Embed Size (px)
DESCRIPTION
Nicotine improves cognitive performance and modulates neuroplasticity in brain networks
Citation preview

Title: Nicotinergic impact on focal and non-focal neuroplasticity induced by non-invasive brain
stimulation in non-smoking humans
Authors: Nivethida Thirugnanasambandam MBBS,M.Tech1, Jessica Grundey MD 1, Kim
Adam1, Anne Drees1, Angela C. Skwirba1, Nicolas Lang MD 2, Walter Paulus MD 1, Michael A.
Nitsche MD 1*
Author affiliation: 1Department of Clinical Neurophysiology, Georg-August-University
Goettingen, Robert-Koch-Strasse 40, 37075 Goettingen, Germany; 2 Department of Neurology,
Christian-Albrechts University, Kiel, Germany.
Running title: Nicotinergic impact on neuroplasticity
Number of pages: 28
Figures: 4; Tables: 1; Supplementary material: 1 Table
Number of words:
Abstract: 200
Introduction: 498
Materials and methods: 1456
* Corresponding author:
Prof. Dr. Michael A. Nitsche,
Address same as above.
Email: [email protected]; Phone: +49 55139957; Fax: +49 551398621

Nicotinergic impact on neuroplasticity Nitsche MA
- 2 -
Abstract
Nicotine improves cognitive performance and modulates neuroplasticity in brain networks. The
neurophysiological mechanisms underlying nicotine-induced behavioral changes have been
sparsely studied, especially in humans. Global cholinergic activation focuses plasticity in
humans. However, the specific contribution of nicotinic receptors to these effects is unclear.
Henceforth, we explored the impact of nicotine on non-focal neuroplasticity induced by
transcranial direct current stimulation (tDCS) and focal, synapse-specific plasticity induced by
paired associative stimulation (PAS) in healthy non-smoking individuals. Forty eight subjects
participated in the study. Each subject received placebo and nicotine patches combined with one
of the stimulation protocols to the primary motor cortex in different sessions. Transcranial
magnetic stimulation (TMS) - elicited motor evoked potential (MEP) amplitudes were recorded
as a measure of corticospinal excitability until the evening of the second day following the
stimulation. Nicotine abolished or reduced both PAS- and tDCS-induced inhibitory
neuroplasticity. Non-focal facilitatory plasticity was also abolished, whereas focal facilitatory
plasticity was slightly prolonged by nicotine. Thus, nicotinergic influence on facilitatory, but not
inhibitory plasticity mimics that of global cholinergic enhancement. Therefore, activating
nicotinic receptors has clearly discernable effects from global cholinergic activation. These
nicotine-generated plasticity alterations might be important for the effects of the drug on
cognitive function.
Keywords: neuroplasticity, nicotine, paired associative stimulation, transcranial direct current
stimulation, transcranial magnetic stimulation

Nicotinergic impact on neuroplasticity Nitsche MA
- 3 -
Introduction
Smoking tobacco is the single largest preventable cause of mortality and morbidity (Peto et al.
1992). Nicotine is the primary constituent of tobacco that is responsible for its addictive
properties. Nicotine is the classical agonist at nicotinic acetylcholine receptors (nAchRs) which
are ligand-gated cation channels. Studies in animals and humans have shown that nicotine
improves attention as well as working and long-term memory (Froeliger et al. 2009; Hahn and
Stolerman 2002; Kumari et al. 2003). While many studies focused on the behavioral effects of
nicotine in healthy humans and patients (Jacobsen et al. 2004; Sacco et al. 2005), very few have
investigated the nicotinergic impact on cortical excitability and plasticity, which are the likely
neurophysiological basis for the cognitive effects of the substance. For global cholinergic
enhancement, it was shown that cholinesterase-inhibitors reduce intracortical inhibition, increase
facilitation, and enhance focal, but diminish non-focal facilitatory plasticity in healthy humans
(Korchounov et al. 2005; Kuo et al. 2007). A study on tobacco smokers, who are under chronic
nicotine exposure, revealed enhanced motor cortex inhibition and reduced facilitation (Lang et
al. 2008). Nicotine also enhances and prolongs the facilitatory after-effects of intermittent theta
burst stimulation in human motor cortex (Swayne et al. 2009). Thus, global cholinergic and
nicotinergic activation might have at least partially dissimilar effects on cortical excitability.
Transcranial direct current stimulation (tDCS) and paired associative stimulation (PAS) are non-
invasive brain stimulation techniques that induce neuroplastic cortical excitability alterations
(Nitsche and Paulus 2000, 2001; Nitsche et al. 2003a; Stefan et al. 2000; Wolters et al. 2003).
Both techniques induce NMDA- and calcium-dependent changes of cortical excitability (Nitsche
et al. 2003b; Stefan et al. 2002; Wolters et al. 2003). tDCS modulates spontaneous neuronal

