Embed Size (px)
DESCRIPTION
Definition of MI Dual antiplatelet therapy in secondary prevention
Citation preview

Myocardial Infarction FAQ: Based on Current Guidelines and Evidence
Joonseok (“Joon”) Kim, M.D.MSU Internal Medicine PGY3
February 13, 2014

Contents
• Definition of MI• Interpretation of Troponin Elevations• MI in Critically Ill Patients• Antiplatelet Therapy in Post MI

CASE
• A 56-year-old man is admitted to the hospital with new-onset substernal chest pressure. Medical history is remarkable for hyperlipidemia. He is a cigarette smoker. His medications are aspirin and atorvastatin.
• On physical examination, the patient is afebrile, blood pressure is 132/78 mm Hg, pulse rate is 82/min and regular, and respiration rate is 14/min. No jugular venous distention is noted, the lungs are clear to auscultation, no murmur or gallop is heard, and no peripheral edema is noted.

CASE
• On admission, cardiac troponin I level was 1.2 ng/mL (1.2 µg/L); on hospital day 2 it peaks at 8.4 ng/mL (8.4 µg/L). An electrocardiogram on arrival to the emergency department demonstrated a nonspecific ST-T wave abnormality, but no ST-segment elevation or depression. He began receiving metoprolol, clopidogrel, and intravenous heparin.
• Cardiac catheterization demonstrates overall preserved left ventricular systolic function with diffuse severe disease of the distal portion of all three major epicardial vessels. No catheter-based intervention is performed.

CASE
• What do you want to do upon discharge?
A. Continue aspirin only and stop clopidogrelB. Continue aspirin + clopidogrel therapy for 2 weeksC. Continue aspirin + clopidogrel therapy for 1 yearD. Continue aspirin + clopidogrel therapy lifelong

In Reality…

Since 2011…
• AHA/ACCF Secondary Prevention and Risk Reduction Therapy for Patients With Coronary and Other Atherosclerotic Vascular Disease: 2011 Update
• ACCF 2012 Expert Consensus Document on Practical Clinical Considerations in the Interpretation of Troponin Elevations
• 2012 ACCF/AHA Focused Update of the Guideline for the Management of Patients With Unstable Angina/Non–ST-Elevation Myocardial Infarction
• 2012 Third Universal Definition of Myocardial Infarction
• 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction


Let’s Go Back to Basics
What is MI?

NSTEMI
Presentation
Working Dx
ECG
CardiacBiomarker
Final DxNQMI Qw MI
UA
UnstableAngina
Ischemic Discomfort
Acute Coronary Syndrome
Myocardial Infarction
ST Elevation
No ST Elevation
Non-ST ACS
Libby P. Circulation 2001;104:365, Hamm CW, Bertrand M, Braunwald E, Lancet 2001; 358:1533-1538; Davies MJ. Heart 2000; 83:361-366. Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1-e157, Figure 1. Reprinted with permission.
10

Causes of UA/NSTEMI• Thrombus or thromboembolism, usually arising on
disrupted, or eroded plaque• Occlusive thrombus, usually with collateral vessels• Subtotal occlusive thrombus on pre-existing plaque• Distal microvascular thromboembolism from plaque-associated
thrombus • Thromboembolism from plaque erosion
• Non–plaque-associated coronary thromboembolism• Dynamic obstruction (coronary spasm or
vasoconstriction) of epicardial and/or microvascular vessels
• Progressive mechanical obstruction to coronary flow• Coronary arterial inflammation• Secondary UA• Coronary artery dissection
DeWood MA, et al. N Engl J Med 1986;315:417–23; Braunwald E. et al. Circulation 1998;98:2219–22; Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1-e157

ACC/AHA

















• 1. Even though elevated troponin is a sensitive and specific indication of cardiac myonecrosis, by itself, it does not indicate a myocardial infarction (MI) (myonecrosis due to ischemia) or any specific etiology.
ACCF 2012 Expert Consensus Document on Practical Clinical Considerations in the Interpretation of Troponin Elevations. JACC 2012
10 Points to Remember from an Expert Consensus Document on Interpretation of Troponin Elevations

