Embed Size (px)
DESCRIPTION
Clinical Nutrition
Citation preview

.
Medical Nutrition Therapy for Renal
Disorders

.
Functions of the Kidney
Excretory
Acid-base balance
Endocrine
Fluid and electrolyte balance

.
Excretory Functions
Removal of excess fluid and waste products
180 L of filtrate pass through the kidneys
each day producing 1-2 L of urine
Wastes excreted from the body in urine
include urea (byproduct of protein
metabolism); excess vitamins and minerals;
metabolites of some drugs and poisons

.
Acid-Base Functions
Acid-base balance is maintained through a
buffer system, which maintains blood at pH
of 7.4
Bicarbonate Buffer.
Phosphate buffers intracellular fluid

.
Endocrine Functions
1,25-dihydroxy-vitamin D3 or calcitriol is
produced in the kidney; enhances calcium
absorption
Activation of Vitamin D and excretion of
excess phosphate maintain healthy bones
Erythropoietin: acts on the bone marrow to
increase production of red blood cells

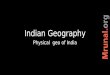
The Nephron

.
The Most Common Kidney Diseases
Diabetic Nephropathy damage to the nephrons in
the kidneys from unused sugar in the blood,
usually due to Diabetes.
High Blood Pressure can damage the small blood
vessels in the kidneys. The damaged vessels
cannot filter poison from the blood as they are
supposed to.
Polycystic Kidney Disease (PKD) is a hereditary
kidney disease in which many cysts grow in the
kidneys. These cysts may lead to kidney failure.

.
The Most Common Kidney Diseases
Acute Renal Failure - Sudden kidney failure caused by blood loss, drugs or poisons. If the kidneys are not seriously damaged, acute renal failure may be reversed.
Chronic Renal Failure - Gradual loss of kidney function is called Chronic Renal Failure or Chronic Renal Disease.
End-Stage Renal Disease - The condition of total or nearly total and permanent kidney failure.

.
Kidney Diseases
Glomerular diseases
– Nephrotic syndrome
– Nephritic syndrome—tubular or
interstitial
Tubular defects
– Acute renal failure (ARF)
Other
– End-stage renal disease (ESRD)
– Kidney stones

.
Nephrotic Syndrome
Albuminuria: more than 3 g/day urinary
albumin losses, with proportionally lesser
amounts for children
Hypoalbuminemia
Hypertension
Hyperlipidemia
Edema

.
MNT in Nephrotic Syndrome
Protein 0.8 to 1 g/kg.
Sodium based on fluid status
Potassium and other minerals (calcium,
phosphorus) monitored and
individualized
Fluid unrestricted
Diet therapy probably not effective for
hyperlipidemia; may require medication

.
Nephritic syndrome: Nutritional
Management
Diet to treat underlying disease
Restrict diet if necessary to control
symptoms
Protein restricted in uremia
Sodium restriction in hypertension
Potassium restriction in hyperkalemia

.
Acute Renal Failure
Rapid, often reversible deterioration of
renal function
GFR declines over hours to days
Most commonly occurs during
hospitalization (5% of hospitalized pts; 30%
of ICU pts)
Associated with major in-hospital morbidity
and mortality (7 to 80%)

.
Renal Replacement Therapies in ARF
Hemodialysis: standard treatment if patient
is hemodynamically stable
– However, risk of hypotension and wide swings
in body weight in unstable patients
Continuous hemofiltration provides slow,
continuous filtration across a membrane,
driven by arterial pressure.

.
Renal Replacement Therapies in ARF
Continuous hemodialysis using ultrafiltrate
fluid similar to plasma
– Clearance occurs through diffusion from high
concentration (blood) to low concentration
Peritoneal dialysis: less often used, not as
effective when large volume or solute
clearances needed.

.
MNT for Adult ARF
Energy: 1.2-1.3 or 25-35 kcal/kg
Protein: 0.8-1.2 g/kg without dialysis; 1.2-1.5 g/kg catabolic and/or initiation of dialysis
Fluid: 24 hour urine output + 500 ml (750-1500 ml)
Sodium: 2.0-3.0 grams
Potassium: 2.0-3.0 grams
Phosphorus: 8-15 mg/kg; may need binders; needs may increase with dialysis, return of kidney function, anabolism

.
Nitrogen Balance in ARF
Standard nitrogen balance studies require a
creatinine clearance of more than 50
mL/min/1.73m2
In ARF, urea nitrogen appearance (UNA) is
a better method of determining nitrogen
balance.