Nicotinergic impact on neuroplasticity Nitsche MA
- 4 -
activity and excitability by either depolarizing or hyperpolarizing neurons. Anodal tDCS induces
depolarization that enhances neuronal excitability whereas cathodal tDCS hyperpolarizes
neurons, decreasing their excitability levels (Nitsche and Paulus 2000, 2001; Nitsche et al.
2003a). Since tDCS affects all neurons beneath the electrodes, it is thought to induce relatively
non-focal plasticity. PAS, on the other hand, induces focal, synapse-specific, timing-dependent,
associative neuroplasticity in the targeted neurons. Here an electrical pulse to a mixed peripheral
nerve at an intensity which activated somatosensory fibres is followed by a suprathreshold
magnetic pulse applied to the corresponding area of the primary motor cortex. Depending on the
interstimulus interval, there occurs synchronous or asynchronous activation of somatosensory-
motor cortical connections that enhance or reduce excitability respectively (Stefan et al. 2000).
In the current study we aimed to identify the specific contribution of nicotinic receptors to the
cholinergic effect on focal and non-focal neuroplasticity by exploring the effects of nicotine on
tDCS- and PAS-generated plasticity in healthy non-smoking humans to improve our
comprehension of the cognition-enhancing and addictive properties of this substance. As in the
foregoing studies, the motor cortex was taken as a model system in this single blinded, placebo-
controlled, partial crossover study because it allows a convenient monitoring of excitability
alterations by measuring motor evoked potential (MEP) amplitudes via transcranial magnetic
stimulation (TMS).
Materials and methods
Subjects
Forty eight healthy human volunteers participated in the study. All of them were complete non-
smokers, that is, none of them had smoked tobacco for at least 3 years prior to the study. They

Nicotinergic impact on neuroplasticity Nitsche MA
- 5 -
did not suffer from any chronic or acute medical illness or any history of neurological/psychiatric
diseases, and did not take any chronic or acute medication. This information was obtained by a
detailed free personal interview with the subjects. Pregnancy, family history of epilepsy,
presence of any metallic implant or cardiac pacemaker was ruled out. All of them were right-
handed according to the Edinburgh handedness inventory (Oldfield, 1971). The selection of
subjects was not based on their results from previous plasticity experiments in our laboratory;
most of them were naïve to the experimental procedure. Table 1 shows the demographic
characteristics of the different groups. All subjects gave written informed consent before
participating in the study. The experiments were approved by the local Ethics Committee and
conformed to the Declaration of Helsinki. Allocation of the subjects to the respective
experimental conditions as well as order of sessions was randomized.
_____________________________________________________________________________
Insert Table 1 here
______________________________________________________________________________
Assessing motor cortex excitability
Single transcranial magnetic (TMS) pulses were delivered from a Magstim 200 stimulator
(Magstim Company, Whitland, Dyfed, UK) at a frequency of 0.25 Hz with a figure-of-eight
shaped coil (diameter of one winding, 70mm; peak magnetic field, 2.2 T). The coil was held
tangentially to the scalp at an angle of 45º to the sagittal plane with the coil handle pointing
laterally and posterior. This induced a postero-anterior current flow in the brain at an angle that
optimally activates the corticospinal system monosynaptically (Di Lazzaro et al., 1998). Motor
evoked potentials (MEPs) were recorded using a surface electromyogram (EMG) set-up. Surface

Nicotinergic impact on neuroplasticity Nitsche MA
- 6 -
EMG electrodes (Ag-AgCl) were placed over the abductor digiti minimi muscle (ADM) in a
belly-tendon montage. Signals were amplified, band-pass filtered (2Hz - 2KHz), digitized
(5KHz) and stored in a laboratory computer for offline analysis using Signal software and CED
1401 (Cambridge Electronic Design, Cambridge, UK). MEPs were elicited using single pulse
TMS over the motor cortex representation of the ADM. The position of the coil on the scalp,
where the stimulus elicited consistently the largest MEP amplitudes for slightly suprathreshold
intensity was marked as the motor ‘hotspot’. Stimulus intensity was then adjusted in order to
obtain peak to peak MEP amplitudes of approximately 1mV (SI1mV). This TMS intensity was
kept constant throughout the experiment. The mean MEP amplitude was calculated from at least
20 pulses for baseline, and post-intervention excitability monitoring. The change of the mean
MEP amplitude over time reflects alterations of motor cortex excitability.
Transcranial direct current stimulation
Twenty four subjects participated in the tDCS experiments. tDCS was administered by a battery-
driven constant current stimulator (Schneider Electronic, Gleichen, Germany) through rubber
electrodes covered by saline soaked sponges (35 square cm). One electrode was placed over the
motor cortex representation of the right ADM as determined by single pulse TMS and the other
electrode over the contralateral supra-orbital region. All subjects received 1mA of either anodal
(for 13 min) or cathodal stimulation (for 9 min), combined with nicotine or placebo medication
in different experimental sessions. Therefore, twelve subjects received anodal tDCS with
nicotine or placebo patches and the remaining twelve received cathodal tDCS with nicotine or
placebo patches. This stimulation intensity and duration (13 min anodal tDCS and 9 min
cathodal tDCS) generates after-effects on cortical excitability lasting for approximately 60 min

Nicotinergic impact on neuroplasticity Nitsche MA
- 7 -
after stimulation (Nitsche and Paulus 2001; Nitsche et al. 2003a). The two consecutive
experimental sessions per subject were separated by at least one week interval.
Paired associative stimulation
Twenty four subjects participated in the PAS experiment. Here a peripheral electrical pulse over
the right ulnar nerve at wrist level was followed by a TMS pulse over the motor cortex
representation of the ADM at inter-stimulus intervals (ISI) of either 10 (PAS 10) or 25
milliseconds (PAS 25). The peripheral pulse was delivered from a Digitimer D185 multipulse
stimulator (Digitimer, Welwyn Garden City, UK) at an intensity of 300% of the sensory
perceptual threshold. The suprathreshold magnetic pulse was delivered from a Magstim 200
stimulator with an intensity which elicited MEP amplitudes of approximately SI1mV. The paired
pulses were repeated 90 times at a frequency of 0.05 Hz. This protocol induces long-lasting
excitability changes in the motor cortex depending on the ISI duration. An ISI of 10 ms induces
excitability diminution whereas an ISI of 25 ms induces facilitation (Stefan et al. 2000; Wolters
et al. 2003). The subjects were instructed to count the number of pulses they received at their
wrist throughout the whole stimulation duration in order to guarantee sufficient attention to the
procedure, which has been shown to be crucial to obtain the intended effects (Stefan et al., 2004).
Pharmacological intervention
Each subject participated in two sessions in randomized order. 30cm2 nicotine transdermal
patches, each containing nicotine 0.83mg/cm2 releasing 15mg over 16 hours or placebo patches
were administered to all subjects in combination with one of the stimulation protocols - anodal
tDCS, cathodal tDCS, PAS-10 or PAS-25. By this dosage of nicotine, physiologically and