• 2. The ‘Third Universal Definition of Myocardial Infarction’ (2012) classifies 5 types of MI: Type 1 is termed spontaneous, related to ischemia due to a primary coronary event (e.g., plaque rupture); Type 2 is secondary to increased oxygen demand or decreased supply; Type 3 is associated with sudden unexpected cardiac death; Type 4a is associated with percutaneous coronary intervention (PCI); Type 4b is associated with stent thrombosis; and Type 5 is associated with coronary artery bypass grafting (CABG) surgery.
ACCF 2012 Expert Consensus Document on Practical Clinical Considerations in the Interpretation of Troponin Elevations. JACC 2012
10 Points to Remember from an Expert Consensus Document on Interpretation of Troponin Elevations

• 3. An elevated troponin level that is ‘smoldering’ and relatively constant over an appropriate sampling interval is more likely to be caused by chronic diseases (e.g., heart failure) versus ischemia.
ACCF 2012 Expert Consensus Document on Practical Clinical Considerations in the Interpretation of Troponin Elevations. JACC 2012
10 Points to Remember from an Expert Consensus Document on Interpretation of Troponin Elevations

• 4. A 20% change at 3-6 hours from the baseline value may be suggestive of MI. That said, there is insufficient evidence to provide concrete guidelines on how to differentiate between acute coronary syndrome (ACS) and non-ACS ischemia-induced troponin elevations without accounting for the clinical circumstances.
ACCF 2012 Expert Consensus Document on Practical Clinical Considerations in the Interpretation of Troponin Elevations. JACC 2012
10 Points to Remember from an Expert Consensus Document on Interpretation of Troponin Elevations

• 5. It is imperative to incorporate troponin testing into global risk assessment. Those patients with an elevated troponin and a high pretest probability of ACS are most likely to derive benefit from a treatment strategy that targets coronary thrombosis.
ACCF 2012 Expert Consensus Document on Practical Clinical Considerations in the Interpretation of Troponin Elevations. JACC 2012
10 Points to Remember from an Expert Consensus Document on Interpretation of Troponin Elevations

• 9. Regardless of the etiology of troponin elevation (or associated disease state), troponin elevation offers incremental prognostic value.
ACCF 2012 Expert Consensus Document on Practical Clinical Considerations in the Interpretation of Troponin Elevations. JACC 2012
10 Points to Remember from an Expert Consensus Document on Interpretation of Troponin Elevations

Troponin I Levels to Predict the Riskof Mortality in Acute Coronary Syndromes
35Antman EM, et al. N Engl J Med 1996;335:1342.
Crude mortality rates at 42 days in patients with ACS

• 10. Troponin may be a useful tool to detect chemotherapy-associated cardiac toxicity, and may have a role in informing the use of treatment in those patients who develop cardiac myonecrosis following high-dose chemotherapy.
10 Points to Remember from an Expert Consensus Document on Interpretation of Troponin Elevations
ACCF 2012 Expert Consensus Document on Practical Clinical Considerations in the Interpretation of Troponin Elevations. JACC 2012

Myocardial Infarction in the ICU
• Elevations of troponin values are common in patients in the intensive care unit and are associated with adverse prognosis, regardless of the underlying disease state.
Third Universal Definition of Myocardial Infarction, JACC 2012

Myocardial Infarction in the ICU
• Some elevations may reflect MI type 2 due to underlying CAD and increased myocardial oxygen demand
• Other patients may have elevated values of cardiac biomarkers, due to myocardial injury with necrosis induced by catecholamines or direct toxic effect from circulating toxins
• Moreover, in some patients, MI type 1 may occur
Third Universal Definition of Myocardial Infarction, JACC 2012

Myocardial Infarction in the ICU
• It is often a challenge for the clinician, caring for a critically ill patient with severe single organ or multi-organ pathology, to decide on a plan of action when the patient has elevated cTn values.
• If and when the patient recovers from the critical illness, clinical judgment should be employed to decide whether—and to what extent—further evaluation for CAD or structural heart disease is indicated.
Third Universal Definition of Myocardial Infarction, JACC 2012

Antiplatelet Therapy

Class I Benefit >>> Risk
Procedure/ Treatment SHOULD be performed/ administered
Class IIa Benefit >> RiskAdditional studies with focused objectives needed
IT IS REASONABLE to perform procedure/administer treatment
Class IIb Benefit ≥ RiskAdditional studies with broad objectives needed; Additional registry data would be helpful
Procedure/Treatment MAY BE CONSIDERED
Class III Risk ≥ BenefitNo additional studies needed
Procedure/Treatment should NOT be performed/administered SINCE IT IS NOT HELPFUL AND MAY BE HARMFUL
shouldis recommendedis indicatedis useful/effective/
beneficial
is reasonable
can be useful/effective/ beneficial
is probably recommended or indicated
may/might be consideredmay/might be reasonableusefulness/effectiveness
is unknown /unclear/uncertain or not well established
is not recommendedis not indicatedshould notis not
useful/effective/beneficial
may be harmful
Applying Classification of Recommendations and Level of Evidence
ACC/AHA Recommendations

