Embed Size (px)
Citation preview

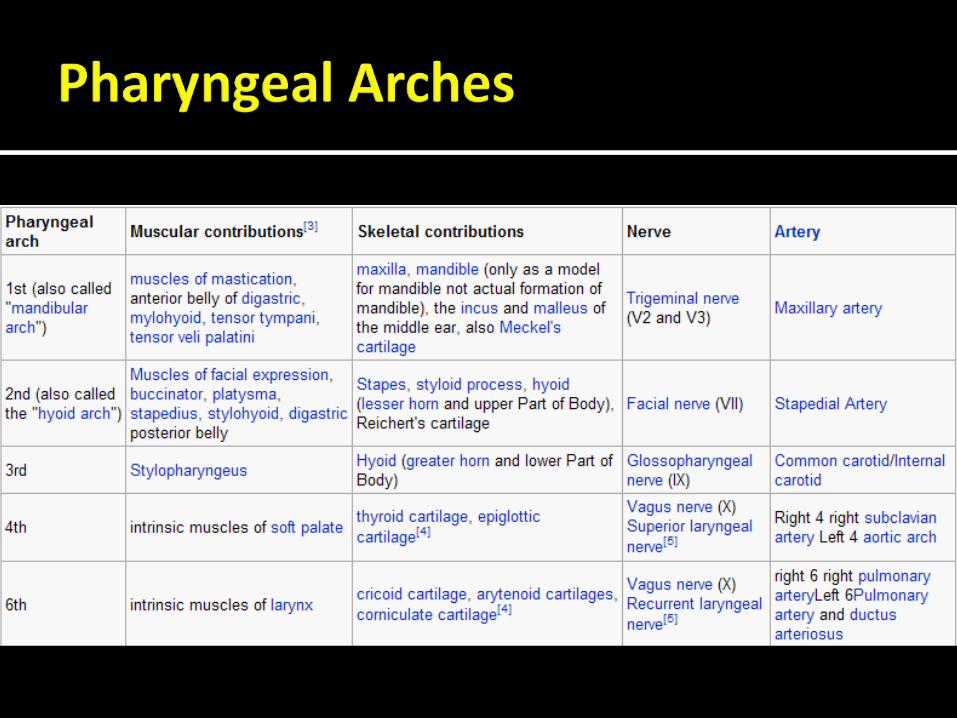
Dr. Lana Obeidat
Development of the Face 4 weeks in utero
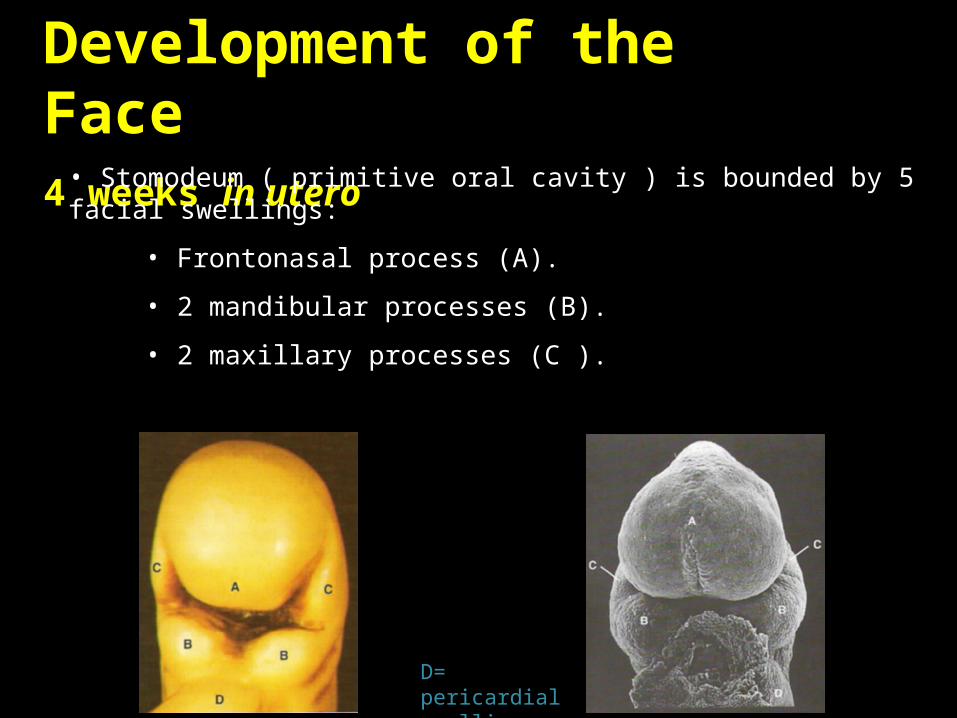
• Stomodeum ( primitive oral cavity ) is bounded by 5 facial swellings:
• Frontonasal process (A).
• 2 mandibular processes (B).
• 2 maxillary processes (C ).
D= pericardial swelling
The facial processes are demarcated by grooves that become flattened out by the proliferative and migratory activity of the underlying mesenchyme
Development of the Face 4 weeks in utero
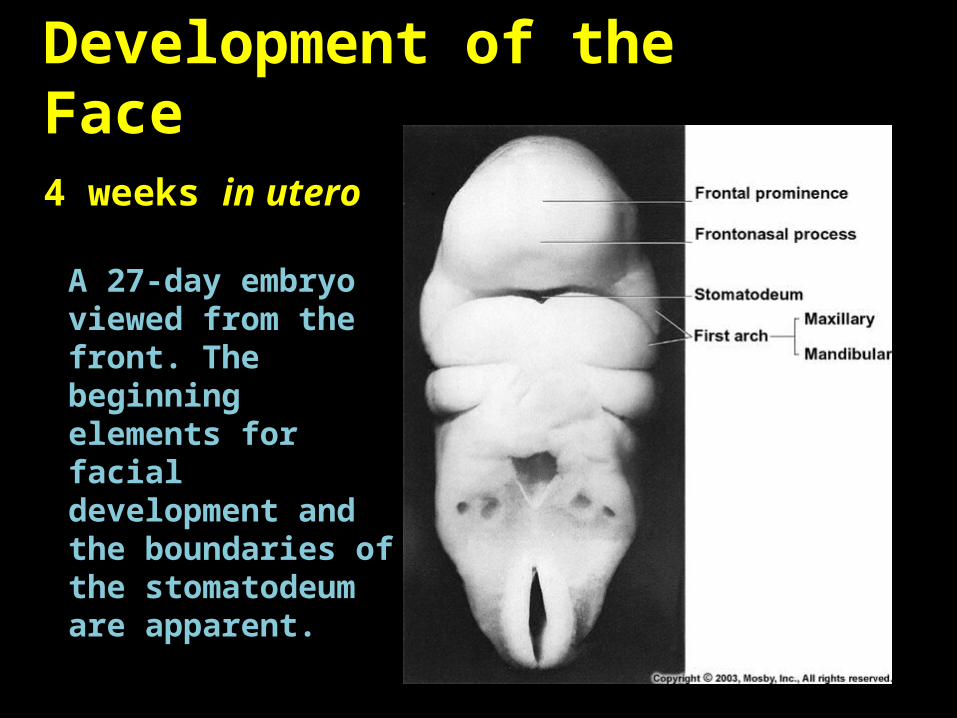
A 27-day embryo viewed from the front. The beginning elements for facial development and the boundaries of the stomatodeum are apparent.
Development of the Face 4 weeks in utero
• The oropharyngeal (buccopharyngeal) membrane separates the oral cavity from the pharynx.
• Bilaminar membrane:
• Outer ectodermal layer.
• Inner endodermal layer.
• The membrane breaks down leaving a continuity between the ectodermally lined oral cavity and the endodermally lined pharynx.