.
Chronic Kidney Disease

.
Causes of Chronic Kidney Disease
Cause Incidence (%)
Diabetes 40
Hypertension 27
Glomerulonephritis 13
Interstitial disease 4
Renal cystic disease 3
Tumors 2
Other 10

.
Medical Management
Dialysis
Immunosuppressant drugs
Kidney transplant
Psychological support

.
Uremia, a Clinical Syndrome—
Signs and Symptoms Malaise
Weakness
Nausea and vomiting
Muscle cramps
Itching
Metallic taste (mouth)
Neurologic impairment

.
MNT for CKD, HD, PDCKD Hemodialysis CAPD or CCPD
Protein 0.6-1.0 1.1-1.4 1.2-1.5g/kg/day
Energy 30-35 30-35 30-35
(kcal/kg IBW)
Phosphorus 8-12 indiv <17 indiv <17 indiv
(mg/kg IBW)
Sodium 1000-3000 2000-3000 2000-4000
(mg/d)
Potassium Individualized ~ 40 Individualized
(mg/kg IBW)
Fluid Unrestricted 500-750 + Individualized
(ml/d) urine output
(1000 if anuric)
Calcium Individualized Individualized Individualized
(mg/d) based on serum level ~1000 mg/day ~1000 mg/day
Use adjusted IBW if obese

.
Nutrition Assessment and
Monitoring in the CKD Pt

.
Anthropometric Measurements
% usual body weight (%UBW)
% standard body weight (%SBW)
Height
Skeletal frame size
BMI
Skinfold thickness
Mid-arm muscle area, circumference, or diameter

.
Body Weight Assessment in CKD
Use dry weight or edema-free body weight
– In HD: post-dialysis weight
– In PD: weight after drainage of dialysate with peritoneum empty
In obese or very underweight people, use adjusted edema-free body weight
Adjusted EFBW=
BWef + [SBW*-BWef x .25]

.
Blood Urea Nitrogen (BUN)
Measure of the nitrogenous waste products of protein
High BUN in CKD may reflect high protein intake, GI bleeding or inadequate dialysis, increased catabolism due to infection, surgery, poor nutrition
Decreased BUN may mean protein anabolism, overhydration, protein loss, low dietary protein

.
Creatinine (normal 0.5-1.4 mg/dL)
Nitrogenous waste product of muscle metabolism
Produced proportionate to muscle mass
Unrelated to dietary protein intake (DPI)
Sensitive marker of renal function: the higher the
serum creatinine, the greater the loss of renal
function; may reflect inadequate dialysis or
muscle catabolism
A decrease in creatinine over time may reflect loss
of lean body mass

.
Phosphorus (normal 3.5-5.5 mg/dL)
As renal function decreases, phos accumulates in
the blood
phos triggers release of PTH that releases
calcium from bone
Phos binders prevent phosphorus from being
absorbed in the gut; form insoluble compound so
phos is excreted in stool
Phos clearance poor in HD and CAPD
↓ phos may mean excess phos binder or poor p.o.

.
Calcium (8.4-9.5 mg/dL)
Most abundant mineral in human body
Nearly half of calcium is bound to albumin; if serum calcium is low, evaluate albumin level; can correct for low albumin
Calcium-Phosphorus Product: multiply serum calcium x serum phos: if >55-75, calcification can occur
<2000 mg/day elemental calcium from diet + binders stage 3-4
High Ca+: calcification, nausea, vomiting, muscle twitching may mean too much Ca+ from meds or diet

.
Serum Sodium (normall 133-145 mEq/L)
Not a reliable indicator of sodium intake in
CKD
Fluid retention due to decreased urine
production can dilute an elevated level
Serum levels must be evaluated in
conjunction with fluid status

.
Lipids
Cardiovascular disease is the most common cause of death in people with CKD
Kidney disease is considered the equivalent of a risk factor, like diabetes
HD: often have normal LDL, TC, ↑triglycerides, ↓ HDL
PD: have ↑ LDL/TC + ↑ TG
Renal Tx: ↑ LDL/TC/TG, normal HDL, often due to medications

.
Cholesterol in CKD
High • High risk TC 200-300 mg/dl (non-fasting)
• LDL goal < 100 mg/dl
Low • <150 -180, evaluate for pro-energy malnutrition
• Increased mortality

