Embed Size (px)
Citation preview

Magnets in Orthodontics
Dr.Umar Mohamed

Contents• Introduction• History• Classification of Magnets• Properties of Magnets• Types of Magnets• Application of Magnets• Application in Orthodontics Intrusion Distalization • Appliances and class IIcorrection• Appliances and class III correction
• Biological Safety of Magnets• Conclusion• References

Introduction• A magnet (from Greek μαγνήτης λίθος,
"Magnesian stone") is a material or object that produces a magnetic field .This magnetic field is invisible and causes the most notable property of a magnet a force that pulls on nearby magnetic materials, or attracts or repels other magnets.
• Magnets attract specific metals, and they have north and south poles. Opposite poles attract each other while like poles repel.

History• Ancient people learned about magnetism from
lodestones, naturally magnetized pieces of iron ore. They are naturally created magnets, which attract pieces of iron. The word magnet in Greek meant "stone from Magnesia, a part of ancient Greece where lodestones were found.

• According to Matasa, the first person to write a book on magnets was William Gilbert in 1600.
• It was William Gilbert who first realized that the Earth was a giant magnet.
• Serious use of magnets in medicine was reported in early 19th century.

• Widely recognized use of magnetic force is by orthopedic surgeons to overcome non-union of fractures in long bones.
Behrman wrote about the retention of dentures by the use of magnets as early as 1953.

• The pioneer work of clinical use of magnets in orthodontics was by Kawata, Blechman and Smiley in 1978.

Properties of magnets

Magnetic Field
• It’s the space in which magnetic pole experiences a force.

Coulomb’s Inverse Square Law
• The force between two isolated magnetic poles is directly proportional to product of their pole strengths and inversely proportional to the square of the distance between them.
• F α m1 X m2
• Curie point:-Pierre Curie(1859-1906)
d2

Coercivity• It is the strength of the external field needed to
demagnetize the material. It is also a measure of the resistance of the material to demagnetization.
• A high coercivity is needed to prevent the magnets from demagnetization when they encounter fields produced by other sources.

Types of magnetic materials in
dentistry• Platinum-cobalt(Pt-co)• Aluminium-Nickel-Cobalt(Al-Ni-Co)• Ferrite• Chromium-cobalt-Iron• Samarium Cobalt(SmCo)• Neodymium-Iron-Boron(Nd2Fe14B)

• One reason for increased use of magnets is the recent development of small magnets made of powerful permanent magnet alloy called rare earth magnets.
• Breakthrough in use of magnets.

Advantages of Rare Earth Magnets over Conventional
Magnets
• High energy product value (smaller magnets can be used)
• Permanent magnet (ie, high coercivity)
• Predictability of amount and direction of force
• Force is directly proportional to size and shape of the magnet

The advantages of magnetic force systems are
• Predictable force levels• Better directional force• No force decay over time• Can exert their force through mucosa and bone• Frictionless mechanism• Less patient discomfort and more patient
cooperation

Application in Orthodontics

Tooth movement• Simple tooth movement without archwires:
Muller (1984)
• Small magnets (approximately 5 x 3 x 1 mm) deliver light continuous forces to close diastemas.

Intrusion• Dellinger (Am J Orthod. 1986) Active Vertical
Corrector• samarium-cobalt magnets, • Replusive intrusive force-600-700 g per magnetic
unit• Headcap and chinstrap.

• Kiliardis et al. (1990), and Woods and Nanda
(1988); (1989), however, have not found magnets incorporated within bite blocks any more efficient at intruding posterior teeth than bite blocks alone.
• Kiliardis et al. (1990) also concluded that the repulsive element of the magnets produced
lateral mandibular movements and thus increased the risk of developing crossbites.