Development of the Face 4 weeks in utero

Development of the Face 5 weeks in utero
• Nasal and optic placodes arise from thickening of the ectoderm.
• Nasal placodes sink into the mesenchyme forming 2 blind ended nasal pits.
• Proliferation of mesenchyme from the frontonasal process around the openings of the nasal pits produces the medial and lateral nasal processes.
•Maxillary processes will enlarge and grow forwards and medially
A Optic placode
B Nasal pit
C Medial nasal process
D Lateral nasal process
E Maxillary process
F Mandibular process
G 2nd branchial arch

Development of the Face 5 weeks in utero
A 34-day embryo viewed from the front. The nasal pits have formed, thereby delineating the lateral and medial nasal processes.
Development of the Face 5 weeks in utero
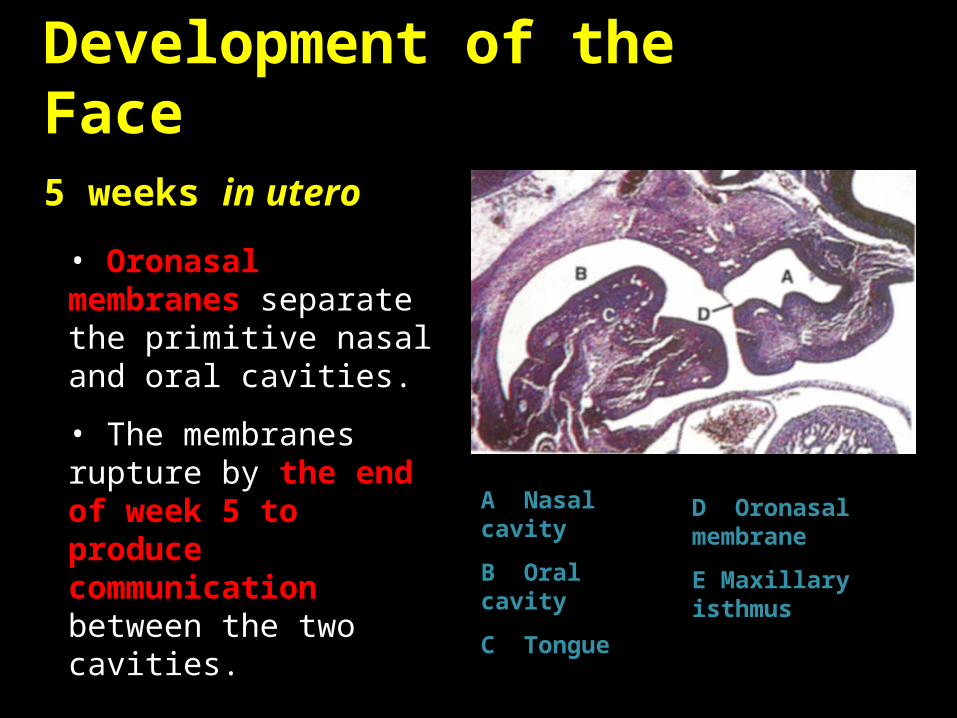
• Oronasal membranes separate the primitive nasal and oral cavities.
• The membranes rupture by the end of week 5 to produce communication between the two cavities. A Nasal cavity
B Oral cavity
C Tongue
D Oronasal membrane
E Maxillary isthmus
Development of the Face 5 weeks in utero
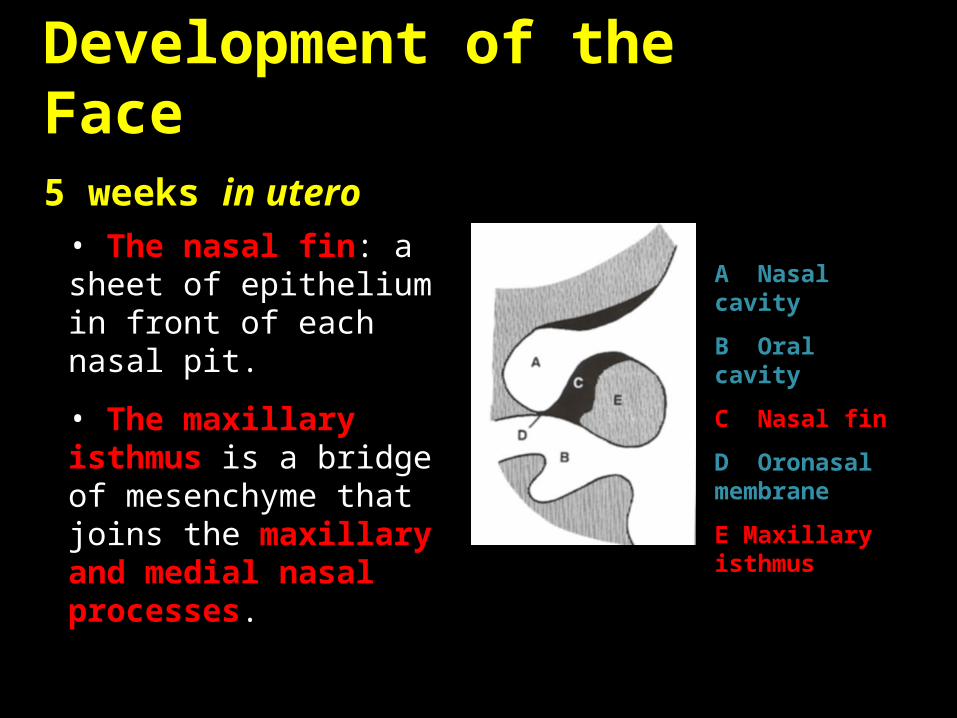
• The nasal fin: a sheet of epithelium in front of each nasal pit.
• The maxillary isthmus is a bridge of mesenchyme that joins the maxillary and medial nasal processes.
A Nasal cavity
B Oral cavity
C Nasal fin
D Oronasal membrane
E Maxillary isthmus
Development of the Face 6 weeks in utero
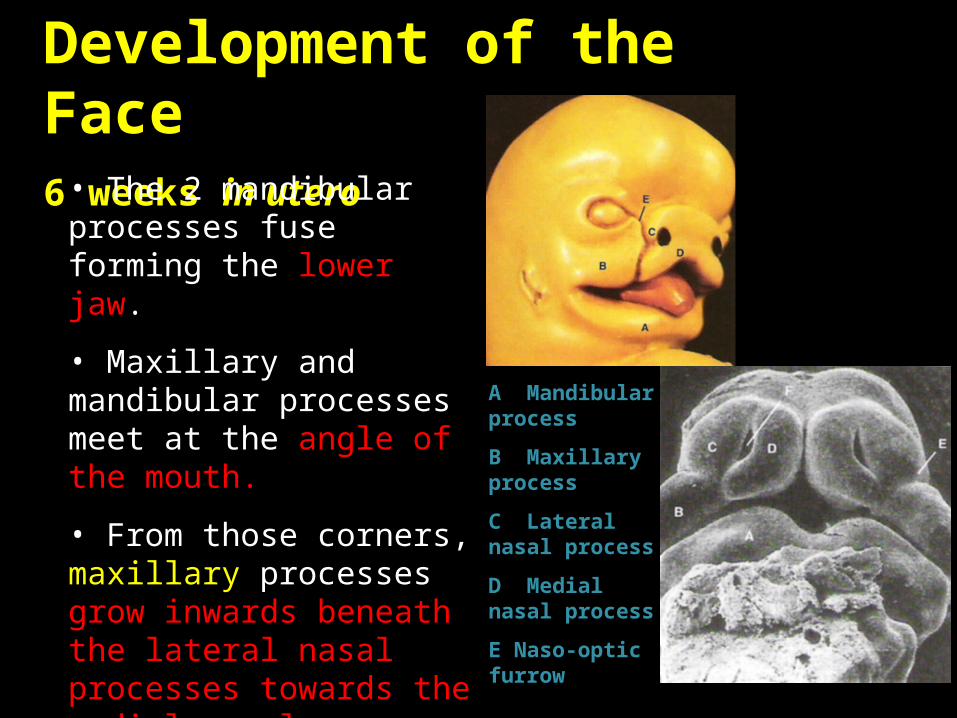
• The 2 mandibular processes fuse forming the lower jaw.
• Maxillary and mandibular processes meet at the angle of the mouth.
• From those corners, maxillary processes grow inwards beneath the lateral nasal processes towards the medial nasal processes.
A Mandibular process
B Maxillary process
C Lateral nasal process
D Medial nasal process
E Naso-optic furrow
Development of the Face 6 weeks in utero
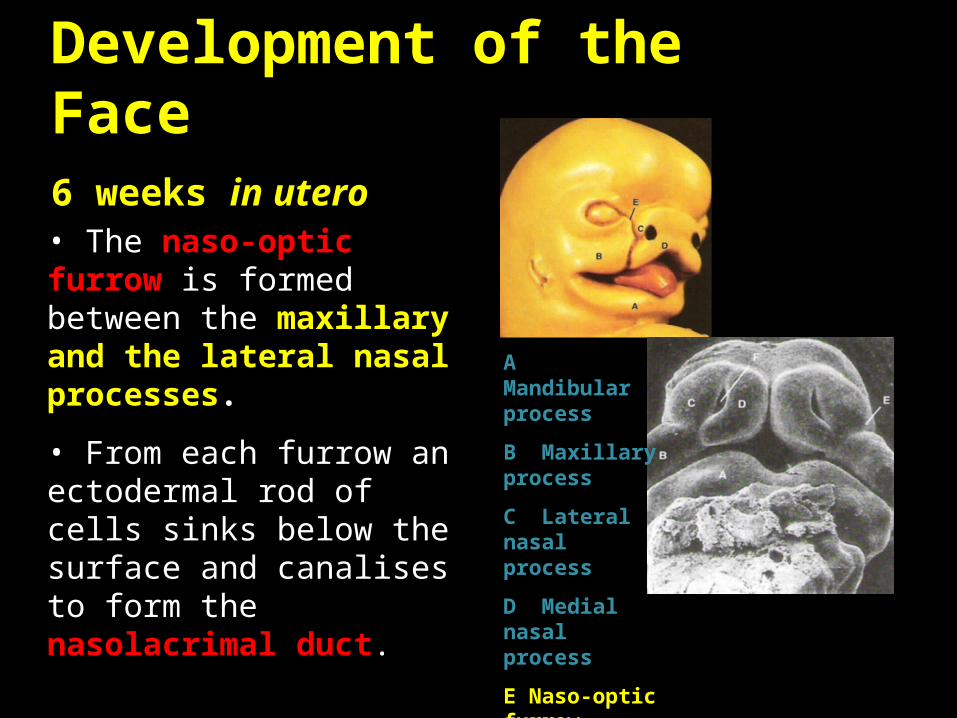
• The naso-optic furrow is formed between the maxillary and the lateral nasal processes.
• From each furrow an ectodermal rod of cells sinks below the surface and canalises to form the nasolacrimal duct.
A Mandibular process
B Maxillary process
C Lateral nasal process
D Medial nasal process
E Naso-optic furrow
Clinical Considerations
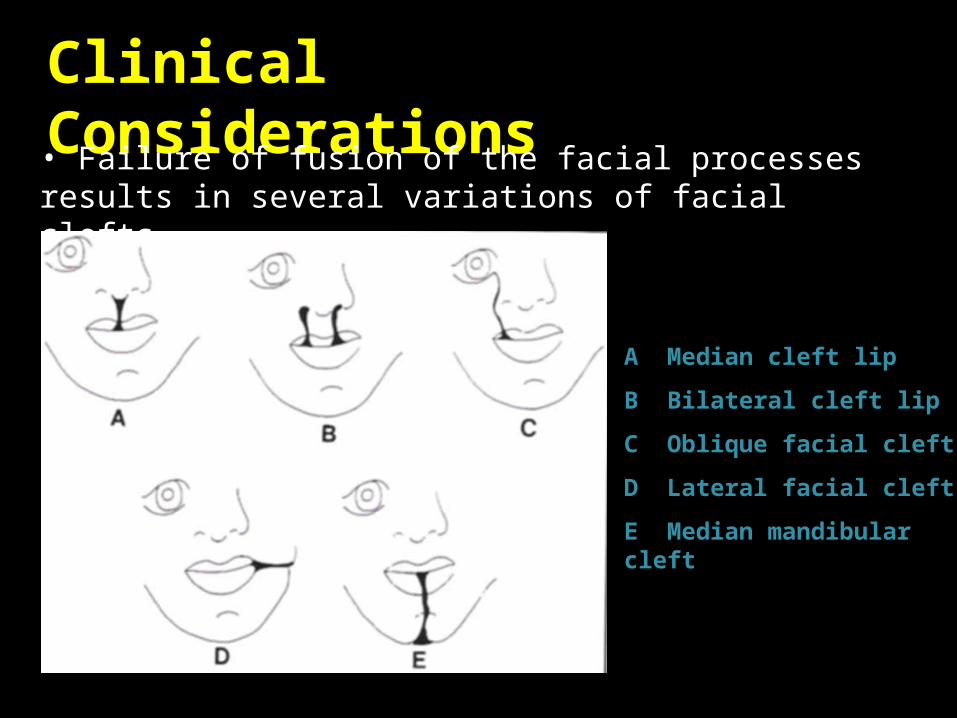
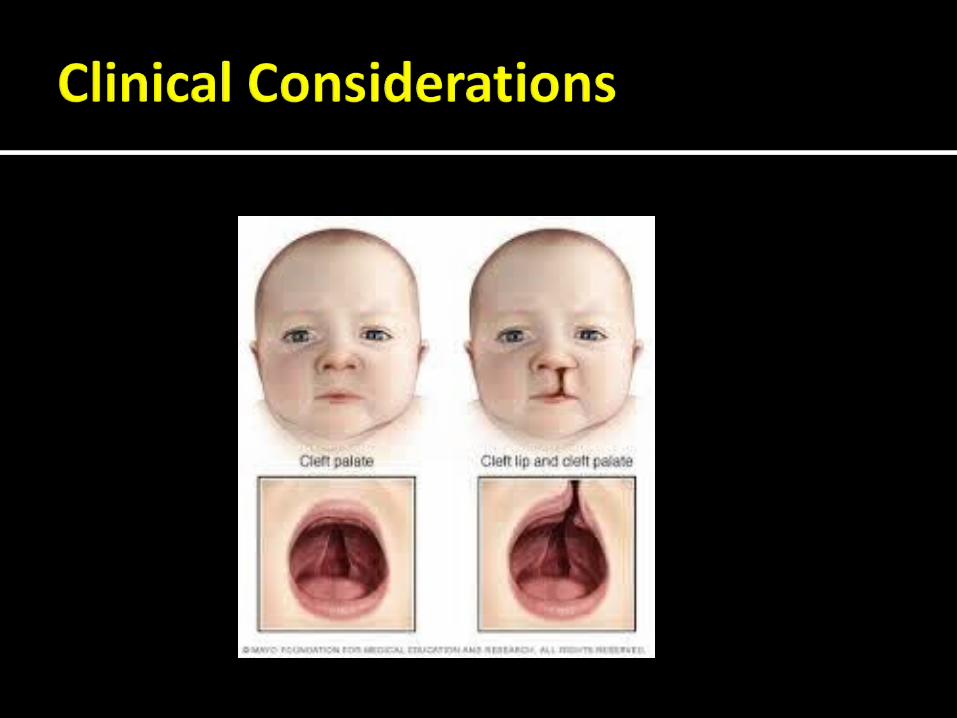
• Failure of fusion of the facial processes results in several variations of facial clefts.
A Median cleft lip
B Bilateral cleft lip
C Oblique facial cleft
D Lateral facial cleft
E Median mandibular cleft

