Embed Size (px)
DESCRIPTION
multiple pregnancy lecture
Citation preview

Multiple pregnancy for Multiple pregnancy for MRCOGMRCOG

Multiple birth UK 1995Multiple birth UK 1995
No. (Rate/1000 mats) No. (Rate/1000 mats) Ratio Ratio
TwinsTwins 9889 (13.6)9889 (13.6) 1 in 73 1 in 73
TripletsTriplets 318 (0.4)318 (0.4) 1 in 2282 1 in 2282
QuadsQuads 10 (0.0001)10 (0.0001) 1 in 72563 1 in 72563
TotalTotal 10217 (14)10217 (14) 1 in 71 1 in 71

Importance of chorionicity?Importance of chorionicity?
Chorionicity affects pregnancy risk:Chorionicity affects pregnancy risk: Fetal loss ratesFetal loss rates Cerebral palsy ratesCerebral palsy rates
Pregnancy risk assessmentPregnancy risk assessment Twin-twin transfusion syndromeTwin-twin transfusion syndrome Prenatal diagnosisPrenatal diagnosis
Chromosome abnormalityChromosome abnormalityStrucural abnormalityStrucural abnormality
Further schedule of surveillance based on Further schedule of surveillance based on chorionicity (?=delivery mode)chorionicity (?=delivery mode)

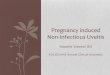
Prevalence death & cerebral palsy Prevalence death & cerebral palsy Western Australia 1980-1989Western Australia 1980-1989
15.6
70.5
92.8
1.67.4 26.7
0102030405060708090
100
per 1000 births
Deaths Cerebral palsy
Singleton
Twins
Triplets

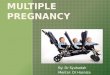
Fetal and Perinatal MortalityFetal and Perinatal Mortality
15
12
9
6
3
0
12.1%
1.8%
15
12
9
6
3
0 2.8% 1.6%
MonochorionicDichorionic
Fetal Loss (<24 weeks)
Perinatal Loss (>24 weeks)
Sebire N et al. BrJOG 1997

Presumed zygosity & cerebral palsy Presumed zygosity & cerebral palsy ((Western Austailia 1956-1985)Western Austailia 1956-1985)
ConcordantConcordant DiscordantDiscordant
MonozygoticMonozygotic 66 99
DizygoticDizygotic 00 2121
P=0.0026

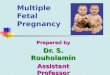
Chorionicity versus zygocityChorionicity versus zygocity
0-4 days
4-7 days
7-14 days
Fused or unfused

Dichorionic10%of all tw ins
33% of m onozygous
Diam niotic17% of all tw ins
56% of m onozygous
Conjoined tw ins0.15% of a ll tw ins0.5%m onozygous
M onoam niotic3% of all tw ins
10% of m onozygous
M onochorionic20%of all tw ins
67% of m onozygous
M onozygous30%of all tw ins(All like sexed)
All dichorionic70%of all tw ins
100% of dizygous
Dizygous70% of all tw ins(1/2 like sexed)
All tw ins

Early ultrasound appearancesEarly ultrasound appearances
Scans before 11 weeks Scans before 11 weeks common in AC pregnanciescommon in AC pregnancies
Chorionicity:Chorionicity: 2 clear sacs dichorionic2 clear sacs dichorionic ?1sac monochorionic?1sac monochorionic
Amnionicity:Amnionicity: UncertainUncertain Yolk sac numberYolk sac number
Dichorionic twins (7 weeks)Dichorionic twins (7 weeks)

Ultrasound diagnosis of chorionicityUltrasound diagnosis of chorionicity
“ “T” signT” signMONOCHORIONICMONOCHORIONIC
““Lambda” signLambda” signDICHORIONICDICHORIONIC

Twin-twin transfusion syndromeTwin-twin transfusion syndrome
25% MC twins will have 25% MC twins will have evidence of TTS at 15-17 evidence of TTS at 15-17 weeksweeks
50% 50% severe TTS severe TTS
Severe TTS 80-90% Severe TTS 80-90% mortalitymortality
Death will occur in both Death will occur in both babiesbabies
RecipientRecipient DonorDonor


Indicators of risk of TTTSIndicators of risk of TTTS
11-13 week scan11-13 week scan Discrepancy in CRLDiscrepancy in CRL Discrepancy in NTDiscrepancy in NT
Donor small NTDonor small NT
Receipient raised NTReceipient raised NT
16 week scan16 week scan Infolding of the Infolding of the
membranesmembranes Size discrepancySize discrepancy

Diagnosis of chronic TTTSDiagnosis of chronic TTTS
MonochorionicStuck twinPolyhydramniosGrowth discrepancyDopplerHydropsPROGRESSIVE*

