Embed Size (px)
Citation preview

PRESENTATION BY GULRUKH

Learning Disability
Definition:
"Specific learning disability" is defined as follows by IDEA:
The term "specific learning disability" means a disorder in one or more of the basic psychological processes involved in understanding or in using language, spoken or written,
which disorder may manifest itself in the imperfect ability to listen, think, speak, read, write,
spell, or do mathematical calculations.
Disorders included. Such term includes such conditions as perceptual disabilities, brain
injury, minimal brain dysfunction, dyslexia, and developmental aphasia.
Disorders not included. Such term does not include a learning problem that is primarily the
result of visual, hearing, or motor disabilities, of mental retardation, of emotional
disturbance, or of environmental, cultural, or economic disadvantage.
Components from 6 different
Definitions:
By their nature are heterogeneous disorders.
Represent specific types of under achievement (i.e. a person demonstrates appreciably less
ability in some skills than in others)
Are probably the result of some central nervous system (CNS) dys-funtion.
Involve some form of psychological process (i.e. Intrinsic) disorder
Can be manifested in academic disorders
Can be manifested in spoken language disorders.
Don’t result from other conditions such as mental retardation, behaviour disorders, and so
forth
Can be manifested in thinking disorders. (derailment, poverty of
speech, tangentially, illogicality, perseveration, neologism)

TYPES OF LEARNING DISORDERS:
Dyslexia 315.00(F81.0)
a language-based disability in
which a person has trouble
understanding written words. It may
also be referred to as reading
disability or reading disorder.
Dyscalculia315.1(FB1.2)a mathematical disability in which a person has a difficult time solving arithmetic problems and grasping math concepts.
Dysgraphia 315.2(F81.
81)
a writing disability in which a person finds it hard to form letters or write within a defined space.
TYPES OF LEARNING DISORDERS
disabilities in which a person has difficulty understanding language despite normal hearing and vision.
a neurological disorder which originates in the right hemisphere of the brain, causing problems with visual-spatial, intuitive, organizational, evaluative and holistic processing functions.

DYSLEXIA:
Dyslexia is the name for specific learning disabilities in reading.
Dyslexia is often characterized by difficulties with accurate word recognition,
decoding and spelling.
Dyslexia may cause problems with reading comprehension and slow down
vocabulary growth.
Dyslexia may result in poor reading fluency and reading out loud.
Dyslexia is neurological and often genetic.
Dyslexia is not the result of poor instruction.
With the proper support, almost all people with dyslexia can become good readers
and writers.

SIGNS & SYMPTOMS
The Dyslexia Research Trust6 includes these as the most common signs and symptoms
associated with dyslexia:
Learning to read - the child, despite having normal intelligence and receiving proper teaching
and parental support, has difficulty learning to read.
Milestones reached later - the child learns to crawl, walk, talk, throw or catch things, ride a bicycle later than the majority of other kids.
Speech - apart from being slow to learn to speak, the child commonly mispronounces words,
finds rhyming extremely challenging, and does not appear to distinguish between different
word sounds.
Slow at learning sets of data - at school the child takes much longer than the other children to
learn the letters of the alphabet and how they are pronounced. There may also be problems
remembering the days of the week, months of the year, colors, and some arithmetic tables.
SIGNS & SYMPTOMS
Coordination - the child may seem clumsier than his or her peers. Catching a ball
may be difficult.
Left and right - the child commonly gets "left" and "right" mixed up.
Reversal - numbers and letters may be reversed without realizing.
Spelling - may not follow a pattern of progression seen in other children. The child
may learn how to spell a word today, and completely forget the next day. One
word may be spelt in a variety of ways on the same page.
Phonology problems - phonology refers to the speech sounds in a language. If a
word has more than two syllables, phonology processing becomes much more
difficult. For example, with the word "unfortunately" a person with dyslexia may be
able to process the sounds "un" and "ly", but not the ones in between.