Failure of fusion of the maxillary and medial nasal processes produce : Cleft lip Which maybe unilateral or bilateral
Failure of the medial nasal processes may be responsible for the formation of median cleft lip
Clefts are of multi-factorial aetiology associated with both genetic and environmental disturbances
It occurs in the 6th and 7th weeks of intrauterine life

This defect is characterized by a "light" furrow along the vertical length of the lip with a small vermilion notch and minor imperfections

By definition, it has an intact nasal sill, commonly termed the Simonart band.

This involves the full-thickness defect of the lip and alveolus, extends into the base of the nose and is often accompanied by a palatal cleft.
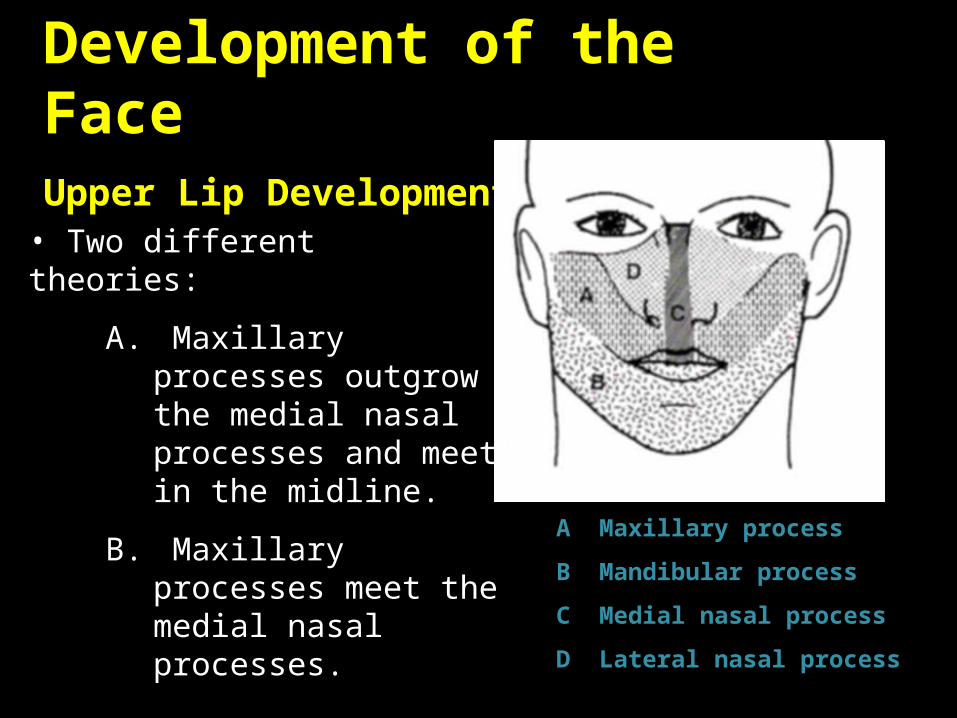
Development of the Face Upper Lip Development
A Maxillary process
B Mandibular process
C Medial nasal process
D Lateral nasal process
• Two different theories:
A. Maxillary processes outgrow the medial nasal processes and meet in the midline.
B. Maxillary processes meet the medial nasal processes.