Serial Amniodrainage
Multicentre Registry (Mari et al. 1998)
• 579 cases
• Survival 68%
• Abnormal neonatal head sonograms - 25%
• Normalise amniotic fluid volume• Improves uterine blood flow• Prevents premature labour

Fetoscopic Laser Ablation
Ville et al. 1998 BrJOGDiLia 1998 (TTTS website)
Non-selective
Laser Ablation
202 cases
59% Survival
4% neurological
handicap rate


FLA vs AmniodrainageFLA vs Amniodrainage
n=116, 17-25 weeks’ gestationn=43: Amniodrainage, Bonn;n=73: Laser ablation, Hamburg
Hecher K et al. 1999 AmJOG
Overall survival (NS)
61% 51%
FLA
Abnormal brain scan (p <0.03)
6% 18%
FLA
FLAAmnion Drainage
Gestation at delivery (p <0.02)
40
30
20
10
0
33.7 30.7

TTS in the 3rd trimester?TTS in the 3rd trimester?
REMEMBERREMEMBER
Chronic type TTSChronic type TTS
Acute “late onset” Acute “late onset” TTSTTS AntenatalAntenatal IntrapartumIntrapartum Delivery of twin 1Delivery of twin 1

Mono-amniotic twinsMono-amniotic twins
High mortality rates (upto 50%)High mortality rates (upto 50%)TTTS/Discordant growth unusualTTTS/Discordant growth unusualMonitor amniotic fluid volumeMonitor amniotic fluid volumeColour-flow doppler for cord entanglementColour-flow doppler for cord entanglementMonitoring of uncertain valueMonitoring of uncertain valueDelivery at 32-34 weeks?Delivery at 32-34 weeks?

Prenatal diagnosis in twinsPrenatal diagnosis in twins
ScreeningScreening Nuchal translucencyNuchal translucency Serum screeningSerum screening
Invasive diagnosisInvasive diagnosis Chorionic villous samplingChorionic villous sampling AmniocentesisAmniocentesis

Screening for aneuploidy in twinsScreening for aneuploidy in twins
Calculation of risksCalculation of risks For each fetusFor each fetus For the pregnancyFor the pregnancy
NT screeningNT screening
Biochemical screeningBiochemical screening
Risks of interventionRisks of intervention Invasive procedureInvasive procedure Selective fetocideSelective fetocide

Single puncture amniocentesisSingle puncture amniocentesis
Sebire et al 1996
Miscarriage risk 1-2%
Selective fetocide 8%+
Sample one sac in MC
Careful documentation

CVS in twinsCVS in twins
Single or double entrySingle or double entry Experienced operatorExperienced operator Careful documentationCareful documentation
Sample 1 placenta in Sample 1 placenta in MC twinsMC twinsMiscarriage risk Miscarriage risk 1-2%1-2%
Risk of selective fetocide Risk of selective fetocide 11-13 weeks 5%11-13 weeks 5%
CVS for “high risk”CVS for “high risk”

Twins and fetal abnormalityTwins and fetal abnormality
DichorionicDichorionic Same risk doubledSame risk doubled
MonochorionicMonochorionic ““Teratogenic” stimulusTeratogenic” stimulus Increased risk midline Increased risk midline
abnormalitiesabnormalities Not always cordantNot always cordant
Specific twin abnormalitiesSpecific twin abnormalities


Conjoined twinsConjoined twins

Acardiac twinningAcardiac twinning

Scanning schedule- normalScanning schedule- normal
MonochorionicMonochorionic12 weeks12 weeks16 weeks16 weeks20 weeks20 weeks24 weeks24 weeks27 weeks27 weeks30 weeks30 weeks33 weeks33 weeksDelivery 36 weeksDelivery 36 weeks
DichorionicDichorionic12 weeks12 weeks20 weeks20 weeks28 weeks28 weeks32 weeks32 weeks36 weeks36 weeksDelivery 38 weeksDelivery 38 weeks
Increased surveillance if evidence of TTTS or growth abnormality

Low birthweightLow birthweight
a Singleton
b Twins
c Triplets
d quads
52% twins (n=5416) <2500g compared 6% singletons (Regan 2001)

Delivery of pre-term twinsDelivery of pre-term twins
37

Elective delivery of twinsElective delivery of twins
0
2
4
6
8
10
12
14
16
28 29 30 31 32 33 34 35 36 37 38 39
Gestation (weeks)
Sti
llbir
th r
isk
pe
r 1
00
0 o
ng
oin
g p
reg
na
nc
ies
Sairam et al 2002

Delivery mode?Delivery mode?
ChorionicityChorionicity MonochorionicMonochorionic MononamnioticMononamniotic
Presentation and lie Presentation and lie Breech twin 1Breech twin 1
Fetal/maternal complicationsFetal/maternal complications Preterm labourPreterm labour Growth restrictionGrowth restriction Previous caesarean sectionPrevious caesarean section Elective deliveryElective delivery
ConsiderConsider

