Embed Size (px)
DESCRIPTION
My successful LRP application 2011
Citation preview

Research Plan:
I am currently finishing my PGY-3 year of clinical training in Radiation Oncology. During the past 8 months I have spent my research time involved with two groups at Moffitt Cancer Center: one is the NCI’s newly created Physical Sciences in Oncology Center (PS-OC) and the other is Moffitt’s Integrative Mathematical Oncology (IMO) group. With these two groups I have found an intellectual home and a place where my unique skill set and manner of thinking are of real value. I have had enormous success in the short time I have been involved with these groups: I have won a poster award, an ASCO merit award and a 1 year, $200,000 grant from the NCI. Further, I have submitted an original manuscript, have two more in preparation, and have an R21 pending. This work has all been outside of my clinical training, which has continued unabated to this point. I have maintained an excellent standing in my clinical residency program while doing this extra work, and have continued to be involved in the expected load of clinical research as well - publishing two clinical manuscripts1,2 last year and leading a multi-institutional, international collaboration studying glioblastoma in the elderly. Burning the candle at both ends, as it were, has allowed me to accomplish quite a bit, but what I have not been able to do is fully devote myself to my research training.
My role in the lab to date has been innovator, connector, facilitator and translator. To become the independent physician-scientist that I envision, I must take dedicated time to further hone my thinking and research skills. To do this, I need dedicated time for research. I propose to take a three year hiatus from my clinical residency training to do just this. During the three years I will continue my employment at Moffitt Cancer Center, but will be a Research Associate instead of a clinical resident. I will also be enrolled in Oxford University during this time and officially be reading for a doctorate in mathematics. While I will physically be in the United States during the majority of this time, I will be co-supervised by faculty at Moffitt and Oxford. My research during this time, and therefore my doctoral thesis, will be focused on building and validating mathematical models of the metastatic process from primary tumor intravasation to the circulatory phase of metastasis to extravasation and colony formation.
I have chosen to study metastasis because it is currently one of the biggest outstanding questions in cancer. While metastatic disease accounts for the lion’s share of cancer death, it is by far the least understood and most poorly characterized phase of cancer progression. Our efforts to date to study this process have been limited by our technology and, once this process has begun our therapies for these patients are minimally effective. In most cases, while the primary tumor and nodal disease have rich stratification by which we understand patient prognosis, metastatic disease is a binary event, either M0 or M1. This lack of ability to stratify metastatic disease has not, in the past, mattered overmuch as the definitive therapeutic options for patients with M1 disease were limited to systemic agents. Recently, however, we have made advances in our ability to treat oligometastatic disease with minimally or non-invasive local therapies, and we have had suggestions that this actually can, in select patients, influence overall survival3. A greater understanding of metastasis will allow us to optimize current therapies and develop new treatment strategies for this enigmatic process.
I plan to study this complex process in three discrete, but connected, parts and will describe the research plan as such. Phase II is the subject of a recently submitted R21 (1R21CA160127-01) and Phase III is the subject of a funded NCI PS-OC trans-network grant (1U54CA143970-01).
Jacob G. Scott •! H. Lee Moffitt Cancer Center and Research Institute • Evolution of Metastasis • 15 Nov 2010
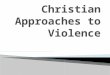
Figure 1: There are three putative routes of intravasation - A. leaky, cooptable endothelium4, B. chimeric vasculature3 and C. motile, invasive tumor cells1.

Phase I: Intravasation - Studying intravasation in vitro or in vivo is exceptionally difficult, which means that this phase of metastasis has been largely understudied. We intend to begin attacking this phase of metastasis beginning from first principals and building an in silico model of this enigmatic process. We hope to eventually be able to validate our results using technologies evolved from the dorsal wound chamber system possessed by our lab.
Overview:To begin the process of hematogenous metastasis, a primary tumor must gain access to and begin to shed tumor cells into the vascular system. How this process happens is the subject of much debate and uncertainty. The subject itself is exceedingly difficult to study in vivo and in vitro but does lend itself well to mathematical models. The proposed methods of intravasation range from a) cells moving through holes in leaky tumor vessels to b) cancer cells evolving to mimic vessel walls an shedding their progeny into the bloodstream to c) actively migrating into the bloodstream4. Each of these processes has been observed under controlled experimental conditions5,6,7, but the process has never been defined rigorously or mechanistically. In this phase of my project I propose to build a hybrid discrete-continuous cellular automaton model of a primary tumor including active local vasculature. The first iterations of this model will include vasculature as only metastatic entrypoints and will be built on work already done in my laboratory8 but this will evolve to include the effect of putative cancer cell chemotactic agents such as EGF and multicellular, multiphenotype, evolvable endothelial cells in addition to the metastatic entrypoint of the vasculature. There is extensive modeling experience available within the IMO, on angiogenesis9, cancer initiation8 and progression10 using these hybrid cellular automata approaches, that I plan to fully utilize for this proposal.