Development of the Palate
• During the 6th week of intrauterine life, the nasal cavities are separated by a nasal septum.
• The nasal cavities are separated from the oral cavity by the primary palate.
• The nasal septum and the primary palate are derivatives of the frontonasal process.
A Primary nasal cavities
B Primary nasal septum
C Primary palate
6 weeks in utero

Development of the Palate
• 2 lateral palatal shelves develop behind the primary palate.
• The lateral palatal shelves are derived form the maxillary processes.
• The secondary nasal septum develops behind the primary septum.
A Lateral palatal shelves
B Primary palate
C Secondary nasal septum
6 weeks in utero
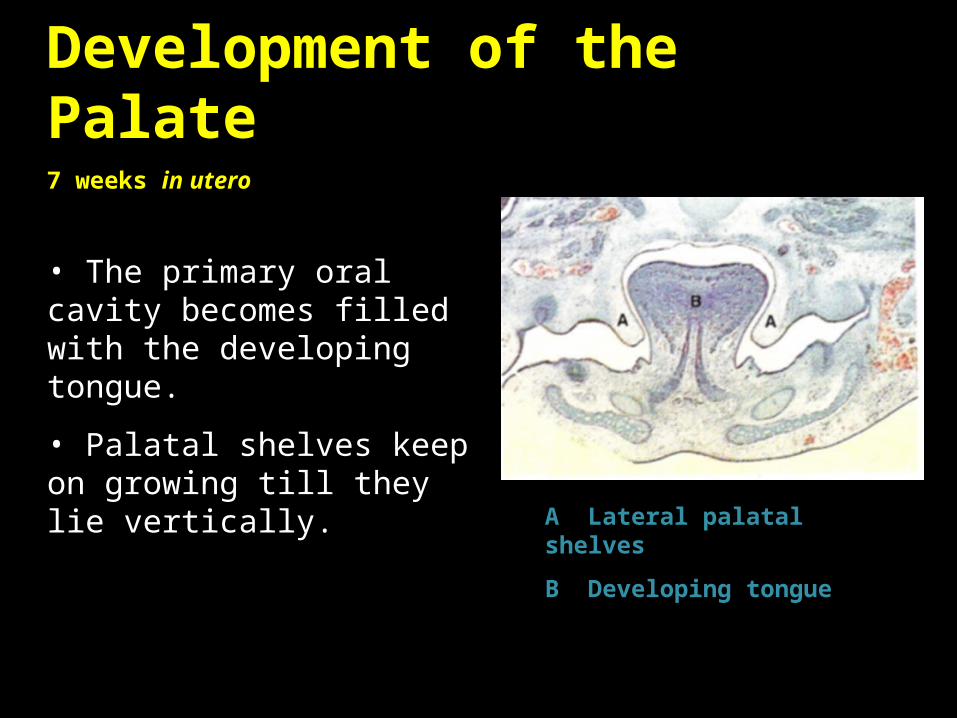
Development of the Palate7 weeks in utero
• The primary oral cavity becomes filled with the developing tongue.
• Palatal shelves keep on growing till they lie vertically.
A Lateral palatal shelves
B Developing tongue
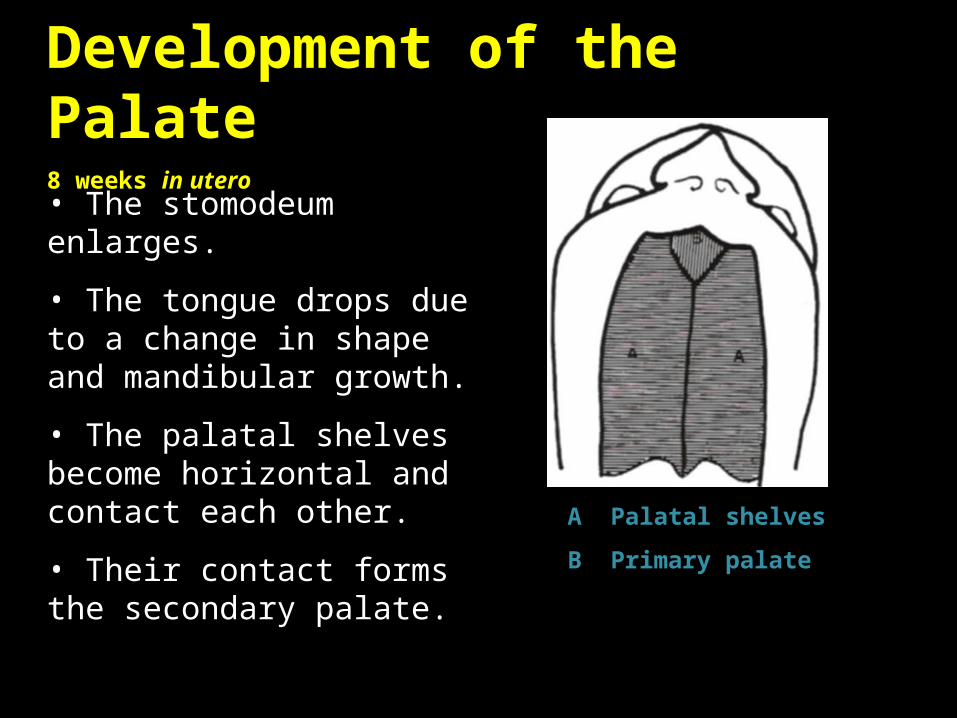
Development of the Palate8 weeks in utero
• The stomodeum enlarges.
• The tongue drops due to a change in shape and mandibular growth.
• The palatal shelves become horizontal and contact each other.
• Their contact forms the secondary palate.
A Palatal shelves
B Primary palate
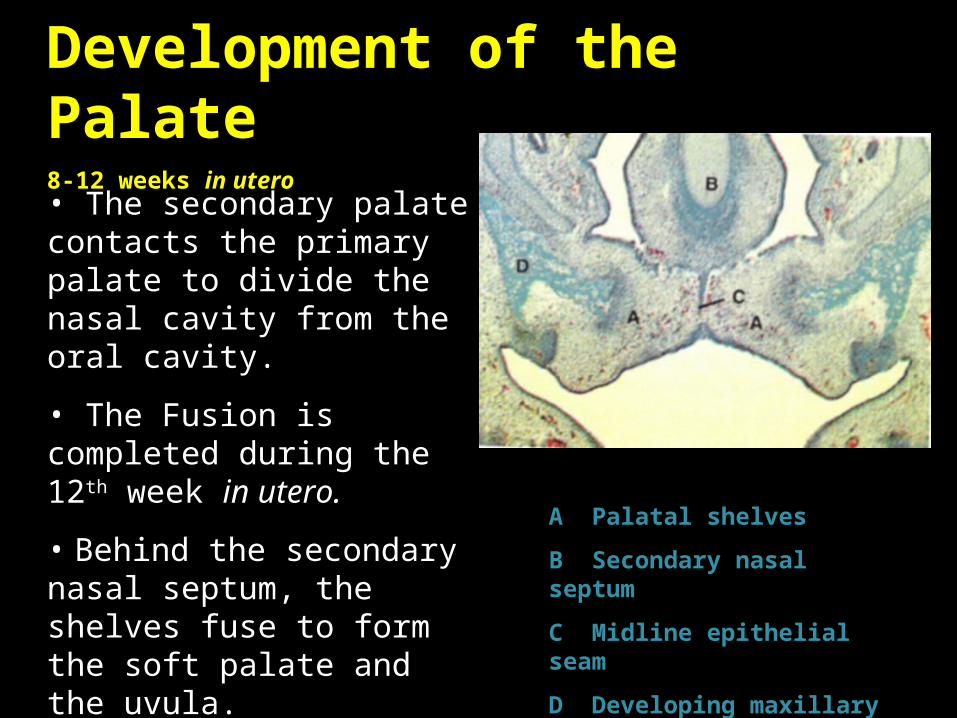
Development of the Palate8-12 weeks in utero
• The secondary palate contacts the primary palate to divide the nasal cavity from the oral cavity.
• The Fusion is completed during the 12th week in utero.
• Behind the secondary nasal septum, the shelves fuse to form the soft palate and the uvula.
A Palatal shelves
B Secondary nasal septum
C Midline epithelial seam
D Developing maxillary bone
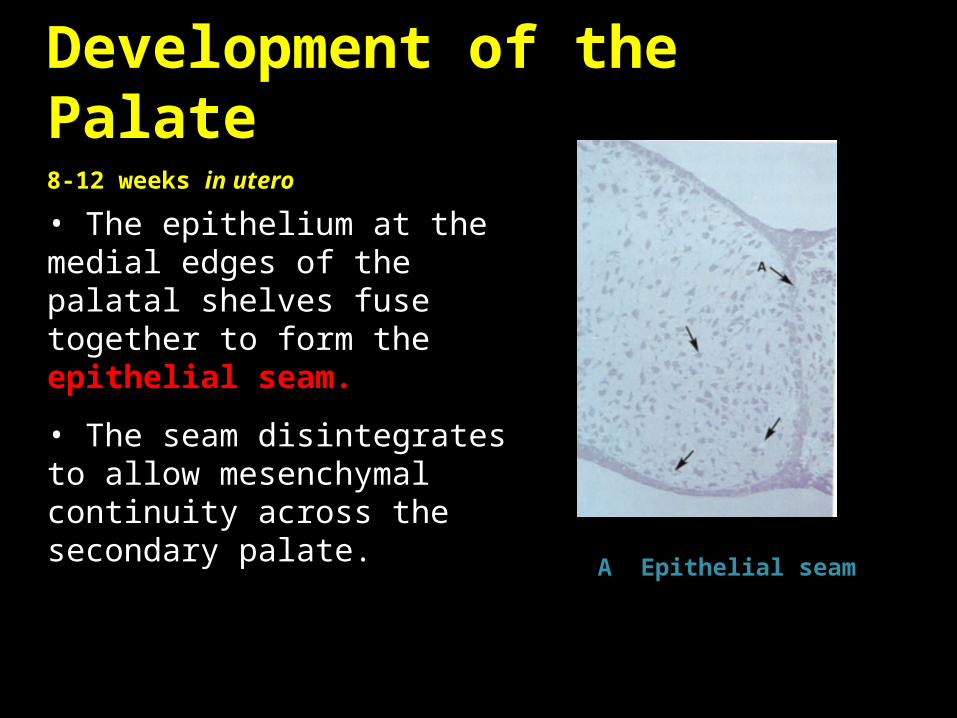
Development of the Palate8-12 weeks in utero
• The epithelium at the medial edges of the palatal shelves fuse together to form the epithelial seam.
• The seam disintegrates to allow mesenchymal continuity across the secondary palate.
A Epithelial seam
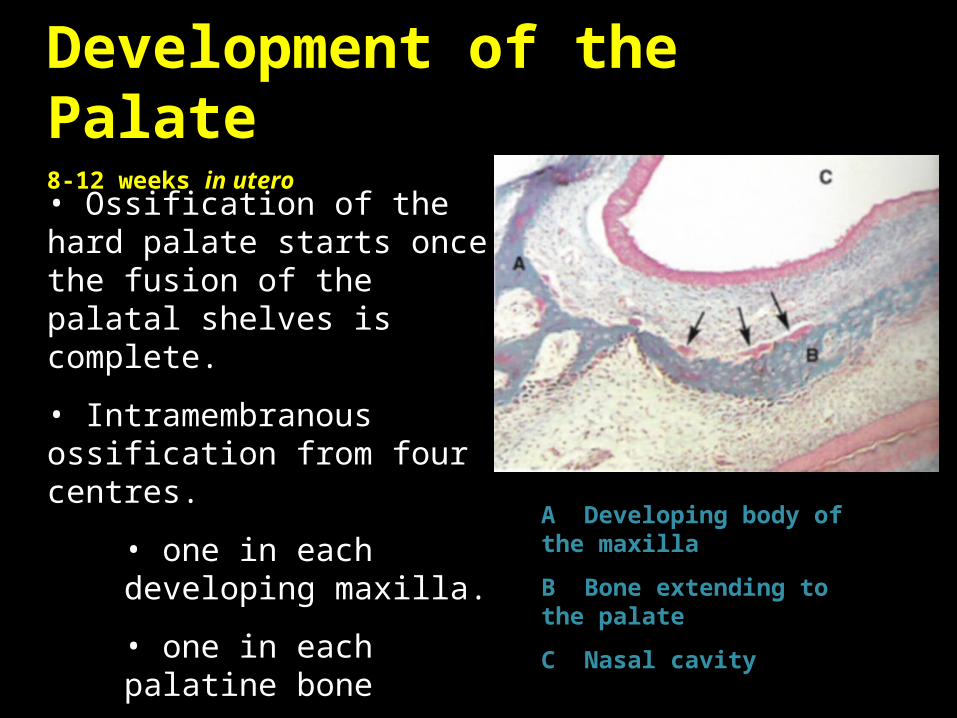
Development of the Palate8-12 weeks in utero
• Ossification of the hard palate starts once the fusion of the palatal shelves is complete.
