytosisInconvenience for frequent contactPoor socioeconomic problemsPresence of serious associated medical illness eg. heart failure

Procedures for RAI TreatmentProcedures for RAI Treatment
Discontinue antithyroid drug for 5-7 daysMeasure 24 hr RAIU I-131 dose calculation for Rx depending on gland size, RAIU, dose of I-131 (uCi) /gram thyroid tissue [100-200 uCi/gram]
RAI Dose = [Thyroid mass (g) x 80-200 uCi/gm]/% uptake

Post RAI TreatmentPost RAI Treatment
Symptomatic-beta blockersAntithyroid drug: start after 7 days as required.Follow up q 1-2 monthsBlood test for T3, T4, TSH as required and when hypothyroid is suspected.Rx hypothyroid by replacement therapyRepeat RAI Rx 3-6 months interval

RAI TREATMENT RAI TREATMENT FOR DTCFOR DTC

RAI Treatment RAI Treatment ffor DTCor DTC
Papillary thyroid carcinoma
Follicular thyroid carcinoma
Both are derived from follicular cells.

Treatment Treatment ofof DTCDTC
SurgeryNear-total /total thyroidectomy
RAI TreatmentHormonal treatment
Suppressive dose of thyroid hormone (T4)to keep TSH 0.1-0.4 mIU/L.
Long-term follow-upERT#

Revised ATA Guidelines for Differentiated Thyroid Cancer
http://www.thyroid.org/professionals/publications/documents/ATA_Guidelines_DTC_2009.pdf

RAI TreatmentRAI Treatment
No invasive properties or metas. 100 mCiInvasive properties 150 mCiLN met 150 mCiLung met 150 mCiBone met 200 mCi

Patient PreparationPatient Preparation
First visit Evaluation of residual thyroid tissue (PO 7+
days without thyroid hormone at least 2 wks)• Thyroid scan • RAIU • (T4, TSH, Tg, TgAb)
Schedule for admission after 4-6 weeks PO. without thyroid H med or prepare as I-131 TBS.

FollowFollow--up up ofof DTC PtsDTC Pts..
Clinical history & physical examinationBlood Tests
Thyroid hormones levels (TSH 0.1-0.4 mIU/L)Tumor marker ie. Tg (N < 1 ng/ml) & TgAb (N< 40 mIU/L)Calcium balance, CBC
I-131 TBS at 6- 12 mo post Rx until negative*(*also other parameters are negative)
Other investigations eg. CXR-yearly, Tl-201, Tc-99m MIBI scan, U/S, CT scan, MRIRepeat RAI Rx: at least 6-12 months interval

NUCLEAR MEDICINE IMAGING
Jiraporn Sriprapaporn, M.D.Division of Nuclear Medicine
Department of RadiologySiriraj Hospital

SScopecope ofof NM INM Imagingmaging
Endocrinology : Thyroid scan, Parathyroid scanCardiovascular system : Myocardial perfusion scan,Radionuclide venographyGenitourinary system : Renogram, Testicular scan,Radionuclide cystographyPulmonary system : Perfusion/ Ventilation lung scanSkeletal system : Bone scanGastrointestinal system : Liver scan, Hepatobiliary scan,GE reflux studyTumor imaging : Ga-67 scan for Lymphoma, I-131 scan for pheochromocytoma, Tc-99m MIBI for parathyroid adenoma

Radiopharmaceutical
Patient
Gamma Camera
Images
Principle Principle oof Nf NMM ImagingImaging

RadiopharmaceuticalRadiopharmaceuticalss
A radioactive material in a form suitable for administration to a human for the purposes of therapy or diagnostic investigation

Radioisotopes eg. I-131, Tc-99m
Radiolabeled compounds eg. Tc-99m MDP for Bone scan, Tc-99m MAA for Lung scan [distribution // compounds]1 Organ Many R’pharmaceuticals1 R’pharmaceutical Many organs
A B
RadiopharmaceuticalRadiopharmaceuticalss

AtomsAtoms
Atoms of all elements are composed of known p, n, & eNuclides containing same no. of 'p'(atomic no. = Z) but different 'n'Isotopes eg. I-123, I-131Isotopes have the same chemical but different physical properties.

Physical PropertiesPhysical Properties
Physical half life
Type of radiation emitted
Energy of radiation emitted
Physical property is characteristic of each radioisotope.!