My role in this project:I will be involved approximately 20% of my time in the next two years developing this model of intravasation. I will be directly involved in driving model development and in the interpretation of the results. Determining the phenotypic characteristics of tumor cells that do and do not successfully intravasate and at what time points in the primary tumor’s life cycle will be a major step forward to understanding this initiating event in metastasis. Further, this information can inform the next step of the project, as those cells which intravasate serve as the source for the cells entering into the circulatory phase of metastasis.
Phase II: Circulatory Phase - Little is known about the life history of circulating tumor cells (CTCs) which are putatively the mechanistic agent driving hematogenous metastasis. We have recently submitted an R21 (1R21CA160127-01) on this portion of the project for which I am a co-investigator. The following description includes portions of the R21 grant proposal, which I co-authored.
Overview:In patients with advanced primary cancer, circulating tumor cells (CTCs) can often be found throughout the entire vascular system11. When and where these CTCs create metastasis is not fully understood and is currently the subject of intense biological study. Paget's well-known seed-soil hypothesis12 suggests that in order to understand the spread of metastases, the soil (the site of a metastasis) is as important as the seed (the metastatic cells). Whilst there are some primary tumors that metastasize to organs in a pattern that makes sense from a flow standpoint, there are many others that appear not to follow this deterministic pattern - for example, soft tissue sarcoma preferentially metastasizes to the lung which is the next stop by flow while prostate cancer almost always skips the lung and appears first in the bone. Our central hypothesis is that the CTC population dynamics, as influenced by both filtration fraction and flow patterns, fundamentally influence the spread of metastases. In this study we endeavor to deconvolute the biological complexity inherent in the circulatory phase of metastasis - physical travel constraints, cell biological changes and chemical signaling - and to focus on vascular connections and flow dynamics to uncover novel strategies and techniques to combat this enigmatic and fatal step in cancer progression. We will accomplish this by building
Jacob G. Scott •! H. Lee Moffitt Cancer Center and Research Institute • Evolution of Metastasis • 15 Nov 2010

and comparing two separate mathematical models, based on the same principles but with very different levels of complexity and methods of parametrization. The first will be simple and analytically tenable and understood through measurements of CTCs during a human trial. The second will be complex, requiring evolutionary computing methods to parameterize with published data on metastatic spread.
Specific Aims:
1. Develop a mechanistic, physics inspired model of CTC dynamics based on a simplified vascular network.
a. Characterize the human vascular system as a simple directed network, representing organs as nodes and blood vessels as directed edges. Derive an associated system of coupled ordinary differential equations (ODEs) to describe CTC dynamics as they populate the system, originating from a tumor source. Explore the dynamics of this system of equations and how they characterize CTC population dynamics.
Milestone: characterize theoretical dynamics of the network and system of equations.
b. Experimentally parametrize the model using actual CTC measurements from specific points in the vascular network at specific points in time from a human clinical trial run at Scripps Clinic.
Milestones: define a filtration coefficient (η) for the lung, liver and gut, define a CTC circulation half life.
c. Experimentally parametrize primary tumor characteristics as they relate to CTC shedding (β) by imaging (volumetric), pathologic and phenotypic characteristics.
Milestone: define correlations between physical tumor characteristics and CTC shedding rate (β).
To obtain accurate measurements of CTCs at the different points in the vascular network and in time, we have begun a collaboration with Peter Kuhn at The Scripps Research Institute. Together, we have formulated a
Jacob G. Scott •! H. Lee Moffitt Cancer Center and Research Institute • Evolution of Metastasis • 15 Nov 2010
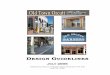
Figure 2. (a) Simplified directed network of human vasculature with nodes representing organs and d i r e c t e d e d g e s r e p r e s e n t i n g a c t u a l vascular connections - starred edges represent sample positions. In this network the primary tumor resides in the Liver. (b) example of a coupled ODE system representing the CTC dynamics of the the d i rec ted ne twork and a s s o c i a t e d a r r e s t e d populations in the nodes. * A r e p r e s e n t s t h e p e r i p h e r a l a r t e r i a l circulation, *B represents the portal vein and *C represents the inferior vena cava

clinical trial studying the value of CTC measurements in the staging of Hepatocellular Carcinoma (HCC). This trial endeavors to understand the relationship between CTC measurements before, during and after attempted curative liver transplantation and clinical outcomes.