Delivery monochorionic diamniotic?Delivery monochorionic diamniotic?
No evidenceNo evidenceElective LSCSElective LSCS Allows early delivery (36-37 weeks)Allows early delivery (36-37 weeks) Avoids late onset TTTSAvoids late onset TTTS Avoids “circulatory charge” T2 after T1 Avoids “circulatory charge” T2 after T1
delivereddelivered Small number of absolute total of twinsSmall number of absolute total of twins
Vaginal deliveryVaginal delivery No antenatal evidence TTTSNo antenatal evidence TTTS Favorable cervix (multips)Favorable cervix (multips) Limit delivery interval Limit delivery interval Monitor T2 carefullyMonitor T2 carefully

Presentations of twinsPresentations of twins
CephalicCephalic BreechBreech OtherOther
CephalicCephalic 38.638.6 13.113.1 0.60.6
BreechBreech 25.525.5 9.29.2 0.60.6
Other Other 8.08.0 3.93.9 0.5 0.5
FIRST TWIN
SECOND TWIN
Percentage of presentation combinations in labour

Breech twin 1Breech twin 1 Prevalent practice =LSCSPrevalent practice =LSCSACOG recommends LSCSACOG recommends LSCSReasons sitedReasons sited
Interlocking twins (1 in 90)Interlocking twins (1 in 90) Interference with decent of Interference with decent of
breechbreech Term breech study (irrelevant)Term breech study (irrelevant) Lack of experience Lack of experience
Vaginal delivery maybe safe Vaginal delivery maybe safe in selected casesin selected cases
EFW1500-3500EFW1500-3500 US no interlocked headsUS no interlocked heads No IUGRNo IUGR Non-footling breechNon-footling breech

0
500
1000
1500
2000
2500
3000
3500
We
igh
t (g
)
Twin 1Twin 2
Weight difference in twins
Audit data SHH 1998
N=45
Twin 1 is not usually bigger than twin 2

Evidence based medicine & twins?Evidence based medicine & twins?
Observational and non-randomised comparative Observational and non-randomised comparative studiesstudies
Address controversyAddress controversy:: mode of delivery of twin 2mode of delivery of twin 2 time interval between delivery of T1 andT2time interval between delivery of T1 andT2 ECV vs breech extractionECV vs breech extraction Trial of scar in twin pregnancyTrial of scar in twin pregnancy
Problem:Problem: retrospective studiesretrospective studies inappropriate measures of outcomeinappropriate measures of outcome recommendations are often empiricalrecommendations are often empirical

Delivery of growth restricted twinsDelivery of growth restricted twins
30-50% IUGR30-50% IUGR ProgressiveProgressive Beginning 32-34wksBeginning 32-34wks Worse after 36wksWorse after 36wks
Offer IOL at 38wksOffer IOL at 38wks Earlier if severe IUGR Earlier if severe IUGR
Doppler assessmentDoppler assessment
Delivery modeDelivery mode EFWEFW Severe discordance (>20%)Severe discordance (>20%)

Vertex/vertexVertex/vertex
Literature supports Literature supports vaginal deliveryvaginal delivery
5% cases T2 will 5% cases T2 will become non-vertex become non-vertex after delivery T1after delivery T1
Report 81% success Report 81% success
Differences of opinionDifferences of opinion ??Perinatal morbidityPerinatal morbidity
Concerns Concerns Head entrapmentHead entrapment
Overall evidence Overall evidence suggests vaginal suggests vaginal delivery is as safe as delivery is as safe as LSCSLSCS
Vertex/breechVertex/breech

VTX/Non-VTX
>2000g<24 weeks
ECV T2
Successful
>24wks & <2000g
Vaginal T1
*Vaginal breech T2
Vaginal T1&T2
*Vaginal breechT2
Probable vaginal T2
Vaginal T1
ECV T2
Unsuccessful UnsuccessfulSuccessful
LSCSLSCS
Probable vaginal T2
*Suitable for vaginal breech

Recent evidence?Recent evidence?
Retrospective 92-97ScotlandAll twin births >24 weeksExcluding
pre-labour IUD Congenital abnormality
PRETERM (vaginal)1438 twin pairs <36/40
23 deaths T1 23 deaths T2
Pulmonary & anoxia
TERM (vaginal) 2436 twin pairs >36/40
No deaths T1 9 deaths T2
7 deaths due to anoxia5 “mechanical” problems
TERM (elective LSCS)454 twin pairs
No deaths T1 or T2
Conclusion
Planned caesarean birth may prevent perinatal deaths
BUT
Chorionicity unknown
(7 of 9 T2 deaths were concordant for sex ie. may be monochorionic)
Smith et al 2002, BMJ