SIGNS & SYMPTOMS
Concentration span - children with dyslexia commonly find it hard to concentrate for long, compared to other children. Many adults with dyslexia say this is because after a few minutes of non-stop struggling, the child is mentally exhausted. A higher number of children with dyslexia also have ADHD (attention-deficit hyperactivity disorder), compared to the rest of the population.
Sequencing ideas - when a person with dyslexia expresses a sequence of ideas, they may seem illogical for people without the condition.
Autoimmune conditions - people with dyslexia are more likely to develop immunological problems, such as hay fever, asthma, eczema, and other allergies.
Types of Dyslexia:
The types are identified by the nature of the problem within the central nervous system /brain.
Trauma Dyslexia
Usually occurs after some form of brain trauma or injury to the area of the brain that controls reading and writing. It is a permanent brain injury rarely seen in today's school-age population because it results from severe head injuries.
Primary dyslexia
It’s a dysfunction of, rather than damage to, the left side of the brain (cerebral cortex) and does not change with age. Individuals with this type of dyslexia are rarely able to read above a fourth-grade level and may struggle with reading, spelling, and writing as adults. Primary dyslexia is passed in family lines through their genes (hereditary). It is found more often in boys than in girls.
Secondary/developmental
Type of dyslexia is felt to be caused by hormonal development or malnutrition during the early stages of fetal development. Poor parenting, abuse, neglect, and/or poor nutrition during the developmental years 0 to 5 are also known causes. Developmental dyslexia diminishes as the child matures. It is also more common in boys.
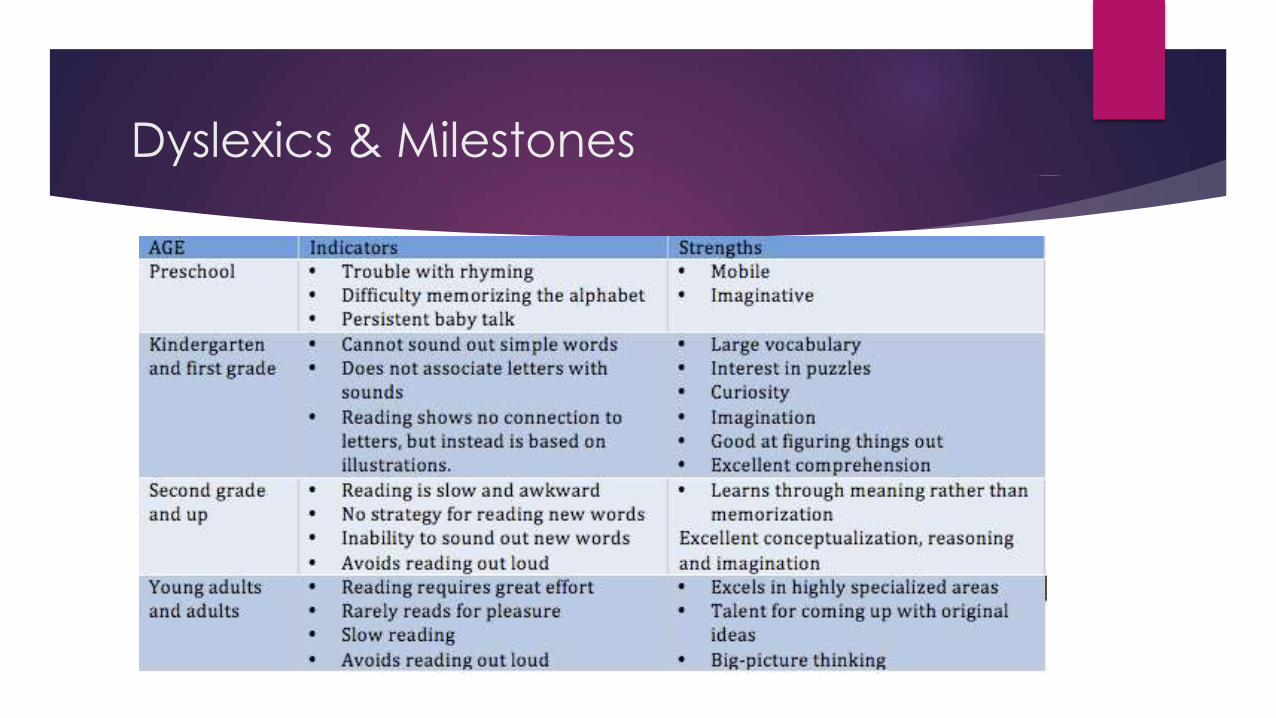
Dyslexics & Milestones