Advantages• Magnets produce a light
continuous force that increases as the teeth get nearer and therefore move quickly,
• Chairside time is low
• No need to reactivate the appliance as long as the magnets have been correctly placed
• Maintaining good oral hygiene is easy.
• Position of the teeth can be controlled by the position of the magnets on the teeth.
• Difficulty in correctly positioning the magnets
Disadvantages

• Canine retraction
Complex intra and inter arch mechanics (Blechman, 1985)
3 magnet configuration to enhance Canine retraction

3 magnet configuration used to simultaneously move all 4 canines distally

• Class II mechanics using magnetic force system in Class II nonextraction case

Impacted tooth• Surgical exposure of the impacted tooth and
applying an attachment of small high energy magnets to provide the traction force so as to aid the eruption of an impacted maxillary canine has been described by Sandler (1991) and Darendeliler and Freidle (1994)
• Small neodymium-iron-boron magnets (3 x 3 x 1 mm) –impacted canine
• Larger magnet(5x5x2 mm )-removable appliance.

Advantages• Rapid, safe, and sure eruption of teeth in much less
time than conventional methods
• No chains, lassos, or ligatures penetrat ing the palatal tissue reduces chances of inflammation, infection, potential ankylosis,
• The attachment is less likely to be knocked and dislodged from the tooth.
• Magnets produce constant physiological forces (40 to 60Gms) over long periods of time and the direction of the force can be chosen by the clinician
• .•

Disadvantages • Disadvantages• Greater the distance of the impacted tooth from
the oral cavity smaller the forces between the
magnets. • The magnets may corrode if their coating is
damaged,




• Mancini (1996) has shown that the attractive
force levels generated between neodymium-iron-
boron magnets set in attraction are sufficient to
induce the cellular and biochemical changes that
are required to produce orthodontic tooth
movement over a reasonable clinical range.

Molar Distalization• Gianelly et al., (1988, 1989) moved maxillary first
molars distally with an intra-oral device using repelling magnets in conjunction with a modified Nance appliance.
• 3 mm in 7 weeks

• Bondemark and Kurol (1992) discussed the simultaneous movement of first and second molars using repelling samarium-cobalt magnets.
• Repelling force -58 to 215 g.
• Maxillary molars were moved to a Class I relationship within an average time span of 16.6 weeks.

• Bondemark et al. (1994) examined repelling magnets versus superelastic nickel titanium coils
used for simultaneous distal movement of maxillary first and second molars.
• Distal molar movement was 3.2 mm for the supercoils and 2.2 mm.
• The results indicated that superelastic coils are more effective than repelling rare earth magnets in molar distalisation

EXPANSION • Intra-maxillary expansion and orthopaedic
movement of the palatal shelves using samarium-cobalt magnets to provide the expansion force
was studied by Vardimon et al. on monkeys in (1987)

Tooth borne appliance
Tissue borne appliance

Funtional appliances
• Vardimon et al., (1989,1990) developed the functional orthopaedic magnetic appliance (FOMA II and III), with positive treatment effects in monkeys.
• In FOMA II, upper and lower attracting neodymium- iron-boron magnets maintain the mandible in an advanced sagittal position to establish a skeletal response.
FOMA II & III

• The results showed that 570 g of magnetic force were produced when the magnets were in apposition and 219 g of force if the jaws were in the rest position. Favourable changes were noted in all active cases.

Magnetic Activator Device(MAD)
Darendeliler and Joho, (1993) developed this magnetically active functional appliance.
Anterior attracting neodymium-iron-boron magnets and posterior repelling magnets.
The repelling magnets generate a force of 300 g each with bite opening 5.5-6.0 mm at the first molars. The two midline-attracting magnets produce a force of
300 g.