Nicotinergic impact on neuroplasticity Nitsche MA
- 8 -
behaviorally relevant plasma levels are accomplished (Tønnesen et al. 1991). Subjects received
the patch 6 hours before the start of the stimulation. This was the approximate time for the
plasma level of nicotine to reach its maximum following application of the patch (Nørregaard et
al. 1992). The patch was retained until the end of the last after-measurement of the experiment
on the evening of the second day. In order to counteract possible systemic side effects of
nicotine, the subjects were instructed to take 20mg domperidone, a peripheral acting dopamine
D2-receptor antagonist with antiemetic effects, in case of need.
Course of the experiment
The subjects received either a placebo or nicotine patch, which was adhered to the left upper arm
and remained there until the end of the last after-measurement on the following evening. They
were given 20mg domperidone and asked to take it orally in case of any side effects.
Unpublished results from our group show that domperidone alone does not have any significant
effect on motor cortical excitability. Six hours later, subjects were seated comfortably in a
reclined position on a dentist´s chair with proper arm and head rests and asked to relax
completely. The EMG electrodes were placed at the right ADM as described above. The motor
‘hotspot’ was determined over the left motor cortex and marked with a water-proof skin marker,
and the TMS intensity needed to induce MEP amplitudes of 1mV (SI1mV) size was determined.
Twenty MEPs were recorded at this stimulus intensity and the mean MEP amplitude was
calculated as the baseline. One of the stimulation protocols, either tDCS or PAS, was
administered. At least 20 MEPs were recorded immediately following the stimulation (0min) and
at time points of 5, 10, 15, 20, 25, 30, 60, 90, and 120 min. For the nicotine patch sessions, the
after-measurements were also conducted in the evening of the stimulation day and in the

Nicotinergic impact on neuroplasticity Nitsche MA
- 9 -
morning and evening of the day following the plasticity induction procedure. We used a
waterproof pen to mark the ADM electrodes and TMS coil positions and ensured that these were
positioned over the same spot during the whole course of the experiment.
_____________________________________________________________________________
Insert Figure 1 here
______________________________________________________________________________
Data analysis and statistics
The individual means of the 20 MEP amplitudes recorded at each time point were calculated for
all subjects. The post-intervention mean MEP amplitudes from each subject were then
normalized to the respective individual mean baseline MEP amplitude. The normalized mean
MEP amplitudes from all subjects were pooled together and the grand average across subjects for
each time bin was calculated.
A repeated measures ANOVA was performed on the normalized data using MEP amplitude as
the dependent factor including all time points up to 120 min after stimulation. Drug (Nicotine
versus Placebo) and time points were included as within-subjects factors. Stimulation (anodal
tDCS/ cathodal tDCS/ PAS-10/ PAS-25) served as between-subjects factors. The Mauchly test
was performed to test for sphericity, and the Greenhouse-Geisser correction applied when
necessary. Conditional on significant results of the ANOVA, we performed post-hoc
comparisons using Student’s t-tests (paired, two-tailed, p<0.05, not adjusted for multiple
comparisons) where we compared (i) the mean MEP amplitudes at the time points after plasticity
induction versus baseline and (ii) the mean MEP amplitudes following nicotine versus placebo at
one time point within a stimulation condition. Moreover, we compared absolute baseline MEP

Nicotinergic impact on neuroplasticity Nitsche MA
- 10 -
values between the stimulation and drug conditions via Student´s t-tests to exclude a priori
differences. Chi square test was performed to look for significant differences in gender
distribution between the groups. For comparison of the age of subjects between the groups,
Student’s t-tests (two - tailed, unpaired, p<0.05) were performed.
Results
All subjects tolerated the experimental procedure well. None of them complained of any side
effects of either nicotine or the stimulation. Especially the participants did not complain of any
sedative effects of the patch. During the experiment, they were completely alert and relaxed.
Since no systemic side effects of nicotine were perceived and none of the participants needed to
take domperidone, the subjects were blinded effectively. Gender distribution did not differ
significantly between the various groups tested by chi square test (p = 0.083). There were
significant differences in the mean age between some of the groups as tested by Student’s
unpaired t-tests. However, the maximum difference of mean age between groups was 2.65 years.
Absolute baseline MEP amplitudes did not differ significantly between groups (Student’s t-test,
two-tailed, paired, p>0.05 for all cases) or medication conditions (Student’s t-test, unpaired, two-
tailed, p = 0.66).
The ANOVA revealed a significant main effect of the between-subjects factor stimulation
(F(3,44) = 18.137; p < 0.001), in accordance with different effects of inhibitory and facilitatory
tDCS and PAS on MEP amplitudes. The main effects of either nicotine (F(1,44) = 0.093; p =
0.762) or time (F(10,440) = 1.654; p = 0.089) were not significant. However, the interactions
between nicotine X stimulation (F(3,44) = 5.498; p = 0.003); time X stimulation (F(30,440) =