• Intramembranous ossification from four centres.
• one in each developing maxilla.
• one in each palatine bone
A Developing body of the maxilla
B Bone extending to the palate
C Nasal cavity
Development of the Palate8-12 weeks in utero
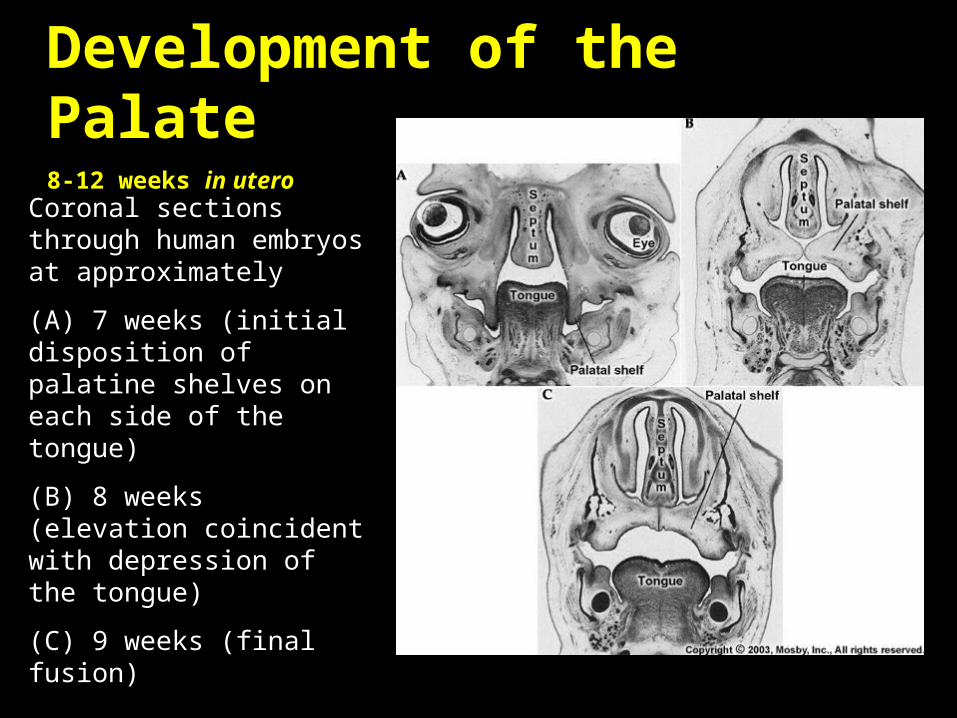
Coronal sections through human embryos at approximately
(A) 7 weeks (initial disposition of palatine shelves on each side of the tongue)
(B) 8 weeks (elevation coincident with depression of the tongue)
(C) 9 weeks (final fusion)
at 4-7 weeks gestation, is necessary for the normal development of embryonic facial structures. When migration and fusion are interrupted for any reason, a facial cleft develops along embryonic fusion lines.
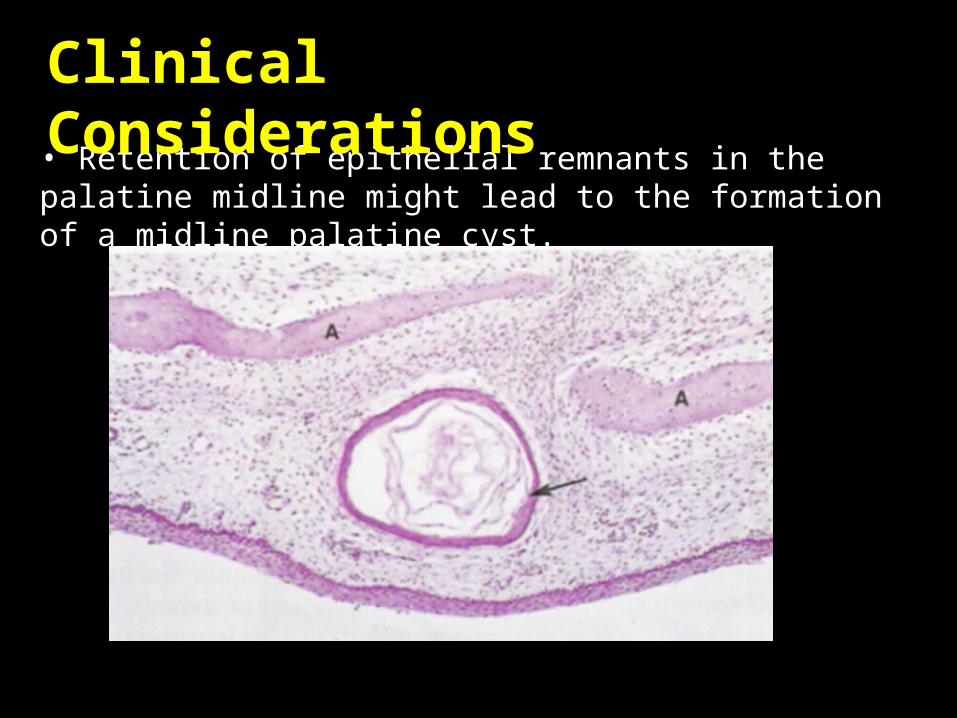
• Retention of epithelial remnants in the palatine midline might lead to the formation of a midline palatine cyst.
Clinical Considerations
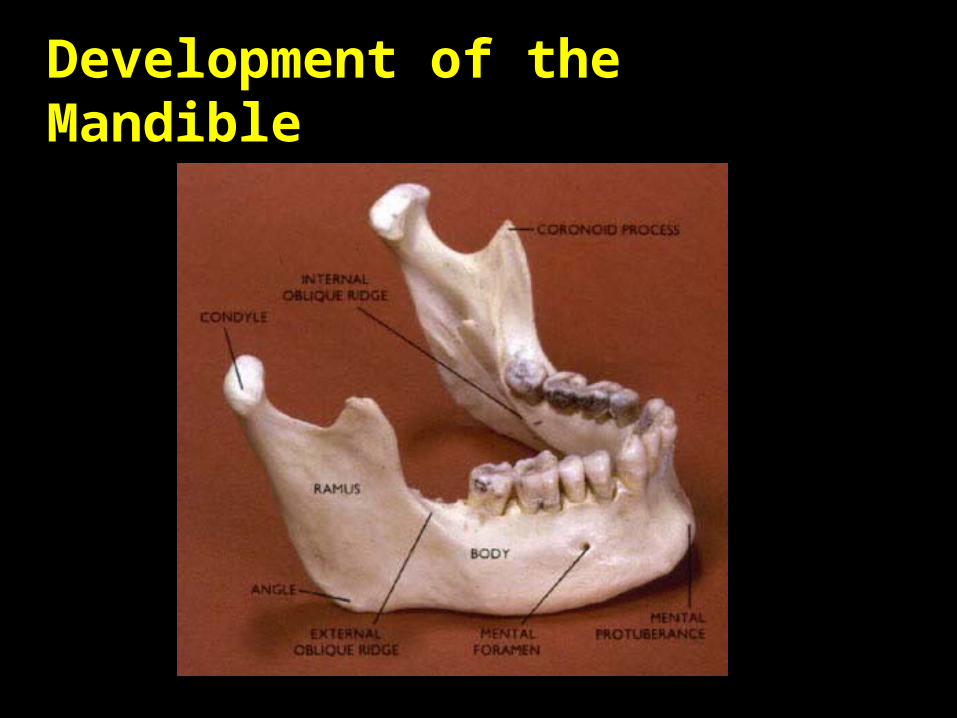
Development of the Mandible
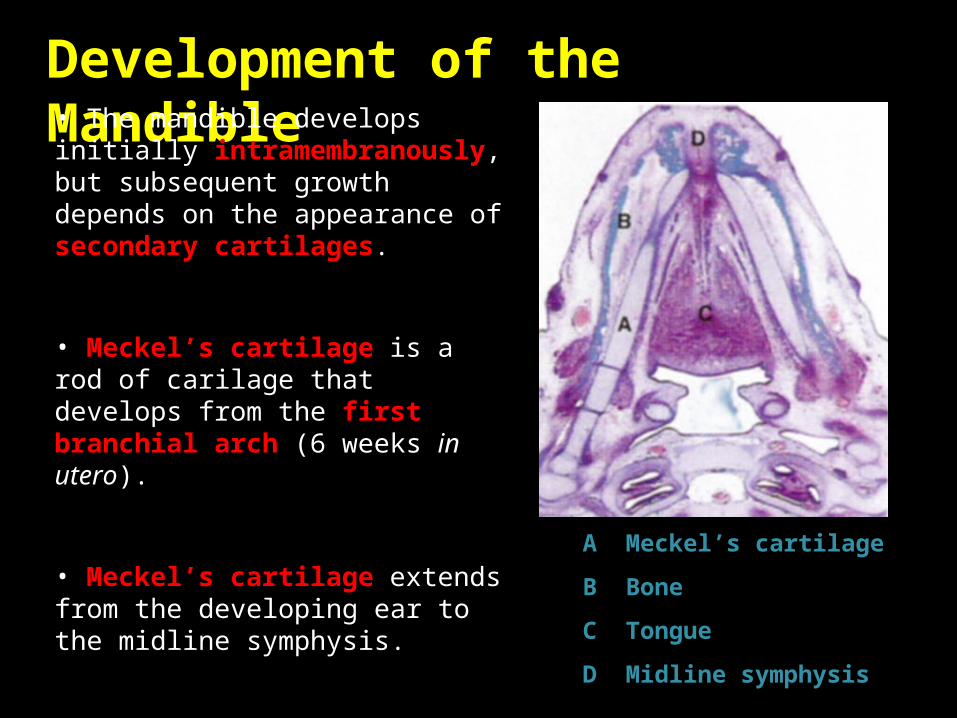
Development of the Mandible • The mandible develops initially intramembranously, but subsequent growth depends on the appearance of secondary cartilages.
• Meckel’s cartilage is a rod of carilage that develops from the first branchial arch (6 weeks in utero).
• Meckel’s cartilage extends from the developing ear to the midline symphysis.
• Acts as a framework for the bone of the mandible forms.
A Meckel’s cartilage
B Bone
C Tongue
D Midline symphysis
Development of the Mandible
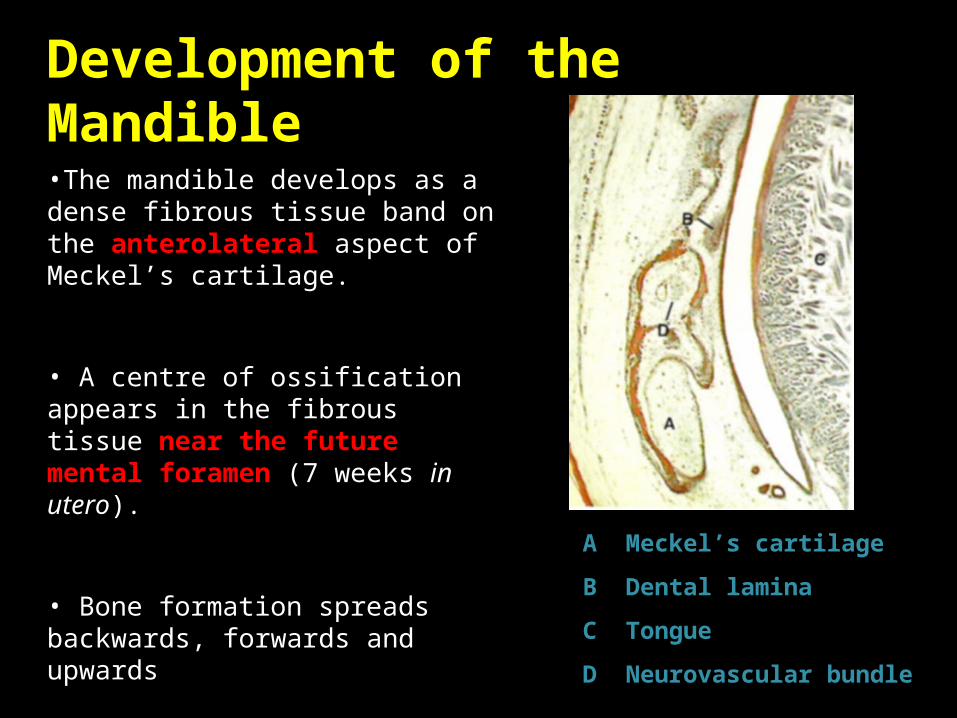
•The mandible develops as a dense fibrous tissue band on the anterolateral aspect of Meckel’s cartilage.
• A centre of ossification appears in the fibrous tissue near the future mental foramen (7 weeks in utero).
• Bone formation spreads backwards, forwards and upwards
A Meckel’s cartilage
B Dental lamina
C Tongue
D Neurovascular bundle
Development of the Mandible
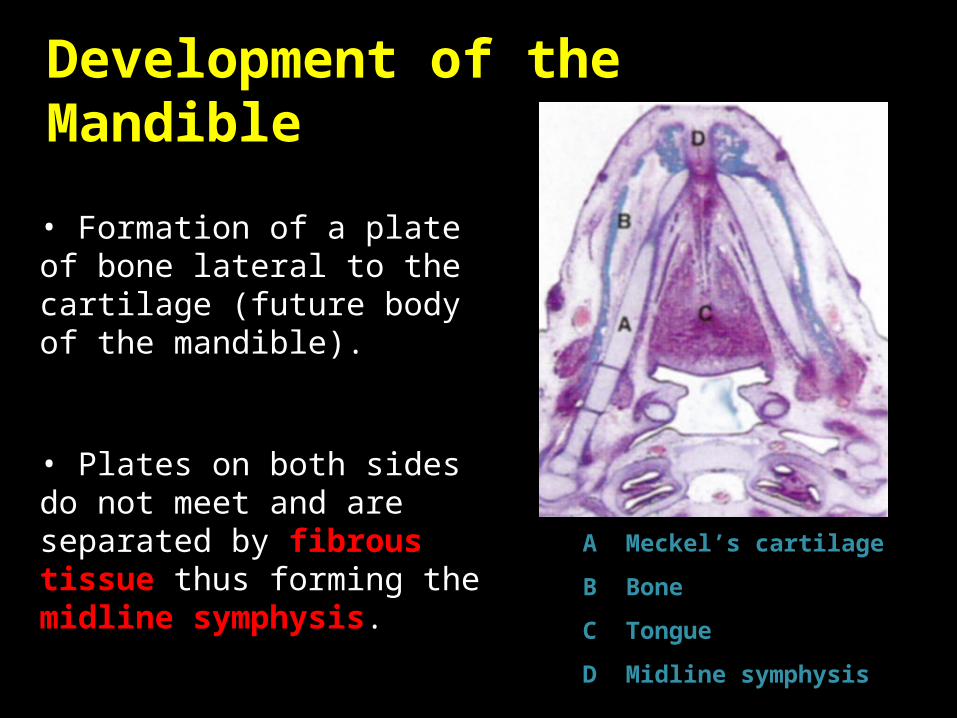
• Formation of a plate of bone lateral to the cartilage (future body of the mandible).
• Plates on both sides do not meet and are separated by fibrous tissue thus forming the midline symphysis. A Meckel’s cartilage
B Bone
C Tongue
D Midline symphysis