Scripps has developed a fluid phase biopsy approach that is able to identify CTCs without the need for surface receptor-based enrichment. This method has been used for a number of morphologic studies13,14 of CTCs and has been shown to be extremely sensitive and specific. This method will be employed in the trial of patients with HCC during which blood draws will be assayed for the presence of CTCs. Blood will be drawn from each of the starred edges (points *A, *B and *C) in figure 2, surrounding the most highly connected organs, before surgery and immediately after resection of the primary tumor. Further, peripheral venous blood (*C) will be drawn at several points during the recovery and follow up period. These data, as well as other clinical, histopathologic and radiologic data will be built into the model in Aim 1.
2. Develop a complex network model of metastasis based on a more complete vascular network.
a. Characterize the human vascular system as a directed network with cancer relevant organs as nodes and blood vessels as edges. Derive an associated system of coupled ordinary differential equations (ODEs) to describe patterns of metastatic spread.
Milestone: produce a complex network model encompassing all relevant organs.
b. Parametrize this more complex network with extant observational data on clinical metastatic spread using a genetic algorithm
Milestone: create a genetic algorithm to evolve parameter sets to match clinical data on metastatic spread for each of approximately 20 tumor initiating sites.
3. Determine how patterns of metastatic spread correlate with CTC measurements and vascular connections in the prediction of clinical cancer metastasis.
a. Compare experimentally parametrized model with clinically parametrized model.Milestone: determine the importance of CTC dynamics and organ filtration parameter measurement in the prediction of metastatic spread.
My role in this project: I intend to spend approximately 50% of my time for the next two years on this portion of the work. I will function as project liaison to the clinical trial and prime mover on the model development for aims 1 and 2. This project is based on a novel method of modeling metastasis of my own creation which was born of my background in physics and systems engineering coupled with my clinical cancer training.
Jacob G. Scott •! H. Lee Moffitt Cancer Center and Research Institute • Evolution of Metastasis • 15 Nov 2010
!
Figure 2: Schematic of project. Outlining Aim 1 - simplistic network model of CTC dynamics parametrized by human clinical trial at Scripps. Aim 2 - complex model of metastasis based on flow inspired rules and published medical data fit with a separate genetic algorithm for each cancer subtype. Aim 3 - Explore similarities and differences in model parameters.

Phase III: Extravasation and Colony Formation - This phase of research will be in the form of experiments derived from theoretical work that I have already done with collaborators from MIT15. In this project, awarded a grant from the NCI (Trans-network supplement to 1U54CA143970-01), we endeavor to understand the role of passenger mutations in the determination of metastatic fitness.
Overview:
It is well known that many patients can have subclinical metastases if their bone marrow is analyzed, yet these patients do not necessarily progress to clinically evident metastatic disease. We currently have no test to determine which patients harbor clinically important metastases - which would become widely metastatic. Work done by Klein et al. analyzing insertion and deletion patterns in individual metastatic cells, has been shown that 1) there exists a large amount of genomic diversity in these colonizing cells, and 2) the colonies have a genomic history suggestive of a population bottleneck and selective sweeps common in evolving populations16. Population genetics have been used to study primary tumor growth by mathematically relating the balance between driver mutations, or mutations in cancer causing pathways that bring about the tumorogenic phenotype, and passenger mutations, or mutations across the genome in pathways unrelated to cancer that arise by hitchiking to driver mutations. This balance between drivers and passengers is critical in determining whether the early tumor progresses to invasive cancer or diminishes to extinction.