Nicotinergic impact on neuroplasticity Nitsche MA
- 11 -
3.070; p < 0.001) were significant, showing that nicotine had different effects on the above-
mentioned stimulation protocols, and that the time course of the effects of these stimulation
protocols was not identical. The three-way interaction nicotine X time X stimulation (F(30,440)
= 1.848; p = 0.005) was also significant. Thus, application of nicotine patch significantly
influenced the after-effects of the different stimulation protocols differently over time.
Nicotinergic impact on tDCS-induced plasticity
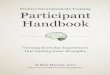
As shown by the post hoc t-tests, in the control condition without nicotine, MEPs were
significantly enhanced following anodal tDCS for up to 90 minutes. Cathodal tDCS diminished
excitability levels significantly also for up to 90 minutes after stimulation. Under nicotine, both
anodal and cathodal tDCS-induced after-effects were abolished. The post-hoc test revealed that
for anodal tDCS, post-tDCS MEP amplitudes under nicotine were not different from baseline
values, but differed significantly from those under placebo medication (table S1). A trendwise
reversal of the effects of anodal tDCS from facilitation to inhibition under nicotine did not reach
statistical significance (p > 0.073). The excitability diminution induced by cathodal tDCS, as
compared to baseline excitability, was also abolished under nicotine; however relative to the
placebo medication condition nicotine induced only a trendwise change (Figure 2 A, B, table
S1).
_____________________________________________________________________________
Insert Figure 2A and 2B here
______________________________________________________________________________

Nicotinergic impact on neuroplasticity Nitsche MA
- 12 -
Effect of nicotine on PAS-induced plasticity
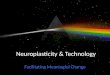
As shown by the post hoc tests, PAS induced a significant facilitation of MEP amplitudes
following PAS-25 and excitability diminution following PAS-10, lasting for up to 90 or 120
minutes after stimulation (table S1) under placebo medication. Under nicotine, the facilitatory
effects of PAS-25 remained significant as compared to the respective baseline MEP for up to 90
min after PAS. MEP amplitudes under nicotine did not differ versus the respective placebo
medication condition for up to 90 min after PAS-25, but were significantly larger as compared to
placebo 120 min after PAS-25, being in favor for a prolonged excitability enhancement
accomplished by PAS-25 under nicotine. The missing difference of PAS-25 under nicotine
relative to baseline excitability 120 min after placticity induction might be caused by the
relatively large variability of the MEPs at this time point (see Table S1). The inhibitory effect of
PAS-10 was abolished under nicotine. Consequently, the post hoc tests revealed no significant
differences of the respective MEP amplitudes relative to baseline, but significant differences of
the respective MEP amplitudes relative to those under placebo medication (figure 3A, B).
_____________________________________________________________________________
Insert Figure 3A and 3B here
______________________________________________________________________________
Discussion
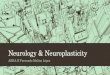
The present study shows that in healthy non-smoking individuals nicotine prominently affects
neuroplasticity. Our data illustrate that (i) nicotine exposure slightly prolongs or at least
preserves the synapse-specific cortical excitability enhancement induced by PAS-25, but

Nicotinergic impact on neuroplasticity Nitsche MA
- 13 -
abolishes the PAS-10 induced depression of cortical excitability (ii) the non-focal excitability
enhancing after-effect of anodal tDCS and the excitability diminution caused by cathodal tDCS
are both abolished (Figure 4). There is also a trendwise reversal of anodal tDCS - induced
facilitation to inhibition under nicotine. Hence, we observe a focusing effect of nicotine on
facilitatory neuroplasticity and an abolishment of inhibitory plasticity, the latter irrespective of
the focality of stimulation.
_____________________________________________________________________________
Insert Figure 4 here
______________________________________________________________________________
Some of our observations match with those of previous studies. The enhancement or preservation
of facilitatory plasticity induced by PAS-25 by nicotine is similar to the effect it had on
intermittent theta burst stimulation (Swayne et al., 2009). The effect of nicotine on facilitatory
plasticity is also comparable to the effect of the cholinesterase inhibitor rivastigmine on identical
plasticity induction protocols, however its effects on inhibitory plasticity are at variance to those
under global cholinergic enhancement under rivastigmine (Kuo et al., 2007).
Proposed mechanism of action
The focusing effect of nicotine on facilitatory plasticity, i.e. consolidating/preserving focal, PAS-
induced, but diminishing non-focal tDCS-generated plasticity, is quite similar to that of global
cholinergic enhancement via rivastigmine described in a previous study (Kuo et al., 2007). A
likely explanation for this effect is the different impact of cholinergic activation on recurrent
activation of afferent input to cortical neurons. It has been shown that excitatory glutamatergic

Nicotinergic impact on neuroplasticity Nitsche MA
- 14 -
synaptic transmission is suppressed by presynaptic inhibition at intrinsic, recurrent synapses, but
not at afferent fibre synapses via cholinergic activation (Hasselmo & Bower, 1992; Hasselmo et
al., 1995; Vogt & Regehr, 2001). Since PAS induces plasticity by a combination of afferent
somatosensory input with a motor cortical stimulus, while tDCS is thought to affect primarily
excitability of cortical interneurons (Nitsche et al., 2005), it might be speculated that these
specific aspects of the stimulation techniques caused the differences of the effects also in the
present experiments. In accordance, in animal experiments an inhibitory effect of the activation
of nicotinergic subreceptors on feedforward interneurons has has been shown to prevent LTP
induction by inhibiting pyramidal neurons, whereas spike-timing dependent LTP was enhanced
(Rosza et al., 2008; Yamazaki et al., 2005), although the latter effect was not shown in all studies
(Couey et al., 2007). Due to the results of the present experiment, this effect of cholinergic
activation on facilitatory plasticity in humans can likely be attributed to an impact of nicotinic
receptors. Another possible explanation of the results is based on the enhancement of
intracellular calcium concentration by nicotinic receptors, e.g. the alpha-7 subreceptor.
Intracellular calcium is a key determinant of plasticity induction, and the after-effects of tDCS
and PAS are calcium-dependent (Nitsche et al., 2003b; Stefan et al., 2002). The amount of
intracellular calcium determines if inhibitory, facilitatory, or no plasticity is induced. A slight
enhancement of intracellular calcium induces LTD, a large enhancement LTP (Lisman, 2001).
Medium and very large concentrations of intracellular calcium induce no or convert plasticity,
the latter possibly due to an activation of hyperpolarizing calcium channels (Misonou et al.,
2004). Since tDCS induces facilitatory plasticity by tonic depolarization of neurons for some
minutes, which might activate voltage-dependent calcium channels, whereas PAS is a phasic
stimulation technique, which induces only short lasting depolarization, the amount of