.
Hematological Indicators
Hemoglobin: ↓ due to lack of erythropoetin,
produced by the kidney; pts receive
synthetic EPO tx (Epogen)
May have anemia of chronic disease
Ferritin: may be indicator of iron overload;
↑ ferritin may mean EPO resistance

.
Glomerular Filtration Rate (GFR)
Best index of kidney function
Used to establish stage of CKD
GFR is the amount of filtrate formed per minute
based on total surface area available for filtration
(number of functioning glomeruli)
Can be determined using injected isotope (inulin)
measurement in urine
Can be calculated from serum creatinine using
standard equations

.
Interdialytic Weight Gain
Pts on dialysis gain several kg of fluid
between HD treatments
If pts gain >5%, may reflect excessive fluid
intake, leading to hypertension, edema,
ascites, pleural effusion
Fluid gains of <2% reflect minimal fluid
and food intake, may be losing body mass

.
Measures of Dialysis Adequacy
Urea Reduction Rate (URR)
Refers to change in urea concentration between
pre and post-dialysis blood tests

.
Monitoring Nutrition Status in CKD
with GFR<12mL/min/1.73m2
Recommended measure Frequency
Serum albumin levels Every 3 months
Edema-free actual body
weight, % std wt, SGA
Every 1-3 months
nPNA or dietary
interviews and diaries
Every 3-4 months

.
Pre-ESRD (DM)
Primary Prevention
– Glycemic control (DCCT)
• Aim for Euglycemia
• Watch for low B.S.
– B.P. control
• 130/80
• Na+ restrict
– Base on comorbidities (~2-3 g.)
– Medications may increase or decrease K+; monitor
• Wt. loss (gradual)/exercise

.
MNT in Patients on Hemodialysis

.
Hemodialysis
Removes concentrated molecules and
excess fluid from pts blood through
diffusion and ultrafiltration
Three parts of the system are the dialyzer
(artificial kidney), the dialysis machine, and
the dialysate
Requires vascular access, usually through
an AV (arteriovenous) fistula

.
AV (arteriovenous) Fistula

.
Nutritional Management
Prevent deficiencies
Control edema and serum electrolytes
Prevent renal osteodystrophy
Provide an attractive and palatable diet

.
MNT in HD: Protein
10-12 g free amino acids lost per treatment
during dialysis
Greater amino acid losses with glucose-free
dialysate and high flux dialyzers
1.2 g protein/kg standard body weight
(SBW) with 50% high biological value
(meat, poultry, fish, eggs, soy, dairy)
Most HD patients take in less than 1 g/day

.
MNT in HD: Energy
Adults <60 years: 35 kcal/kg SBW
Adults > 60 or obese: 30-35 kcals/kg body
weight
Actual intakes of HD patients in studies are
lower than that (mean 23 kcals/kg in HEMO
study)

.
MNT in HD: Lipids
HD patients at risk for lipid disorders
Recommended fat intake<30% of calories
and saturated fat<10%; cholesterol <300
mg/day
Optimum fiber intake 20-25 g/day
These restrictions are difficult to achieve
along with other restrictions of HD diet

.
MNT in HD: sodium and fluid
≥ 1 L fluid output: 2-4 g
Na and 2 L fluid
≤ 1 L fluid output: 2 g Na
and 1-1.5 L fluid
Anuria: 2 g Na and 1 L
fluid
Restrict Na+ if ↑
interdialytic wt gain, CHF,
edema, HTN, low serum
sodium

.
MNT in HD: Potassium
Potassium needs related to urinary output
Most patients on HD can tolerate 2.5 g of K+
Stricter diet may be indicated for pts w/ insulin deficiency, metabolic acidosis, treated with beta blockers or aldosterone antagonists, hypercatabolic
Individuals: 40 mg/kg edema-free IBW or SBW

.
MNT in HD: Phosphorus
Maintain s. phos 3.5-5.5 mg/dL
Usually ok until GFR ↓ to 20-30 mL/min
Dialysis removes 500-1000 mg/treatment
Use phosphorus binders with meals: absorb
50% of dietary phosphorus
Dietary intake: 800 to 1000 mg/day or <17
mg/kg IBW or SBW
Identify high protein, low phos food sources

.
MNT in HD: Calcium
High from excess Ca++ type binders,
vitamin D analogs, Ca++ fortification
Goal 8.4-9.5 mg/dl.