Twin vaginal birth after LSCSTwin vaginal birth after LSCS
Controversial limited data about safetyControversial limited data about safety
Concern ?Concern ?risk of uterine rupturerisk of uterine rupture Over-distentionOver-distention Intrauterine manipulationsIntrauterine manipulations
No evidence of risk No evidence of risk 3 studies no increased risk3 studies no increased risk Other caused of over-distention noOther caused of over-distention noriskrisk
Trial of labour at maternal requestTrial of labour at maternal request

AnalgesiaAnalgesia
Appropriate analgesia essentialAppropriate analgesia essential
Operative delivery may be Operative delivery may be requiredrequired
Increased risk of GAIncreased risk of GA Prophylactic antacidsProphylactic antacids
Anaesthetist available on LWAnaesthetist available on LW
Epidural optimizes vaginal Epidural optimizes vaginal delivery (recommended)delivery (recommended)
Epidural not mandatoryEpidural not mandatory Nitrous oxideNitrous oxide OpiatesOpiates

Issues in monitoring twinsIssues in monitoring twins
““High risk”High risk” EFM EFM
Continuous & simultaneousContinuous & simultaneous
External transducer External transducer T2T2
FSE FSE T1 T1 after ROMafter ROM
Ensure 2 heartbeats seenEnsure 2 heartbeats seen
Careful monitoring after Careful monitoring after delivery of T1 delivery of T1 (ultrasound aids (ultrasound aids transducer positioning)transducer positioning)

‘‘The Delivery’ - Twin 1The Delivery’ - Twin 1
Encourage active pushing Encourage active pushing
Semi-recumbent position Semi-recumbent position once T1 crowningonce T1 crowning
Episiotomy as necessaryEpisiotomy as necessary
Clamp & mark cord T1Clamp & mark cord T1
Ventouse or forcepsVentouse or forceps

‘‘The Delivery’ - Twin 2The Delivery’ - Twin 2
ECV
versus
Breech delivery
versus
Internal podalic version
Palpate lie immediately after delivery T1

‘ ‘ The Delivery’ - Twin 2The Delivery’ - Twin 2
Start syntocinon infusion Start syntocinon infusion once T2 cephaliconce T2 cephalicEscalate dose at 5 minute Escalate dose at 5 minute intervalsintervalsAwait contractions & PP to Await contractions & PP to stabilized above pelvisstabilized above pelvisARMARMFSE if poor external CTGFSE if poor external CTGVentouseVentouseBreech extractionBreech extraction?Delivery interval?Delivery interval

Combined vaginal-abdominal deliveryCombined vaginal-abdominal deliveryMisfortune or mismanagement?Misfortune or mismanagement?
Increasing incidence Increasing incidence 1-15% LSCS T21-15% LSCS T2
Higher rate elLSCS in Higher rate elLSCS in twinstwins LSCS for T2LSCS for T2 Operator experienceOperator experience Some management Some management
issuesissues
JustifiedJustified Failed version in Failed version in
transverse lietransverse lie SROM-shoulder SROM-shoulder
presentationpresentation Cord prolapse Cord prolapse
(especially prems)(especially prems) Large T2Large T2 ?Fetal distress with ?Fetal distress with
high presenting parthigh presenting part

Delayed delivery intervalDelayed delivery interval
Caution:Caution:isolated case reportsisolated case reports
publication biaspublication bias
Consideration:Consideration:gestation gestation
chorionicitychorionicity
maternal informed maternal informed consentconsent

Delayed delivery intervalDelayed delivery interval
48 twin pregnancies48 twin pregnancies
40/96 surviving 40/96 surviving infants infants (39=T2)(39=T2)
Interval 3 - 143 daysInterval 3 - 143 days
mean 44.8 daysmean 44.8 days
No consensus on No consensus on treatment strategytreatment strategy
Obs & Gyn Survey 1999: 54,343-8

‘‘The delivery’ - third stageThe delivery’ - third stage
Active managementActive management
Syntocinon 5 units Syntocinon 5 units (IV or IM)(IV or IM) after delivery after delivery of second twinof second twin
Syntocinon infusion after delivery of Syntocinon infusion after delivery of placentaplacenta

UK birth rate of TripletsUK birth rate of Triplets
0
50
100
150
200
250
300
1982 1984 1986 1988 1990 1992 1994

Higher multiples-?chorionicityHigher multiples-?chorionicity
Can be:Can be: TrichorionicTrichorionic DichorionicDichorionic
TriamnioticTriamniotic
Diamniotic Diamniotic MonochorionicMonochorionic
Tri-amnioticTri-amniotic
Monoamniotic (rare)Monoamniotic (rare)
Scan earlyScan early
Scan oftenScan often