Nicotinergic impact on neuroplasticity Nitsche MA
- 15 -
intracellular calcium increase caused by tDCS might be larger than that caused by PAS.
Therefore, a further calcium enhancement via nicotinic receptor activation might enhance the
calcium level above the concentration inducing LTP-like plasticity, and therefore result in an
abolishment of plasticity in case of tDCS, but not PAS. This effect on different kinds of
facilitatory plasticity of nicotine might enhance the signal-to-noise ratio (Hasselmo and Barkai,
1995), which would facilitate the representation of meaningful, synchronous inputs and suppress
non-meaningful inputs. Indeed, it has been recently suggested that nicotine improves memory
performance via calcium-dependent mechanisms in animals (Biala & Kruk, 2009).
In contrast, nicotine abolished all kinds of inhibitory plasticity irrespective of the specific
stimulation protocol. One possible explanation might be that the calcium-enhancing properties of
nicotinic receptor activation here resulted in an intracellular calcium level too large to induce
LTD-like plasticity. This mechanism of action would also explain the different effect of global
cholinergic activation by rivastigmine on inhibitory plasticity, as described in a previous study,
where this substance prolonged tDCS- and PAS-generated inhibitory plasticity (Kuo et al.,
2007), because muscarinic receptors inhibit voltage-gated calcium channels (Brown, 2010), and
thus might counteract the effects of nicotinic receptors in this case. The effects of nicotine on
inhibitory plasticity obtained in the present study are not in accordance with some animal
experiments, where nicotinic activation has been shown to be important for LTD induction
(Partridge et al., 2002; Fujii & Sumikawa, 2001), however, the effect of nicotine on LTD seems
to depend on the general proneness of the system to inhibitory plasticity (Alzoubi et al., 2007,
2008), which likely differs between animal preparations and in vivo studies in humans.
It should be mentioned that these mechanistic explanations of the results are hypothetical
presently. Alternative explanations, such as the modification of NMDA receptor-dependent

Nicotinergic impact on neuroplasticity Nitsche MA
- 16 -
plasticity by nicotine-dependent alteration of GABAergic activity (Couey et al. 2007), cannot be
ruled out. These hypotheses should be tested more directly in future studies, e.g. by altering the
activity of nicotinic subreceptors, or calcium channels, in combination with nicotine exposure.
General remarks
The results of the present study demonstrate that nicotine clearly influences neuroplasticity in
non-smoking individuals. Nicotine focuses facilitatory plasticity whereas it abolishes inhibitory
plasticity. The effects differ from those of non-specific cholinergic activation. The focusing
effect of nicotine on facilitatory plasticity might help to explain how this drug improves
attention, working memory and long-term memory in animals and humans via enhancing the
signal to noise ratio of plasticity. Also the abolition of inhibitory plasticity by nicotine might
affect cognitive processes. First, it might shift the net balance of plasticity more into the direction
of facilitatory plasticity, and therefore indirectly enhance cognitive performance further. Second,
inhibitory plasticity, especially long-term depression (LTD) has been shown to be directly
involved in certain forms of learning and memory formation. Collingridge and colleagues (2010)
describe a role of LTD in hippocampal-based learning and memory formation, and recognition
memory in perirhinal cortex. Since our findings show that nicotine abolishes LTD-like plasticity
it could be speculated that nicotine might worsen LTD-dependent forms of learning and memory.
However, an impairment of cognitive functions by nicotine has been rarely described (Toledano
et al., 2010), thus further behavioral studies are needed to explore the cognitive effects of
nicotine more systematically.
Some limiting aspects of this study should be mentioned. Blinding could have been somewhat
compromised considering the fact that the experimenters were not blinded to the intervention.

Nicotinergic impact on neuroplasticity Nitsche MA
- 17 -
However, the data were collected by more than one investigator without notable difference in the
results, which probably indicates low experimenter bias, and experimenters were not informed
about hypotheses about expected outcomes of the experiments, which should have limited
expectancy effects. Although the subjects did not complain of any sedation due to nicotine, the
degree of alertness was not explicitly assessed and hence its effect on the measurements cannot
be ruled out completely. We did not measure plasma concentrations of nicotine, thus it could be
argued that inter-individual differences of the bioavailability of the substance had an impact on
the results. However, since we studied a fairly homogenous group of participants, and we
induced plasticity during steady state drug concentration, we do not think that variability of
plasma concentration of nicotine can explain the results. We studied the effect of only a single
dosage of nicotine in the present experiments. Thus it cannot be ruled out that the effect of
nicotine on plasticity differs dose-dependently, as shown for other neuromodulators, like
dopamine (Monte-Silva et al. 2009, 2010). Moreover, since nicotine receptors are rapidly
modified by chronic exposure, this study cannot discern between primary effects of nicotine on
nicotinic receptors and secondary effects caused by receptor desensitization or upregulation.
Moreover, it should not be taken for granted that the effects obtained on motor cortex plasticity,
as in the current study, translate exactly to other cortices, where nicotinic receptor density, and
subreceptor composition might differ (McGehee and Role, 1995; Gotti et el., 2009) Furthermore
the results of a single dosage nicotine application in non-smokers, as performed here, might
differ from the effects of nicotine in smokers who are chronically exposed to it. Future studies
should address these aspects in larger detail.