Class I Benefit >>> Risk
Procedure/ Treatment SHOULD be performed/ administered
Class IIa Benefit >> RiskAdditional studies with focused objectives needed
IT IS REASONABLE to perform procedure/administer treatment
Class IIb Benefit ≥ RiskAdditional studies with broad objectives needed; Additional registry data would be helpful
Procedure/Treatment MAY BE CONSIDERED
Class III Risk ≥ BenefitNo additional studies needed
Procedure/Treatment should NOT be performed/administered SINCE IT IS NOT HELPFUL AND MAY BE HARMFUL
Level A: Recommendation based on evidence from multiple randomized trials or meta-analyses Multiple (3-5) population risk strata evaluated; General consistency of direction and magnitude of effect
Level B: Recommendation based on evidence from a single randomized trial or non-randomized studies Limited (2-3) population risk strata evaluated
Level C: Recommendation based on expert opinion, case studies, or standard-of-care Very limited (1-2) population risk strata evaluated
Applying Classification of Recommendations and Level of Evidence
ACC/AHA Recommendations

Antithrombotic Trialists’ Collaboration. BMJ 2002;324:71–86
Category % Odds ReductionAcute MIAcute CVA Prior MIPrior CVA/TIAOther high risk CVD
(e.g. unstable angina, heart failure) PAD
(e.g. intermittent claudication) High risk of embolism (e.g. Afib) Other (e.g. DM)All trials
1.00.50.0 1.5 2.0 Control better Antiplatelet better
*Aspirin was the predominant antiplatelet agent studied**Include MI, stroke, or death
Aspirin reduces the risk of adverse cardiovascular events
Aspirin Evidence: Secondary Prevention

Aspirin (75-162 mg daily) if known CAD† or NSTE-ACS‡
Aspirin (81-325 mg daily) following PCI or fibrinolytic therapy for a STEMI*
Aspirin (preferentially at 81 mg daily) following PCI for a NSTE-ACS# or a STEMI* or fibrinolytic therapy for a STEMI*
Smith SC Jr. et al. JACC 2011;58:2432-2446Wright RS et al. JACC 2011;57:e215-367
O’Gara PT et al. JACC 2013;61:e78-e140Jneid H et al. JACC 2012;60:645-681
I IIaIIbIII
I IIaIIbIII
I IIaIIbIII
Aspirin Recommendation: Secondary Prevention

Aspirin (162-325 mg daily) for at least 1 month after bare metal stent implantation (Class I, Level B), at least 3 months after sirolimus-eluting stent implantation (Class I, Level B), and at least 6 months after paclitaxel-eluting stent implantation (Class I, Level B) after which aspirin (75-162 mg daily) should be continued indefinitely (Class I, Level A for a bare metal stent and Class I, Level B for a drug eluting stent)
Aspirin (75-162 mg daily) as the initial dose after stent implantation in those at higher bleeding risk
King SB 3rd et al. JACC 2008;51:172-209
I IIaIIbIII
I IIaIIbIII
I IIaIIbIII
Aspirin Recommendation: Secondary Prevention

Aspirin (100-325 mg daily) following CABG surgery
Hillis LD et al. JACC 2011;58:e123-210
I IIaIIbIII
Aspirin Recommendation: Secondary Prevention

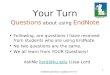
12,562 patients with NSTE-ACS randomized to daily aspirin (75-325 mg) or clopidogrel (300 mg load, 75 mg thereafter) plus aspirin (75-325 mg) for 9 months
Dual antiplatelet therapy is more efficacious in NSTE-ACS
3 6 90 12
Rat
e of
CV
dea
th,
myo
card
ial i
nfar
ctio
n,
or s
trok
e
P<0.001
Months of Follow Up
CURE Trial Investigators. NEJM 2001;345:494-502
Aspirin + Placebo
Aspirin + Clopidogrel
Clopidogrel in Unstable Angina to Prevent Recurrent Events (CURE) Trial
DAPT Recommendation: Secondary Prevention