Treatment:

Integrative Approach:
Learning Disabilities Diagnostic Inventory- LDDI
Description
The learning disabilities diagnostic inventory (LDDI) is an assessment device composed of
items taken from the research and theoretical literature on specific learning disabilities
(LD) especially as it pertains to the neuropsychological aspects. The items represent
specific observable behaviours associated with LD in listening, speaking reading writing
mathematics and reasoning.
Consists of:
six independent scales, each with 15 easy-to-rate items.
Stanines are used to identify the likelihood of intrinsic processing disorders in the six
areas—Listening, Speaking, Reading, Writing, Mathematics, Reasoning
also to conduct a profile analysis to determine the extent to which a student’s LDDI profile
reflects that which is associated with learning disabilities.

Learning Disabilities Diagnostic Inventory
AGE RANGE:
Identify learning disabilities in children ages 8 to 17.
TIME PERIOD:
The LDDI can be completed in 10 minutes by a teacher or speech-language pathologist who is familiar with the student’s skills.
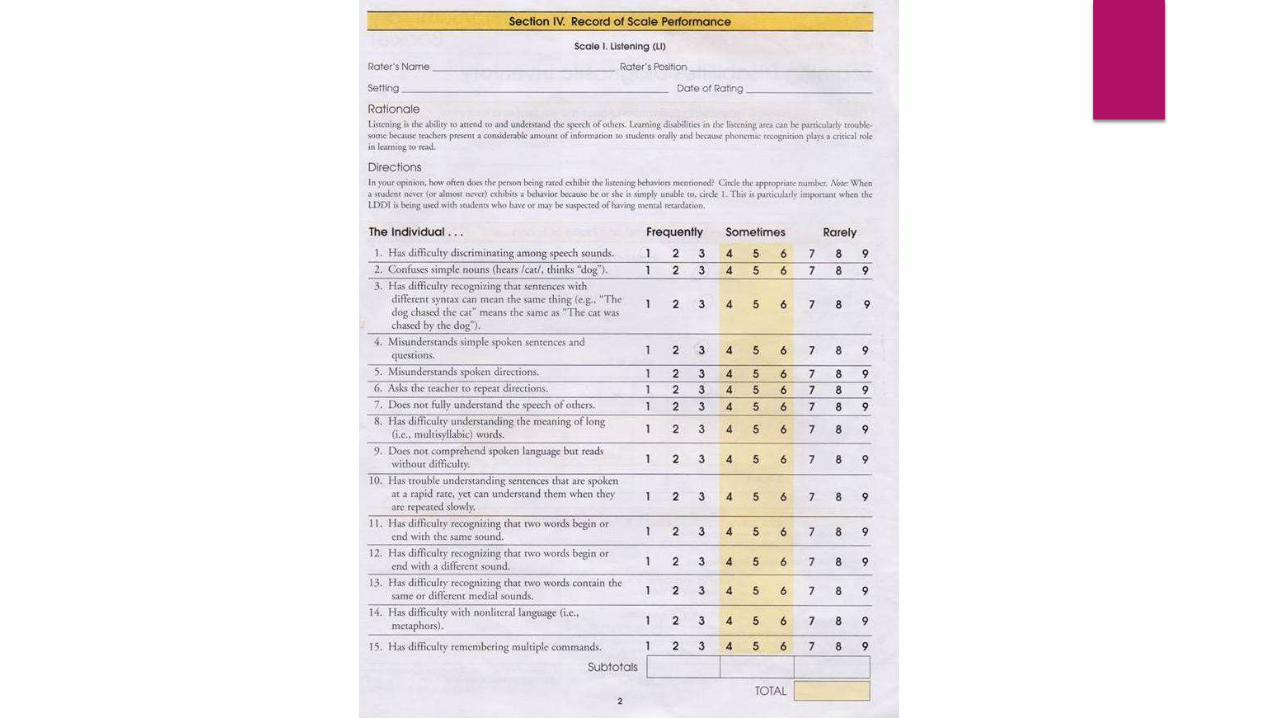
Scales & Forms
Listening
Speaking
Reading
Writing
Mathematics
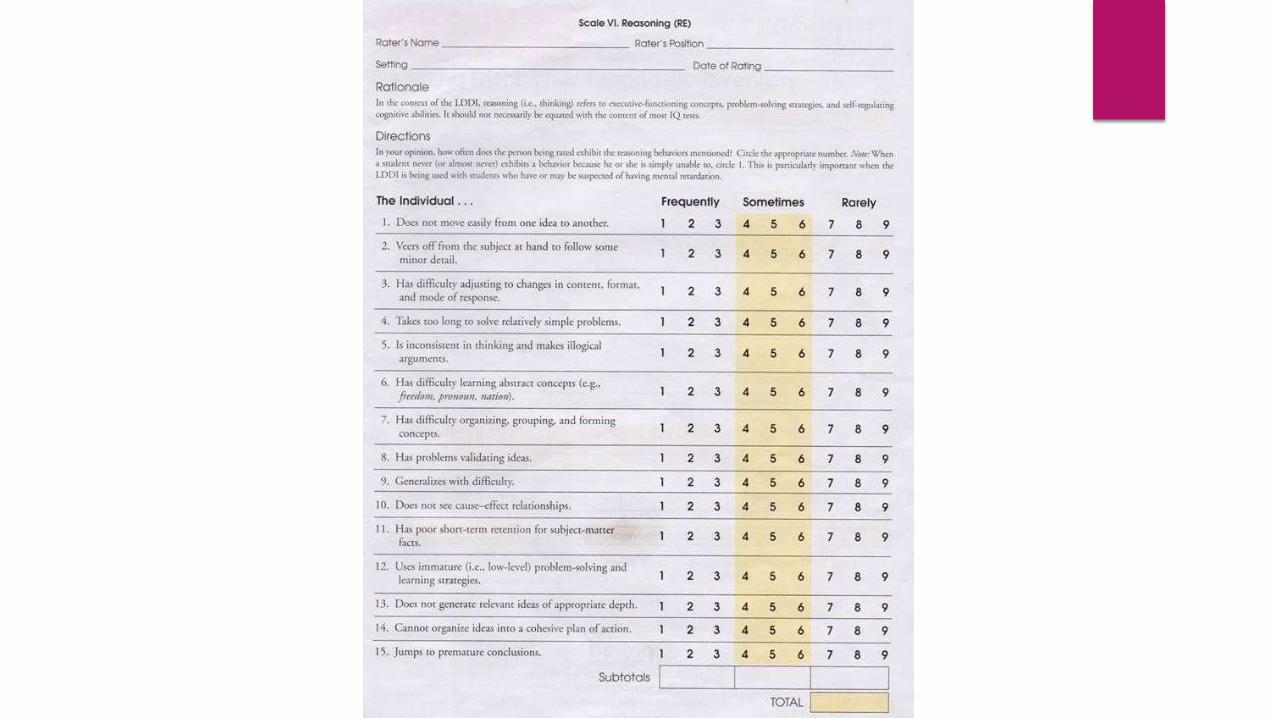
Reasoning


Worksheet:




LDDI SCORING
RAW SCORES Total number of points rated
for each scale.
Don’t tell anything in particular, just help in finding out stanines.
STANINES Stanines are converted from
raw scores using the tables in the appendix.
Standard scores with a mean of 5 and a standard deviation of 1.96) and percentiles
Identify the likelihood of intrinsic processing disorders in the six areas assessed by the lddi.
Conduct a profile analysis to determine the extent to which a student’s LDDI profile reflects which is associated with learning difficulties.
PERCENTILES Percentile ranks represent
values that indicate the percentage of the distribution of a representative sample of individuals of the same age group