Nicotinergic impact on neuroplasticity Nitsche MA
- 18 -
Conclusion
The results of this study deliver clear evidence for an important role of nicotine in the formation
of neuroplasticity, the likely basis of learning and memory formation, in humans. Via its
focusing effect on facilitatory plasticity, nicotine might be an attractive candidate to enhance
these processes in neuropsychiatric diseases accompanied by cognitive decline. The abolition of
inhibitory plasticity by nicotine also could have a significant impact on some forms of learning
and memory, and also affect addictive behavior to some extent. Moreover, its effect on plasticity
might be an important mechanism for starting nicotine consumption, addiction and the high
probability of relapse in smokers. Interestingly the effects of nicotine on plasticity share some of
those of dopamine (Kuo et al., 2008), which might be an explanation for the frequent nicotine
consumption in schizophrenia, in which dopaminergic malfunctioning is an important pathologic
mechanism. Clearly, more studies are needed to explore the exact role of nicotine in healthy
humans and in those suffering from neuropsychiatric diseases to a larger degree. Moreover the
results of this study are important in another aspect. Non-invasive brain stimulation techniques
are increasingly used as scientific and therapeutic tools. The results of the present study show
that the activity of the nicotinergic system might critically affect the effects of brain stimulation.
This potentially important confounding factor should thus be taken into account in future studies
using brain stimulation.
Disclosure/Conflict of interest
The authors declare that, except for income received from my primary employer, no financial
support or compensation has been received from any individual or corporate entity over the past

Nicotinergic impact on neuroplasticity Nitsche MA
- 19 -
three years for research or professional service and there are no personal financial holdings that
could be perceived as constituting a potential conflict of interest.
Funding:
The study was supported by the Deutsche Forschungsgemeinschaft (DFG grant NI683/4-1
‘Towards risk prediction of nicotine dependency by exploring individual limits of cortical
neuroplasticity in humans’; NI 683/4-2 “Impact of the nicotinergic alpha7 receptor on cortical
plasticity in smokers and nonsmokers”) within the DFG priority program ‘Nicotine: Molecular
and Physiological Effects in Central Nervous System’.
Supplementary information is available at the Neuropsychopharmacology website.

Nicotinergic impact on neuroplasticity Nitsche MA
- 20 -
References
Alzoubi KH, Aleisa AM, Alkadhi KA. (2007). Adult-onset hypothyroidism facilitates and
enhances LTD: reversal by chronic nicotine treatment. Neurobiol Dis. 26(1):264-72.
Alzoubi KH, Aleisa AM, Alkadhi KA. (2008). Effect of chronic stress or nicotine on
hypothyroidism-induced enhancement of LTD: electrophysiological and molecular studies.
Neurobiol Dis. 32(1):81-7.
Biała G, Kruk M. (2009). Influence of bupropion and calcium channel antagonists on the
nicotine-induced memory-related response of mice in the elevated plus maze. Pharmacol Rep.
61(2):236-44.
Brown DA. (2010). Muscarinic acetylcholine receptors (mAChRs) in the nervous system: some
functions and mechanisms. J Mol Neurosci. 41:340-346.
Couey JJ, Meredith RM, Spijker S, Poorthuis RB, Smit AB, Brussaard AB, Mansvelder HD.
(2007). Distributed network actions by nicotine increase the threshold for spike-timing-
dependent plasticity in prefrontal cortex. Neuron. 54(1):73-87.
Di Lazzaro V, Oliviero A, Profice P, Saturno E, Pilato F, Insola A, Mazzone P, Tonali P,
Rothwell JC. (1998). Comparison of descending volleys evoked by transcranial magnetic and
electric stimulation in conscious humans. Electroencephalogr Clin Neurophysiol. 109(5):397-
401.

Nicotinergic impact on neuroplasticity Nitsche MA
- 21 -
Froeliger B, Gilbert DG, McClernon FJ. (2009). Effects of nicotine on novelty detection and
memory recognition performance: double-blind, placebo-controlled studies of smokers and
nonsmokers. Psychopharmacology (Berl). 205(4):625-33.
Fujii S, Sumikawa K. (2001). Nicotine accelerates reversal of long-term potentiation and
enhances long-term depression in the rat hippocampal CA1 region. Brain Res. 894(2):340-6.
Gotti C, Clementi F, Fornari A, Gaimarri A, Guiducci S, Manfredi I, Moretti M, Pedrazzi P,
Pucci L, Zoli M. (2009). Structural and functional diversity of native brain neuronal nicotinic
receptors. Biochem Pharmacol. 78(7):703-11.
Hahn B, Stolerman IP. (2002). Nicotine-induced attentional enhancement in rats: effects of
chronic exposure to nicotine. Neuropsychopharmacology. 27(5):712-722.
Hasselmo ME, Barkai E. (1995). Cholinergic modulation of activitydependent synaptic plasticity
in the piriform cortex and associative memory function in a network biophysical simulation. J
Neurosci. 15:6592– 6604.
Hasselmo ME, Bower JM. (1992). Cholinergic suppression specific to intrinsic not afferent fiber
synapses in rat piriform (olfactory) cortex. J Neurophysiol 67:1222–1229.
Hasselmo ME, Schnell E, Barkai E. (1995). Dynamics of learning and recall at excitatory
recurrent synapses and cholinergic modulation in rat hippocampal region CA3. J Neurosci
15:5249 –5262.