Source Source oof Production f Production oof Radionuclidesf Radionuclides
Reactor Radionuclides contain excess neutron.Cyclotron Radionuclides contain deficient neutron.Generator

GeneratorGenerator--produced Radionuclidesproduced Radionuclides
Parent Radionuclide Daughter Radionuclide Decay product
99Mo 99mTc 99Tc113Sn 113mIn 113In81Rb 81mKr 81Kr195mHg 195mAu 195Au191Os 191mIr 191Ir115Cd 115mIn 115In87Y 87mSr 87Sr90Sr 90Y 90Zr68Ge 68Ga 68Zn82Sr 82Rb 82Kr

CyclotronCyclotron--producedproduced RadionuclidesRadionuclides(for SPECT)(for SPECT)
TlTl--201201
GaGa--6767
II--123123
InIn--111111

Radionuclides Used Radionuclides Used iin Nn NMM
Radionuclides used in NM emit beta or gamma radiationBeta minus particles easily absorbed in tissue suitable for therapyGamma rays more readily transmitted through tissue, allow external measurement &imaging by gamma cameraBeta plus particles allow PET imagingfollowing the "annihilation"

PositronPositron--emitting Radionuclidesemitting Radionuclides
Radionuclides T1/2C-11 20 min.N-13 10 min.O-15 2 min.F-18 110 min.Ga-68 68 min.Rb-82 75 sec

CheapAvailablePure gamma emitterOptimal gamma energy (100-200 keV) * 140Optimal half life *6 hrSafeChemically active
* Tc-99m is the most ideal agent !
Ideal Properties Ideal Properties oof Radioisotopesf Radioisotopes

Specific Uptake of TcSpecific Uptake of Tc--9999mm
Thyroid glandSalivary glandsGastric mucosaChoroid plexus

Planar gamma camera
SPECT or SPETSPECT or SPET =Single Photon Emission (Computed) TomographySPECT/CT
PETPET = Positron Emission TomographyPET/CT
InstrumentsInstruments

PET/CTPET/CT

DISCOVERY PET/CT_GEDISCOVERY PET/CT_GE

PET & PET/CT ImagingPET & PET/CT Imaging
PET:Metabolic imagingUsing positron emitter radionuclidesBiological tracers (C-N-O-F)More sensitiveBetter imageWhole body evaluation

Advantages Advantages oof Nf NMM StudiesStudies
Functional*SensitiveQuantitativeVery safeNot too expensiveMinimally invasiveLow radiation exposureScreeningFollow-up

Disadvantages Disadvantages oof Nf NMM StudiesStudies
Not widely availableGive minimal radiationGenerally non-specificRequire NM instrument &radiopharmaceuticalsRelatively more expensive than routine X-ray or U/S

Radiation ProtectionRadiation Protection
To decrease radiation doses from unselaed sources of radionuclides by ……..
1. shielding & avoiding contamination2. increasing distance from the source3. limiting time of exposure

Important TopicsImportant Topics
Which organ imaging?Uses or indications?Which R’pharm can be used? Route?What is the mechanism of uptake?What is the appropriate pt preparation?Technique of imaging procedure
Imaging acquisition protocol (positioning-views)(Processing) & Image display
InterpretationNormal: Normal distribution?Abnormal: DDx?


Mechanisms Mechanisms oof Localizationf Localization
1. Capillary blockade: Tc-99m MAA lung scan2. Diffusion : Tc-99m DTPA brain scan3. Sequestration : Ht. denatured RBC , labelled plt.4. Phagocytosis : Tc-99m sulfur colloid liver scan5. Active transport : Iodide, pertechnetate, Tl, OIH,
IodoCH, IDA6. Compartmental localization : labelled RBC, SC for GI
studies7. Physicochemical adsorption : Tc-99m MDP bone scan8. Ag-Ab reaction : labelled MoAb9. Others and unknown

Imaging TechniquesImaging Techniques
Static vs dynamic imagingPlanar vs SPECT imagingWhole-body imagingImaging views: anterior, posterior,RAO, LAP, RPO, LPO, LL, RLMarkers: hot & cold

Image AcqusitionImage Acqusition
Preset countPreset time: dynamicCombined

Image ProcessingImage Processing
Dynamic imaging: renalSPECT imaging: tumor, brain, cardiac

Image DisplayImage Display
Black on whiteWhite on blackColors
Adjust intensity !!
Not too dark and not too light !!

Practical IssuesPractical Issues
Radiation protection at all timesPrepare yourself about the tests before hands.Check the indications, appropriate?Any precaution or specific patient preparation required?Patient history taking & making note (LAB)Relevant physical examinationDouble check for correct dose preparationCorrect R’pharm administrationCheck the images before the patient leaveCheck the quality and quantity of the films and report paper imagesAsk the attending staff if you feel uncertain.Read the scan when it’s done.






![Nuclear Physics in Medicine - · PDF fileNuclear Physics in Nuclear Physics in Medicine 2013 NuPECC medicine – Chapter 1 - Hadrontherapy [HADRONTHERAPY] Draft – for internal use](https://img.pdfslide.us/doc/110x75/5a802f987f8b9ada388c139d/nuclear-physics-in-medicine-physics-in-nuclear-physics-in-medicine-2013-nupecc.jpg)

