.
MNT in HD: Vitamins
H2O soluble vitamins
Dialyzable – take after H.D.
B vitamins and vitamin C in renal vitamin
↑ Vit. C → ↑ oxalate → calcification of soft tissues
and stones
Individualize need for:
– Fe++ (IV most common), Vitamin D, Ca++, Zinc.

.
MNT in HD: Vitamin D
Vitamin D is activated in the kidney to
calcitriol, or vitamin D3
As D3 levels fall, calcium absorption ↓ and
phos excretion ↓
Vitamin D3 therapy helps prevent renal
bone disease but may cause hypercalcemia
Renal pts should use calcitriol supplements
under the supervision of a physician

.
Hemodialysis
Typical diet order
– 2000 calorie, 80 g protein, 2 g Na+, 3 g K+,
low phosphorus, 1500 cc fluid restriction

.
Skeletal Effects of Chronic
Renal Failure
Hyperphosphatemia
Hypocalcemia
Hyperparathyroidism
Low bone mass and density
Osteitis fibrosa cystica—hyperplastic
demineralized bone

.
Monitor Patient Status
1. BP >140/90
2. Edema
3. Weight changes
4. Urine output
5. Urine analysis:
—Albumin
—Protein

.
Monitor Patient Status (cont)
6. Kidney function
Creatinine clearance
Glomerular filtration rate (GFR)
7. Blood values
BUN 10 to 20 mg/dl (<100 mg/dl)
Creatinine 0.7 to 1.5 mg/dl (10-15 mg/dl)
Potassium 3.5 to 5.5 mEq/L
Phosphorus 3.0 to 4.5 mg/dl
Albumin 3.5-5.5 g/dl
Calcium 9-11 mg/dl

.
Peritoneal Dialysis

.
CAPD (continuous ambulatory
peritoneal dialysis)
Most patients do 4-5 exchanges per day
A specific volume of dialysate (1500-3000 ml) is infused into the peritoneal cavity via a catheter
The dialysate dwells for 4 hours as excess fluid and toxins diffuse through peritoneal membrane
Dialysate and wastes are drained from the body and the process repeated.
Dialysate is present in the body 24 hours per day
APD (automated peritoneal dialysis therapy) speeds the process

.
MNT for PD: Energy
Energy: 35 kcals/kg/day SBW or adjusted
body weight for pts<60 years; 30 kcals/kg
for those >60
Calories provided in the dialysate should be
included in total intake (may absorb as
much as 1/3 of daily energy needs)

.
MNT for PD: Protein
PD patients lose 5-15 grams of protein a
day, primarily as albumin
Goal 1.2-1.3 g/kg SBW or ABW/day

.
MNT for PD: Sodium
PD clears sodium very well, so sodium can
be fairly liberal
However, high salt diets increase thirst and
may make adherence to fluid limits more
difficult
General recommendation is 2-4 grams
sodium

.
MNT for PD
Potassium: is easily cleared by PD; some
patients may need K+ supplementation
Calcium: limit to 2000 mg elemental
calcium
– Generally pts get ~1500 mg from calcium-
based phosphate binders
– Serum calcium should be maintained in low
normal range (8.4-9.5 mg/dl)

.
MNT for PD
Phosphorus: limited to 800-1000 mg/day
which is difficult with high protein diet
– Use phosphate binders
Fluid: can be adjusted by varying the
dextrose concentrations of the dialysate
– May need to be restricted if pts cannot achieve
fluid balance without frequent hypertonic
exchanges

.
PD: weight gain,
hypertriglyceridemia, hyperglycemia
Increase exercise as allowed by MD
Limit sodium and fluid to minimize
hypertonic exchanges
Use solutions with alternate hypertonic
agents such as Icodextrin
Modify energy intake to facilitate wt loss
Modify intake of sugars and fats, especially
saturated fats

.
PD: Protein Losses, Malnutrition
Patient education regarding protein goals and ways to meet them
Suggest pt eat protein foods first and limit fluids at mealtime
Frequent smaller portions of protein and easy to eat proteins such as egg white, cottage cheese, etc
Education on sterile technique to avoid peritonitis