Development of the Mandible
• Continued bone formation leads to an increase in the size of the mandible.
• Formation of the alveolar process around the developing tooth buds.
• Neurovascular bundle starts to be surrounded by bone.
A Alveolar process
B Neurovascular bundle
C Meckel’s cartilage
D Tongue
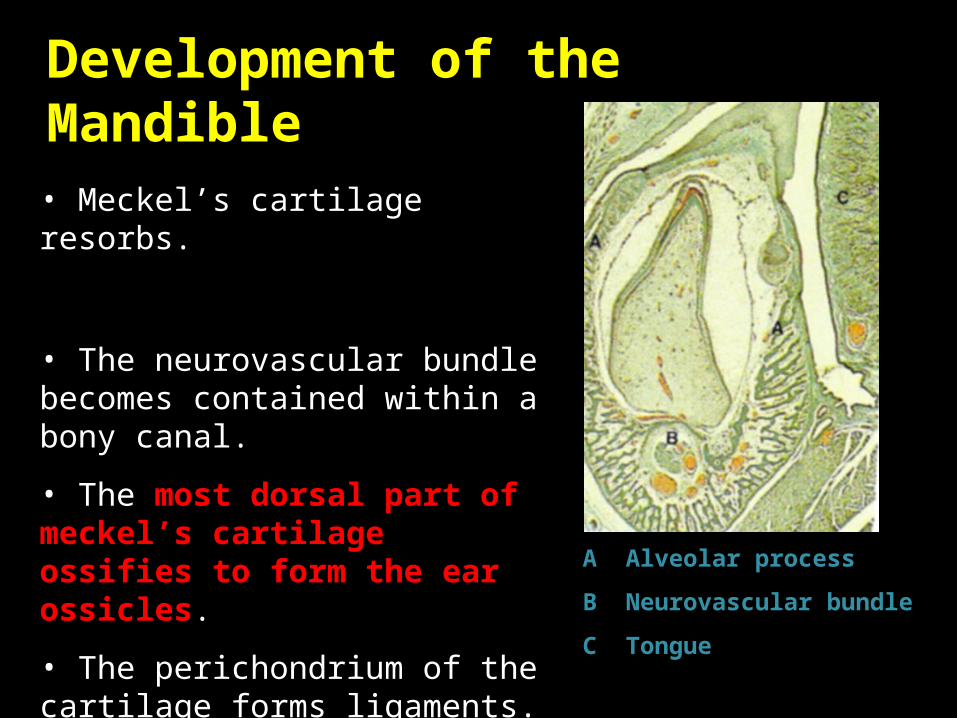
Development of the Mandible
• Meckel’s cartilage resorbs.
• The neurovascular bundle becomes contained within a bony canal.
• The most dorsal part of meckel’s cartilage ossifies to form the ear ossicles.
• The perichondrium of the cartilage forms ligaments.
A Alveolar process
B Neurovascular bundle
C Tongue