Nicotinergic impact on neuroplasticity Nitsche MA
- 22 -
Jacobsen LK, D'Souza DC, Mencl WE, Pugh KR, Skudlarski P, Krystal JH. (2004). Nicotine
effects on brain function and functional connectivity in schizophrenia. Biol Psychiatry.
55(8):850-858.
Korchounov A, Ilic TV, Schwinge T, Ziemann U. (2005). Modification of motor cortical
excitability by an acetylcholinesterase inhibitor. Exp Brain Res. 164(3):399-405.
Kumari V, Gray JA, ffytche DH, Mitterschiffthaler MT, Das M, Zachariah E, Vythelingum GN,
Williams SC, Simmons A, Sharma T. (2003). Cognitive effects of nicotine in humans: an fMRI
study. Neuroimage. 19(3):1002-1013.
Kuo MF, Grosch J, Fregni F, Paulus W, Nitsche MA. (2007). Focusing effect of acetylcholine on
neuroplasticity in the human motor cortex. J Neurosci. 27(52):14442-7.
Kuo MF, Paulus W, Nitsche MA. (2008). Boosting focally-induced brain plasticity by dopamine.
Cereb Cortex. 18(3):648-651.
Lang N, Hasan A, Sueske E, Paulus W, Nitsche MA. (2008). Cortical hypoexcitability in chronic
smokers? A transcranial magnetic stimulation study. Neuropsychopharmacology. 33(10):2517-
2523.
Lisman JE. (2001). Three Ca2+ levels affect plasticity differently: the LTP zone, the LTD zone
and no man's land. J Physiol. 532(Pt 2):285.
McGehee DS, Role LW. (1995). Physiological diversity of nicotinic acetylcholine receptors
expressed by vertebrate neurons. Annu Rev Physiol. 57:521-46.

Nicotinergic impact on neuroplasticity Nitsche MA
- 23 -
McKay BE, Placzek AN, Dani JA. (2007). Regulation of synaptic transmission and plasticity by
neuronal nicotinic acetylcholine receptors. Biochem Pharmacol. 74(8):1120-1133.
Misonou H, Mohapatra DP, Park EW, Leung V, Zhen D, Misonou K, Anderson AE, Trimmer
JS. (2004). Regulation of ion channel localization and phosphorylation by neuronal activity. Nat
Neurosci. 7(7):711-718.
Monte-Silva K, Kuo MF, Thirugnanasambandam N, Liebetanz D, Paulus W, Nitsche MA.
(2009). Dose-dependent inverted U-shaped effect of dopamine (D2-like) receptor activation on
focal and nonfocal plasticity in humans. J Neurosci. 29(19):6124-6131.
Nitsche MA, Paulus W. (2000). Excitability changes induced in the human motor cortex by weak
transcranial direct current stimulation. J Physiol. 527 (Pt 3):633-639.
Nitsche MA, Paulus W. (2001). Sustained excitability elevations induced by transcranial DC
motor cortex stimulation in humans. Neurology. 57(10):1899-901.
Nitsche MA, Fricke K, Henschke U, Schlitterlau A, Liebetanz D, Lang N, Henning S, Tergau F,
Paulus W. (2003a). Pharmacological modulation of cortical excitability shifts induced by
transcranial direct current stimulation in humans. J Physiol. 553(Pt 1):293-301.
Nitsche MA, Nitsche MS, Klein CC, Tergau F, Rothwell JC, Paulus W. (2003b). Level of action
of cathodal DC polarisation induced inhibition of the human motor cortex. Clin Neurophysiol.
114(4):600-604.
Nitsche MA, Seeber A, Frommann K, Klein CC, Rochford C, Nitsche MS, Fricke K, Liebetanz
D, Lang N, Antal A, Paulus W, Tergau F. (2005). Modulating parameters of excitability during

Nicotinergic impact on neuroplasticity Nitsche MA
- 24 -
and after transcranial direct current stimulation of the human motor cortex. J Physiol. 568(Pt
1):291-303.
Nørregaard J, Tønnesen P, Simonsen K, Säwe U. (1992). Long-term nicotine substitution after
application of a 16-hour nicotine patch in smoking cessation. Eur J Clin Pharmacol. 43(1): 57-60
Partridge JG, Apparsundaram S, Gerhardt GA, Ronesi J, Lovinger DM. (2002). Nicotinic
acetylcholine receptors interact with dopamine in induction of striatal long-term depression. J
Neurosci. 22(7):2541-9.
Peto R, Lopez AD, Boreham J, Thun M, Heath C Jr. (1992). Mortality from tobacco in
developed countries: indirect estimation from national vital statistics. Lancet. 339(8804):1268-
1278.
Rózsa B, Katona G, Kaszás A, Szipöcs R, Vizi ES. (2008). Dendritic nicotinic receptors
modulate backpropagating action potentials and long-term plasticity of interneurons. Eur J
Neurosci. 27(2):364-77.
Sacco KA, Termine A, Seyal A, Dudas MM, Vessicchio JC, Krishnan-Sarin S, Jatlow PI,
Wexler BE, George TP. (2005). Effects of cigarette smoking on spatial working memory and
attentional deficits in schizophrenia: involvement of nicotinic receptor mechanisms. Arch Gen
Psychiatry. 62(6):649-659.
Stefan K, Kunesch E, Cohen LG, Benecke R, Classen J. (2000). Induction of plasticity in the
human motor cortex by paired associative stimulation. Brain. 123 (Pt 3):572-584.