Psychometrics of the Test:
Reliability
Internal consistency reliability coefficients exceed .90 for all scales. evidence for
stability and inter-scorer reliability is also provided and coefficients are in the .80s
and .90s.
Thus, the LDDI can be used with confidence to yield consistent results.
ValidityThese studies involved extensive item selection and differentiation examinations,
which included confirmatory factor analysis; as well as studies that examined the
lddi’s relationship to age, academic achievement, group differentiation, gender,
and ethnicity-all of which support the validity of the lddi scores. Factor analysis
research also validated the lddi’s factor structure. These studies all provide
evidence that the LDDI yields valid results that can be used with confidence to
identify the presence or absence of learning difficulties in children and
adolescents.
Controlling for Test Bias
The LDDI was built to minimise the effects of bias
First, the effects of bias were controlled and minimized through the inclusion of
minority groups in the normative sample.
Second, the examination of reliability and validity information was presented for
the different racial, ethnic, and gender groups.
A particularly powerful element of content-description validity is the demonstration
of excellent internal consistency reliability for the different racial, ethnic, and
gender groups.
Finally, the use of differential item functioning analysis was used to reduce item
bias during item selection. Delta score values were used to remove items that
appeared to be biased against targeted groups.

the LDDI will tell you the extent to which students’ skill patterns in a
particular area (e.g., reading, writing) are consistent with those individuals
known to have LD in that area (e.g., dyslexia, dysgraphia).

STRENGTHS AND
LIMITATIONS
INTERNAL CONSISTENCY
RELIABILITY COEFFICIENTS EXCEED
.90 FOR ALL SCALES. IN ADDITION, EVIDENCE FOR
STABILITY AND INTERSCORER
RELIABILITY IS PROVIDED, AND
COEFFICIENTS ARE IN THE .80S
AND .90S. THUS, THE
LDDI CAN BE USED WITH
CONFIDENCE TO YIELD
CONSISTENT RESULTS.

STRENGTHS
CONTROLLING FOR TEST BIAS
LDDI WAS BUILT TO MINIMIZE THE EFFECTS OF BIAS. NUMEROUS STEPS WERE TAKEN TO DETECT AND ELIMINATE SOURCES OF CULTURAL, GENDER, AND RACIAL BIAS. FIRST, THE EFFECTS OF BIAS WERE CONTROLLED AND MINIMIZED THROUGH THE INCLUSION OF MINORITY GROUPS IN THE NORMATIVE SAMPLE. SECOND, THE EXAMINATION OF RELIABILITY AND VALIDITY INFORMATION WAS PRESENTED FOR THE DIFFERENT RACIAL, ETHNIC, AND GENDER GROUPS. A PARTICULARLY POWERFUL ELEMENT OF CONTENT-DESCRIPTION VALIDITY IS THE DEMONSTRATION OF EXCELLENT INTERNAL CONSISTENCY RELIABILITY FOR THE DIFFERENT RACIAL, ETHNIC, AND GENDER GROUPS. FINALLY, THE USE OF DIFFERENTIAL ITEM FUNCTIONING ANALYSIS WAS USED TO REDUCE ITEM BIAS DURING ITEM SELECTION. DELTA SCORE VALUES WERE USED TO REMOVE ITEMS THAT APPEARED TO BE BIASED AGAINST TARGETED GROUPS
LIMITATIONS
THE LDDI IS LIMITED TO A
SINGLE LANGUAGE WHICH IS
ENGLISH, WHICH LIMITS NON-
ENGLISH SPEAKING CHILDREN TO BE ABLE TO TAKE THE TEST.
ALSO, THE TEST IS RATED BY THE
EXAMINER SO THERE IS NO
MEASUREABLE SCORE THAT
CAN BE COMPARED AGAINST
OTHER CHILDREN’S SCORES; IT
IS OPINION-BASED AND VARIES
BETWEEN EACH EXAMINER

PRECAUTIONS:
The examiner should heavily focus on the child during the assessment to
ensure a proper rating. If they are rated incorrectly, the consequences of a
poor rating could be devastating to the child’s future. The area should be
well lit and the seating comfortable for the child. Because there is a
listening section of the LDDI, the room should be quiet and easy to hear to
avoid all potential distractions and interruptions. The scale should not be
used as basis for planning individual instructional program

THANKYOU FOR
LISTENING
ANY
QUESTIONS!