We have begun theoretical work in which we used a similar approach that contained significant genetic heterogeneity in the primary tumors and metastasizing cells to gain new insights into the metastatic process and to better understand why some tumors are more able to succeed after arresting in a foreign stroma than others15. Our initial model showed that the probability of a tumor producing successful metastases is correlated with both primary tumor factors (e.g.: tumor size and age as well as the mutational spectrum of the cancer) and also factors relating to the new microenvironment in which the metastases grow (e.g. pH and
Jacob G. Scott •! H. Lee Moffitt Cancer Center and Research Institute • Evolution of Metastasis • 15 Nov 2010
Figure 3. Model overview showing primary tumor model of fitness function modified by stochastically accrued driver and passenger mutations with m o d i fi c a t i o n t o i n c l u d e evolution in foreign stroma. Model prediction that greater mutational load leads to lesser metastatic fitness. In vitro and in vivo biological results showing cells grown in mutagenic and clastogenic c o n d i t i o n s f o r m a n y generat ions exhibi t less metastatic and migrational fitness

oxygen availability). Many of these factors, along with the molecular properties of the passenger mutations, may be exploited by therapies. Our underlying hypothesis is that more mutations leads to more passengers which, in turn, leads to less metastatic fitness.
Our experimental plan involves subjecting luciferase transfected human cancer cells (both MDA-mb-231_luc and MCF-10a_luc_Her2) to differential levels of mutagenic exposure. The resultant cells will then be subjected to in vitro migration assays and in vivo metastasis assays to ascertain their phenotypic metastatic fitness. The cells found to have the widest variation in metastatic fitness will then have their genotypes analyzed to determine mutation load. Molecular methods will be used to detect mutations in the coding regions (full exome sequencing) and copy-number alterations (SNP-array) allowing us to correlate metastatic phenotype with number and severity of passenger and driver mutations using previously developed bioinformatic approaches. My role in this project:I conceived of the theoretical work which led to the hypothesis for this project and I am a co-investigator on the already awarded NCI trans-network PS-OC grant. I will spend approximately 30% of my time over the next two years on this portion of the project. I will be instrumental in the modeling as well as the experimental aspects of this project. I will be involved in the in vitro and in vivo biological experiments and will be a prime mover in the model building as well as the data analysis (in silico). We have two manuscripts in preparation at this time (one theoretical and one biological) and I share the first author position on both.
Summary/Big Picture:
Metastasis is complex, but I hope to come to a deeper understanding of it by reducing it to a series of simpler, more tenable steps. Each of these steps will be studied initially as stand alone processes, but with the end goal being to integrate them into a cohesive suite of models of metastasis. I hope to be able to view this suite of models as a single entity to better understand the process and to elucidate weak points in the cascade that would be amenable to intervention. While working on these projects I will be walking in the clinical, basic scientific and theoretical worlds equally. I will be serving to sharpen my skills as a researcher and working toward a research based doctoral degree. The combination of these experiences and endeavors will give me the skills that I need to be reach my goal of being an effective physician-scientist.
References:
1. Scott JG, et al. Int J Radiat Oncol Biol Phys. Epub 2010 Jul 312. Scott JG, et al. in press, NeuroOncology3. Milano MT, et al. Cancer 2008, Feb 1; 112(3):650-8. PMID: 180722604. Bockhorn M, et al. Lancet Oncology 2007, 8(5):444. PMID: 174669023. Wyckoff JB, et al. Cancer Research 2007,67(6):2649. PMID: 173635854. Chang YS, et al. Proc Natl Acad Sci USA; 2009. 97(26):14608-14613. PMID: 111210635. Mazzone M, et al. Cell 2009, 136(5):839 PMID: 192171506. Basanta D, et al. Cancer Res. Sep 1;69 (17):7111-20. PMID: 197067777. Chaplain MA, et al. Annu Rev Biomed Eng. 2006;8:233-57. PMID: 16834556 8. Anderson A. R. A., et al. Cell 2006; 127, 905- 915. PMID: 171297789. Jiao LR, et al. J Clin Oncol; Dec 20; 27(36):6160-5. PMID: 1988452910.Paget S. Lancet 1889; 1:571-57311.Marrinucci D, et al. J Oncol 2010; 861341. PMID: 2011174312.Marrinucci D, et al. Arch Pathol Lab Med; 2009;133(9):1468-1471 PMID: 1972275713.McFarland C, Scott JG. et al. Koch Symposium, Boston MA, 2010 Jun 1014.Klein CA, et al. Lancet 2002, 360(9334):683. PMID: 12241875
Jacob G. Scott •! H. Lee Moffitt Cancer Center and Research Institute • Evolution of Metastasis • 15 Nov 2010