Nicotinergic impact on neuroplasticity Nitsche MA
- 25 -
Stefan K, Kunesch E, Benecke R, Cohen LG, Classen J. (2002). Mechanisms of enhancement of
human motor cortex excitability induced by interventional paired associative stimulation. J
Physiol. 543(Pt 2):699-708.
Swayne OB, Teo JT, Greenwood RJ, Rothwell JC. (2009). The facilitatory effects of intermittent
theta burst stimulation on corticospinal excitability are enhanced by nicotine. Clin Neurophysiol.
120(8):1610-5.
Toledano A, Alvarez MI, Toledano-Díaz A. (2010). Diversity and variability of the effects of
nicotine on different cortical regions of the brain - therapeutic and toxicological implications.
Cent Nerv Syst Agents Med Chem. 10(3):180-206.
Tønnesen P, Nørregaard J, Simonsen K, Säwe U. (1991). A double-blind trial of a 16-hour
transdermal nicotine patch in smoking cessation. N Engl J Med. 325(5):311-5.
Vogt KE, Regehr WG. (2001). Cholinergic modulation of excitatory synaptic transmission in the
CA3 area of the hippocampus. J Neurosci 21:75– 83.
Wolters A, Sandbrink F, Schlottmann A, Kunesch E, Stefan K, Cohen LG, Benecke R, Classen
J. (2003). A temporally asymmetric Hebbian rule governing plasticity in the human motor
cortex. J Neurophysiol. 89(5):2339-2345.
Wonnacott S. (1997). Presynaptic nicotinic Ach receptors. Trends Neurosci. 20(2):92-98.
Yamazaki Y, Jia Y, Hamaue N, Sumikawa K. (2005). Nicotine-induced switch in the nicotinic
cholinergic mechanisms of facilitation of long-term potentiation induction. Eur J Neurosci.
22(4):845-60.

Nicotinergic impact on neuroplasticity Nitsche MA
- 26 -
Table 1: Comparison of the subject characteristics of the four experiments. The table lists the
age and gender characteristics of the subjects who participated in the four different categories of
the experiment. Also the mean of the absolute baseline MEP amplitude values are shown.
Stimulation
Parameter
Anodal tDCS Cathodal
tDCS PAS 10 PAS 25
Number of subjects
12 12 12 12
Number (%) of females
6 (50) 7 (58.33) 6 (50) 6 (50)
Age of subjects (mean ± SD) in years
24.3±1.1 26.9±3.5 25.9±2.1 24.5±1.3

Nicotinergic impact on neuroplasticity Nitsche MA
- 27 -
Titles and legends to figures:
Figure 1
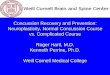
Illustration of the experimental design. Each subject underwent two experimental sessions. At
the beginning of the session, the subjects first received either a placebo or a nicotine patch. After
6 hours break, baseline (BL) motor evoked potentials (MEPs) of approximately 1 mV amplitude
were recorded by single pulse transcranial magnetic stimulation (TMS) over the motor cortical
representational area of the abductor digiti minimi muscle (ADM). One of the four stimulation
protocols (anodal tDCS/cathodal tDCS/PAS-25/PAS-10) was then applied. After-measurements
were made immediately following the stimulation and once every 5 min for the first 30 min, then
once every 30 min for 120 min for both sessions. In addition, MEPs were also recorded the same
evening, next morning and evening for the nicotine patch sessions.
Figure 2
Nicotinergic impact on transcranial direct current stimulation (tDCS) induced neuroplasticity.
Shown are the graphs with MEP amplitudes standardized to baseline on the Y-axis plotted
against various time points following the stimulation. (A) In the placebo condition (squares),
anodal tDCS enhances motor cortex excitability until 90 minutes following stimulation. This
effect of anodal tDCS is abolished in the nicotine condition (circles). (B) The cathodal tDCS-
induced excitability diminution observed in the placebo condition (squares) is also abolished by
application of nicotine (circles). Filled symbols indicate statistically significant deviations from
baseline and asterisks indicate significant differences between the control and nicotine conditions

Nicotinergic impact on neuroplasticity Nitsche MA
- 28 -
(Student’s t-test, paired, two-tailed, p<0.05). SE, same evening; NM, next morning; NE, next
evening; MEP, motor evoked potential. Error bars indicate S.E.M.
Figure 3
Nicotinergic impact on paired associative stimulation (PAS) induced neuroplasticity. The graphs
show baseline-standardized MEP amplitudes on the Y-axis plotted at different time points
following the stimulation. (A) In the placebo condition (squares), PAS-25 induced a clear
increase of MEP amplitudes lasting for 90 minutes after stimulation. With nicotine (circles), the
facilitatory after-effect of PAS-25 is slightly prolonged. (B) PAS-10 under placebo medication
(squares) induced a prominent decrease of MEP amplitudes significant until 90 minutes after
stimulation. Nicotine (circles) abolished the inhibitory after-effect of PAS-10. Filled symbols
indicate statistically significant deviations from baseline and asterisks indicate significant
differences between the control and nicotine conditions (Student’s t-test, paired, two-tailed,
p<0.05). SE, same evening; NM, next morning; NE, next evening; MEP, motor evoked potential.
Error bars indicate SEM.
Figure 4
Effect of nicotine on focal/non-focal neuroplasticity induced in the human motor cortex until 30
minutes following stimulation. Nicotine shows a focusing effect on facilitatory plasticity. Focal
facilitatory plasticity is prolonged, whereas non-focal facilitatory plasticity is abolished under
nicotine. Nicotine also abolishes any effect of excitability-reducing plasticity-generating
protocols. Each bar represents the mean MEP amplitude until 30 minutes after stimulation
standardized to the baseline. Error bars indicate S.E.M.