2,116 patients undergoing PCI randomized to 4 weeks of DAP* followed by aspirin (75-325 mg) monotherapy vs. persistent DAP* for 1 year
DAP therapy produces greater benefit when used for 1 year
Steinhubl S et al. JAMA 2002;288:2411-2420
0 123 6 90
Ris
k of
MI,
stro
ke,
or d
eath
(%
)
27% RRR, P=0.02
10
5
15 4 weeks of DAP*
Months from Randomization
1 year of DAP*
Clopidogrel for the Reduction of Events during Observation (CREDO) Trial
DAPT Recommendation: Secondary Prevention

COMMIT Collaborative Group. Lancet 2005;366:1607-1621
9% relative risk reduction (P=.002)
(10.1%)(9.2%)
Days Since Randomization (up to 28 days)
Dea
th,
MI,
or
Str
oke,
%
10
9
8
7
6
5
4
3
0
0
In-H
ospi
tal M
orta
lity,
%
Days Since Randomization (up to 28 days)
(8.1%)(7.5%)
7% relative risk reduction (P=.03)
7 14 21 28 7 14 21 280
8
7
6
5
4
3
2
1
0
Clopidogrel and Metoprolol in Myocardial Infarction (COMMIT) Trial
45,852 patients presenting within 24 hours of STEMI treated medically and randomized to aspirin and clopidogrel (75 mg daily) vs. aspirin only
DAPT produces greater benefit in medically managed STEMI patients
DAPT Recommendation: Secondary Prevention

Clopidogrel (75 mg daily; Class I, Level B), prasugrel* (10 mg daily; Class I, Level C), or ticagrelor (90 mg twice daily; Class I, Level C) if aspirin intolerance or a true aspirin allergy following a NSTE-ACS
Clopidogrel (75 mg daily) or ticagrelor (90 mg twice daily) in addition to aspirin for up to 1 year following a NSTE-ACS managed conservatively
Jneid H et al. JACC 2012;60:645-681
I IIaIIbIII
I IIaIIbIII
I IIaIIbIII
*In PCI treated patients
DAPT Recommendation: Secondary Prevention

Clopidogrel (75 mg daily), prasugrel (10 mg daily), or ticagrelor (90 mg twice daily) in addition to aspirin for 1 year following PCI for a NSTE-ACS or a STEMI
Clopidogrel (75 mg daily) in addition to aspirin for a minimum of 14 days (Class I, Level A) and up to 1 year (Class I, Level C) following fibrinolytic therapy for a STEMI
Jneid H et al. JACC 2012;60:645-681O’Gara PT et al. JACC 2013;61:e78-e140
I IIaIIbIII
I IIaIIbIII
I IIaIIbIII
DAPT Recommendation: Secondary Prevention

If the risk of morbidity because of bleeding outweighs the anticipated benefit afforded by a P2Y12 receptor antagonist, earlier discontinuation should be considered
Continuation of a P2Y12 receptor antagonist beyond 1 year may be considered in patients undergoing drug eluting stent placement
I IIaIIbIII
I IIaIIbIII
Kushner F et al. JACC 2009;54:2205-2241Jneid H et al. JACC 2012;60:645-681
O’Gara PT et al. JACC 2013;61:e78-e140
DAPT Recommendation: Secondary Prevention

CASE
• A 56-year-old man is admitted to the hospital with new-onset substernal chest pressure. Medical history is remarkable for hyperlipidemia. He is a cigarette smoker. His medications are aspirin and atorvastatin.
• On physical examination, the patient is afebrile, blood pressure is 132/78 mm Hg, pulse rate is 82/min and regular, and respiration rate is 14/min. No jugular venous distention is noted, the lungs are clear to auscultation, no murmur or gallop is heard, and no peripheral edema is noted.

CASE
• On admission, cardiac troponin I level was 1.2 ng/mL (1.2 µg/L); on hospital day 2 it peaks at 8.4 ng/mL (8.4 µg/L). An electrocardiogram on arrival to the emergency department demonstrated a nonspecific ST-T wave abnormality, but no ST-segment elevation or depression. He began receiving metoprolol, clopidogrel, and intravenous heparin.
• Cardiac catheterization demonstrates overall preserved left ventricular systolic function with diffuse severe disease of the distal portion of all three major epicardial vessels. No catheter-based intervention is performed.

• What do you want to do upon discharge?
A. Continue aspirin only and stop clopidogrelB. Continue aspirin + clopidogrel therapy for 2 weeksC. Continue aspirin + clopidogrel therapy for 1
yearD. Continue aspirin + clopidogrel therapy lifelong
Back to Initial Case…

Q & A
• Thank you for your attention