• Several types have been designed to deal with differing clinical problems,
• (MAD I) - lateral displacement • (MAD II) - Class II malocclusions • (MAD III) - Class III malocclusions and • (MAD IV) - open bite cases

• Each appliance has a lingual acrylic portion with two "C" type retention clasps on the first molars, a labial bow, two samarium cobalt magnets (Sm2Co17) and an occlusal bite plane to avoid cusp interferences
• A 30° inclination of the occlusal surface (4 ´ 6 mm) of the magnet to the basal surface (5.2 ´ 4 mm) produces an oblique force vector to correct a Class II malocclusion.
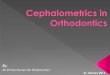
MAD II

MAD III• A MAD III appliance was constructed
from a bonded upper plate and a removable lower plate, each carrying two buccal magnets .
• The lower buccal magnets were placed more anteriorly and buccally than the upper buccal magnets so their attractive force would not interfere with the repulsive force of the midpalatal magnets.

• The upper and lower magnets had a tendency to move toward a fully centered contact, thus creating a forward force against the maxilla and a backward force against the mandible.
• The total sagittal force between the upper and lower plates was about 300g initially, increasing to 600g as the crossbite and Class III condition were corrected.

Magnetic Twin block
• Clark used SmCo & NdFeB in his Twin block. The magnets were embedded in the inclined surface of the Twin blocks. In attractive mode they ensured the Twin blocks are always in contact even at night. When used in repelling mode it reduces the need for reactivation by inducing additional forward posture of mandible.


The Propellant Unilateral Magnetic Appliance (PUMA):
• Chate, 1995 - Introduced a new technique for hemifacial microsomia; used for stimulating the autogenous costochondral graft.
• Consists of SmCo magnets embedded in upper & lower acrylic bite blocks in repelling mode. The long axis of the magnets are perpendicular to blocks interface. Encouraging results were reported.


Retainers • Springat & Sandler (1991) suggested the
use of micro magnets to retain central incisors that have been brought together
to close a midline diastema.

Magnetic sensor• A system was developed for measuring tooth
displacement by orthodontic force. Eight small magnetic sensors and a magnet are combined to measure threedimensional displacement.
• Sensors, arranged cubically in the three planes of space, are placed in the mouth and fixed to the posterior teeth by a splint. A
• magnet is placed in the center of the 8 sensors and attached to a front tooth that is subjected to orthodontic force.
• Sensors detect the magnet's movement as target tooth displacement

Biological safety of magnets
• To evaluate biological safety 3 levels of testing are conducted
Level 1: In vitro Testing to evaluate toxic and carcinogenic effect
Level 2: Testing on animals
Level 3: Clinical trials

• Kawata (1987) : No significant changes in Ascorbic acid, Ca2+ and Citric acid concentrations in blood, but after application of force by conventional orthodontic treatment there is decrease in blood and adrenal gland concentration of Ascorbic acid and it is related to stress.
• WHO reports (1993) suggests that static magnetic fields up to 2T shows no significant health effects. However short term exposure to static fields greater than 5T may produce detrimental health effects

Conclusion
• Magnets can be used to give predictable forces in either attraction or repulsion; they can be made small enough to suit most dental and orthodontic applications and can produce high forces.Their use in orthodontics, however, is limited due to a number of factors.
.

• The force between two magnets drops dramatically with distance and even at small distances apart the forces can be very low.
• When heated they can suffer considerable loss of flux and, therefore, force.
• The orientation of one magnet to another is of the utmost importance and when not in perfect alignment the force between them drops significantly
Revista Latinoamericana de Ortodoncia y Odontopediatría Ortodoncia.ws edición electrónica Octubre 2011 Kumar A, Mascarenhas R,Husain, A.

Thank you

Reference• Rare earth magnets in Orthodontics – Joseph H. Noar
BJO1999.• Magnetic force systems in orthodontics – Blechman
AJO1985• The use of magnets to move the molars distally –
Gianelly AJO1989• Magnetic versus mechanical expansion with different
force thresholds & points of force application – Vardimon AJO1987.
• Cl-II bimaxillary protrusion treated with Magnetic Forces - Darendeliler JCO1992.
• Open bite correction with the Magnetic activator device IV-Darendeliler JCO1995.