malleus, incus : originates from First pharyngeal arch
Stapes: originates from second pharyngeal arch
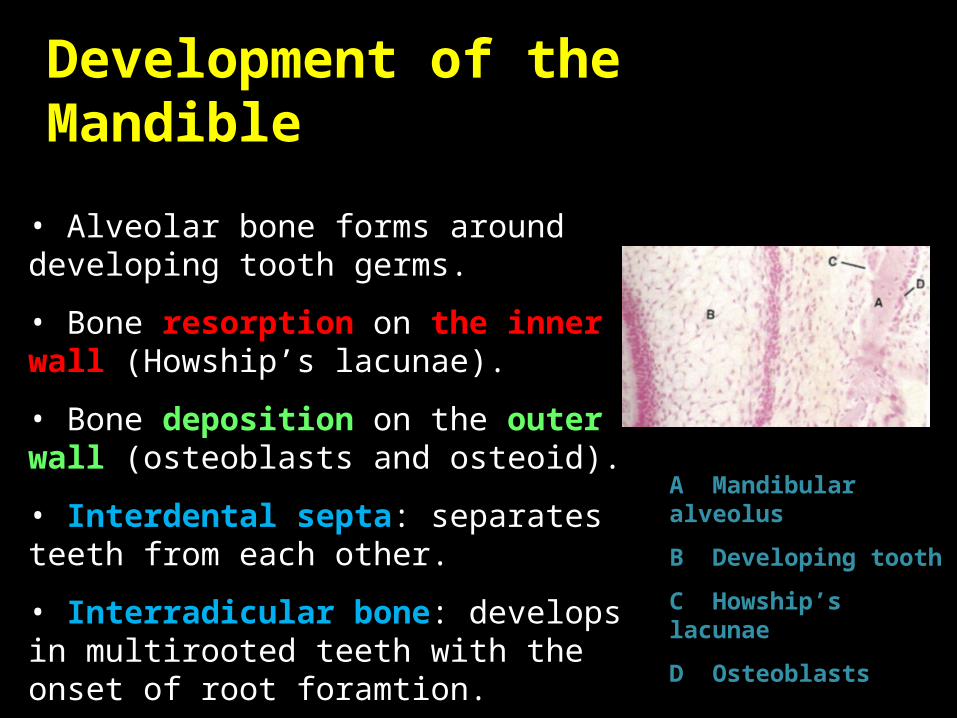
Development of the Mandible
• Alveolar bone forms around developing tooth germs.
• Bone resorption on the inner wall (Howship’s lacunae).
• Bone deposition on the outer wall (osteoblasts and osteoid).
• Interdental septa: separates teeth from each other.
• Interradicular bone: develops in multirooted teeth with the onset of root foramtion.
A Mandibular alveolus
B Developing tooth
C Howship’s lacunae
D Osteoblasts
Development of the Mandible
• The ramus of the mandible develops as a fibro-cellular condensation.
• Continuous with the body of the mandible.
• Backwards spread of ossification.
• Appearance of 3 secondary cartilages (10-14 weeks in utero).
• The condylar cartilage is the main one, and there are other carilages associated with the coronoid processes and in the region of the mandibular symphysis.

Development of the Mandible

Development of the Mandible
• The condylar cartilage appears beneath the fibrous articular layer of the future condyle.
• The temporomandibular joint develops from mesenchyme between the temporal bone and the developing condyle.
• The upper and lower joint cavities appear as clefts during the 12th week in utero.
• Remaining mesenchyme becomes the articular disc.
• Joint capsule. A Condylar cartilage
B Meckel’s cartilage
C Bone of the mandibular fossa
D Developing articular disc
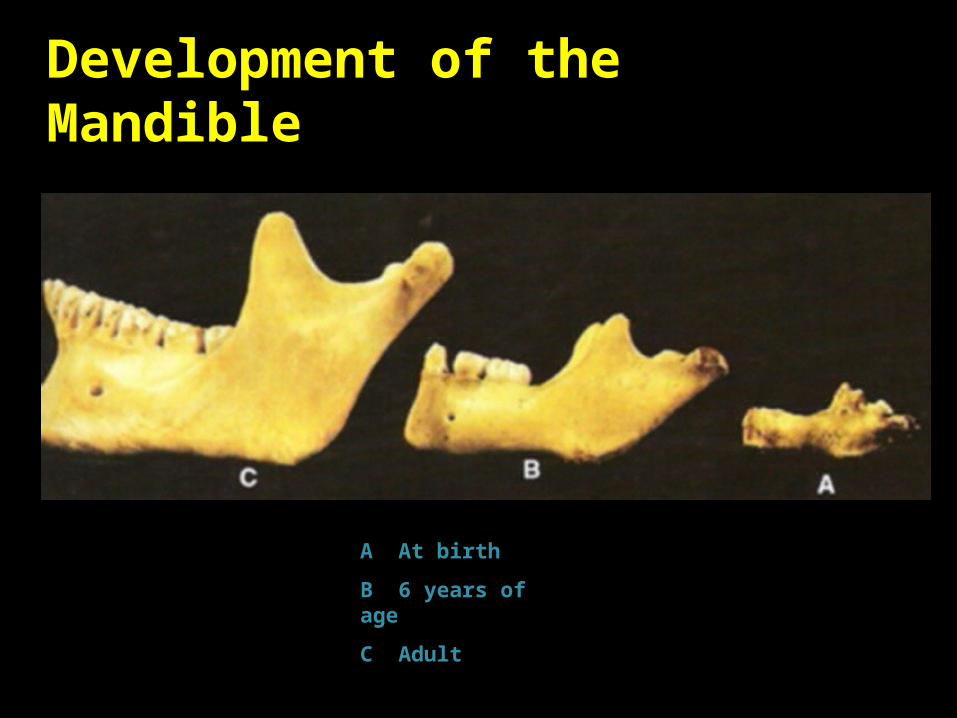
Development of the Mandible
A At birth
B 6 years of age
C Adult