.
Food Groups Kcal CHO g. PRO g. FAT g. Na mg. K+ mg. PO4 mg.
Milk ( ½ c.) 85 6 4 5 80 185 110
Meat 65 0 7 4 25 100 65
Starch 80 15 2 1 80 35 35
Vegetable 25 5 1 0 15 150 20
Fruit 60 15 0.5 0 5 150 15
Fat (1TB.) 100 0 0 11 150 0 5
Calorie
Boosters
60 15 0 0 15 20 5
Beverages:
Coffee (1c.)
tea (1 bag)
0 0 0 0 0 100 0
RENAL EXCHANGES FOR MEAL PLANNING

.
Protein Foods (65 kcals, 7 grams protein, 25 mg Na, 100 mg K+, 65 mg
phos)
Meat 1 ounce
Egg 1
Fish 1 ounce
Shellfish 1 ounce
Poultry 1 ounce
Egg substitutes ¼ c
Bacon 4 slices
Cheese 1 oz
Milk 1 cup
Nut butters 2 T
Cottage cheese ¼ cup
Lunchmeat 1 oz

.
Milk Servings (2% milk) 85 kcals, 6 g CHO, 4 g pro, 5 g fat, 80 mg Na+, 185 mg K+, 110 mg Phos
½ cup milk
½ cup plain ice cream
½ cup yogurt

.
Starch Servings80 kcal, 15 g CHO, 2 g pro, 1 g fat, 80 mg Na+, 35 mg K+, 35 mg PO4
Bread, white or rye 1 slice
Cake 2 in sq or cupcake
Plain cake donut 1
Cold cereal 1 cup
Dinner roll 1 small
Macaroni, noodles, rice ½ cup
Popcorn, unsalted, 1 cup

.
Vegetable Servings25 kcal, 5 g CHO, 1 g pro, 15 g Na+, 150 mg K+, 20 mg PO4
Asparagus ½ cup
Green beans ½ cup
Cabbage ½ cup
Carrots ½ cup
Cauliflower ½ cup
Corn ½ cup

.
Fruit Servings ↓ K+60 kcals, 15 g CHO, .5 g protein, 150 mg K+, 15 mg phos
Apple
Apple juice ½ c
Applesauce ½ c
Apricot nectar ½ c
Blackberries ½ c
Blueberries ½ c
Fruit cocktail ½ c
Grapes ½ c
Lemon
Lime
Peach
Pear
Pineapple
Plums (1)
Raspberries
Watermelon

.
Fruit Servings (High potassium)60 kcals, 15 g CHO, .5 g protein, >250 mg K+, 15 mg phos
Apricots
Bananas
Dates
Honeydew melon
Kiwifruit
Nectarine
Orange
Orange Juice
Prune juice
Prunes
Raisins

.
Fat Choice100 kcals, 11 g fat, 150 mg Na+, 5 mg PO4
Margarine/butter 1 T
Cream cheese 2 T
Mayonnaise 11/2 T
Non-dairy topping ½ cup
Sour cream ¼ cup
Vegetable oil 1 T
Tartar sauce 2 T

.
Calorie Boosters60 kcals, 15 g CHO, 15 mg Na+, 20 mg K+, 5 mg PO4
Hard candy 4 pieces
Jam or jelly 2 T
Jelly beans 15
Honey 2 T
Sugar brown or white 2 T
Marshmallows 5 large
Fruit snacks and candies 1 oz

.
Beverages100 mg K+ (also counts as fluid)
Coffee 1 cup
Tea 1 bag
Others16 oz

.
Well Mr. Osborne, it may not be kidney stones after all.

.
Kidney Stones1. Particulate matter crystallizes
Ca salts (Ca oxalate or Ca phosphate)
Uric acid
Cystine
Struvite (NH4, magnesium and phosphate)
2. Ca salts in stones—Rx: high fluid; evaluate calcium from diet; may need more!
3. Treat metabolic problem; low-oxalate diet may be needed; acid-ash diet is sometimes useful but not proven totally effective

.
Acid-Ash Diet
Increases acidity of urine (contains chloride,
phosphorus, and sulfur)
Meats, cheese, grains emphasized
Fruits and vegetables limited (exceptions
are corn, lentils, cranberries, plums, prunes)

.
Alkaline-Ash Diet
Increases alkalinity of urine (contains
sodium, potassium, calcium, and
magnesium)
Fruits and vegetables emphasized
(exceptions are corn, lentils, cranberries,
plums, prunes)
Meats and grains limited

.
Summary
Renal diseases—delicate balance of
nutrients
Regular monitoring of lab values, with
altered dietary interventions accordingly