Growth of the mandible occurs by the remodeling of bone.
Increase in the height of the body occurs primarily by the formation of alveolar bone. Although some bone is also deposited along the lower border of the mandible .
Increase in length of the mandible is accomplished by bone deposition on the posterior surface of the ramus with compensatory resorption on its anterior surface, accompanied by deposition of bone on the posterior surface of the coronoid process and resorption on the anterior surface of the condyle.
Increase in the width of the mandible is produced by deposition of bone on the outer surface of the mandible and resoprion on the inner surface
Development of the Maxilla

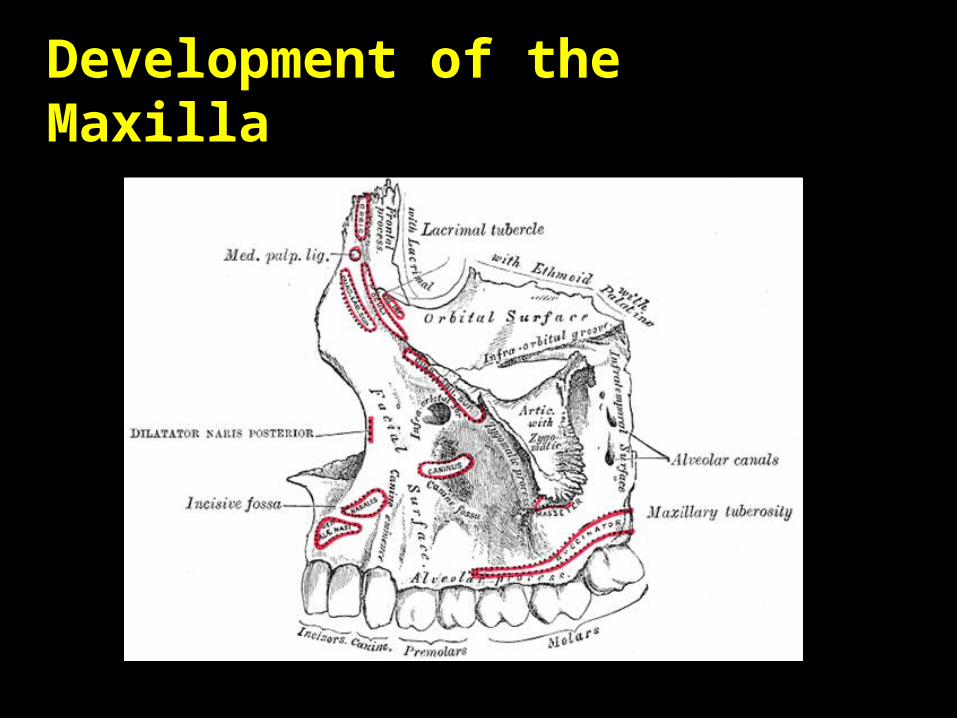
Development of the Maxilla• The maxilla develops intramembranously with the centre of ossification appearing during the 8th week of intrauterine life.
• Growth is affected by the development of the orbital, nasal and oral cavities.
• from the region of the developing deciduous canine, ossification spreads throughout the developing maxilla into its growing processes : palatine, zygomatic, frontal and alveolar.
A Developing maxilla
B Developing canine
C Palatine process
Development of the Maxilla
• The maxilla grows by bone remodelling and suture growth.
• Eyeballs, nasal septum and orbital pad of fat provide forces that separate the maxilla from adjacent bones, thus allowing sutural growth.
• An outpocketing of the middle meatus of the nose results in the appearance of the maxillary sinus (4 months in utero).

Development of the Maxilla
A Front view
B Side view
Although small at birth the maxillary sinus is identifiable radiologically.
After birth the maxillary sinus enlarges with the growing maxilla although it is only fully developed following the eruption of the permanent dentition
Forward growth of the whole face is dependent upon growth of the spheno-occipital synchondrosis

Congenital abnormalities of the jaws are most often associated with ( First branchial arch ) syndromes.
Treacher Collins’ syndrome and Pierre Robin’s sequence are the two most common types of the first arch syndrome

Treacher Collins’ Syndrome : is a rare autosomal dominant congenital disorder characterized by craniofacial deformities
The typical physical features include:
1. Downward-slanting eyes2. Micrognathia 3. Conductive hearing loss 4. underdeveloped zygoma 5. drooping part of the lateral
lower eyelids6. malformed or absent ears.

Pierre Robin’s sequence : is a congenital condition of
facial abnormalities in humans.
The 3 main features are1. Cleft palate2. Retrognathia (abnormal
positioning of the jaw or maxilla)
3. Glossoptosis (airway obstruction caused by backwards displacement of the tongue base)

Trauma and infection in the region of the TMJ may lead to an ankylosis of the condyle with the base of the skull, with the most common sigh of limited mouth opening
The lack of function of the mandible may lead to a decreased growth on the affected side with resulted facial asymmetry

Development of the Tongue
• The tongue develops from different embryological origins.
• The anterior 2 thirds is derived from 3 swellings:
• 2 lateral lingual swellings
• 1 midline tuberculum impar
• The posterior third is derived from a single midline swelling called the copula.
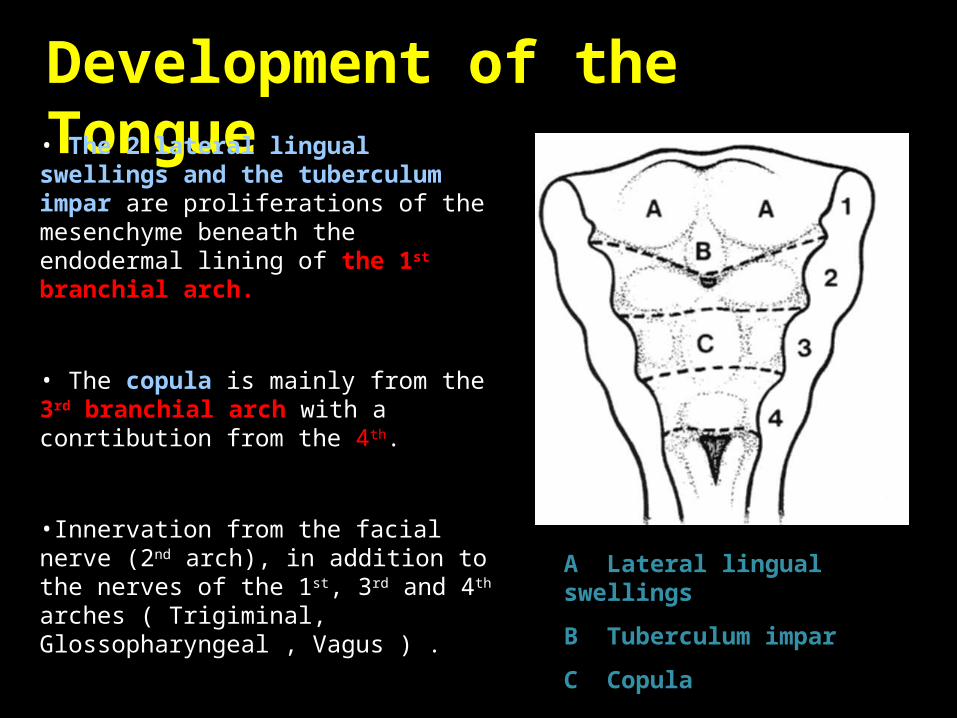
Development of the Tongue • The 2 lateral lingual swellings and the tuberculum impar are proliferations of the mesenchyme beneath the endodermal lining of the 1st branchial arch.
• The copula is mainly from the 3rd branchial arch with a conrtibution from the 4th.
•Innervation from the facial nerve (2nd arch), in addition to the nerves of the 1st, 3rd and 4th arches ( Trigiminal, Glossopharyngeal , Vagus ) .
•Tongue muscles develop from occipital somites that migrate into the tongue with their nerve supply (hypoglossal nerve).
A Lateral lingual swellings
B Tuberculum impar
C Copula

Development of the Thyroid
• The thyroid gland develops between the tuberculum impar and the copula.
•The thyroid gland is the first endocrine gland that developes
• Foramen caecum on the fully developed tongue, demarcates the site of origin of the thyroid gland