Embed Size (px)
Citation preview

KEY TERMS
antihistamines
antitussives
decongestants
expectorants
mucolytics
rebound congestion
rhinitis medicamentosa
ANTITUSSIVES
benzonatate
codeine
dextromethorphan
hydrocodone
DECONGESTANTS
Topical Nasal Decongestants
ephedrine
oxymetazoline
phenylephrine
tetrahydrozoline
xylometazoline
Oral Decongestants
pseudoephedrine
Topical Nasal SteroidDecongestants
beclomethasone
budesonide
dexamethasone
flunisolide
fluticasone
triamcinolone
ANTIHISTAMINES
azelastine
brompheniramine
buclizine
cetirizine
chlorpheniramine
clemastine
cyclizine
cyproheptadine
desloratadine
dexchlorpheniramine
dimenhydrinate
diphenhydramine
fexofenadine
hydroxyzine
loratadine
meclizine
phenindamine
promethazine
EXPECTORANT
guaifenesin
MUCOLYTICS
acetylcysteine
dornase alfa
Drugs Acting on the Upper
Respiratory Tract
C H A P T E R 54
822

Drugs that affect the respiratory system work to keepthe airways open and gases moving efficiently. The
classes discussed in this chapter mainly act on the upperrespiratory tract and include the following:
• Antitussives, which block the cough reflex• Decongestants, which decrease the blood flow to
the upper respiratory tract and decrease the over-production of secretions
• Antihistamines, which block the release or actionof histamine, a chemical released during inflamma-tion that increases secretions and narrows airways
• Expectorants, which increase productive cough toclear the airways
• Mucolytics, which increase or liquefy respiratorysecretions to aid the clearing of the airways
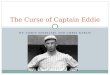
Figure 54.1 displays the sites of action of these drugs.Box 54.1 discusses the use of these agents in various agegroups.
ANTITUSSIVES
Antitussives are drugs that suppress the cough reflex. Manydisorders of the respiratory tract, including the commoncold, sinusitis, pharyngitis, and pneumonia, are accompa-nied by an uncomfortable, unproductive cough. Persistentcoughing can be exhausting and can cause muscle strainand further irritation of the respiratory tract. A cough that
occurs without the presence of any active disease processor persists after treatment may be a symptom of anotherdisease process and should be investigated before any med-ication is given to alleviate it.
Therapeutic Actions and Indications
The traditional antitussives (Table 54.1), includingcodeine (generic only), hydrocodone (Hycodan), and dex-tromethorphan (Benylin and many others), act directly onthe medullary cough center of the brain to depress thecough reflex. Because they are centrally acting, they arenot the drugs of choice for anyone who has a head in-jury or who could be impaired by central nervous system(CNS) depression. These drugs are rapidly absorbed, me-tabolized in the liver, and excreted in the urine. They crossthe placenta and enter breast milk and should not be usedduring pregnancy or lactation because of the potential forCNS depressive effects on the fetus or neonate.
Other antitussives have a direct effect on the respira-tory tract. Benzonatate (Tessalon) acts as a local anes-thetic on the respiratory passages, lungs, and pleurae,blocking the effectiveness of the stretch receptors thatstimulate a cough reflex. This drug is metabolized in theliver and excreted in the urine. It should be avoided inpregnancy and lactation because of the potential for ad-verse effects on the fetus or baby. All of these drugs areindicated for the treatment of nonproductive cough.
CHAPTER 54 — Drugs Acting on the Upper Respiratory Tract 823
Medullarycough center
Topical nasaldecongestants,oral decongestants,nasal steroids work here
Mucolyticswork here
Antihistamines work here
Inhaled steroidswork here
Lung surfactantswork here
AlveoliBronchodilatorswork here
Terpin hydrate,benzotate,guaifenesinwork here
Mucus
Codeine,hydrocodone,dextromethorphanwork here
FIGURE 54.1 Sites of action of drugsacting on the upper respiratory tract.

Contraindications and Cautions
Antitussives are contraindicated in patients who need tocough to maintain the airways (e.g., postoperative patientsand those who have undergone abdominal or thoracicsurgery). Careful use is recommended for patients with
asthma and emphysema because cough suppression in thesepatients could lead to an accumulation of secretions and a lossof respiratory reserve. Caution should also be used in pa-tients who are hypersensitive to or have a history of addiction to narcotics (codeine, hydrocodone). Codeine isa narcotic and has addiction potential. Patients who need todrive or to be alert should use codeine, hydrocodone,and dextromethorphan with extreme caution because thesedrugs can cause sedation and drowsiness.
Adverse Effects
Traditional antitussives have a drying effect on the mu-cous membranes and can increase the viscosity of respi-ratory tract secretions. Because they affect centers in thebrain, these antitussives are associated with CNS adverseeffects, including drowsiness and sedation. Their dryingeffect can lead to nausea, constipation, and complaints ofdry mouth. The locally acting antitussives are associatedwith gastrointestinal (GI) upset, headache, feelings ofcongestion, and sometimes dizziness.
824 PART X — Drugs Acting on the Respiratory System
BOX 54.1
Drug Therapy Across the Lifespan:Upper Respiratory Tract Agents
CHILDREN
These drugs are used frequently with children. Most ofthese agents have established pediatric guidelines. Caremust be taken when these drugs are used with children be-cause the risk of adverse effects—including sedation, con-fusion, and dizziness—are more common with children.
Because many of these agents are available in over-the-counter (OTC) cold, flu, and allergy remedies, it is veryimportant to educate parents about reading labels andfollowing dosing guidelines to avoid potentially serious ac-cidental overdose. Parents should always be asked specifi-cally whether they are giving the child an OTC or herbalremedy.
Parents should also be encouraged to implement non-drug measures to help the child cope with the upper res-piratory problem—drink plenty of fluids, use a humidifier,avoid smoke-filled areas, avoid contact with known aller-gens or irritants, and wash hands frequently during thecold and flu season.
ADULTS
Adults may inadvertently overdose on these agents whentaking multiple OTC preparations to help them get throughthe misery of a cold or flu. They need to be questioned spe-cifically about the use of OTC or herbal remedies before anyof these drugs are advised or administered. Adults can alsobe encouraged to use nondrug measures to help them copewith the signs and symptoms.
The safety for the use of these drugs during pregnancyand lactation has not been established. There is a potentialfor adverse effects on the fetus related to blood flowchanges and direct drug effects when the drugs cross theplacenta. The drugs may enter breast milk and also mayalter fluid balance and milk production. It is advised thatcaution be used if one of these drugs is prescribed duringlactation.
OLDER ADULTS
Older adults frequently are prescribed one of these drugs.Older adults are more likely to develop adverse effects as-sociated with the use of these drugs, including sedation,confusion, and dizziness. Safety measures may be neededif these effects occur and interfere with the patient’s mobility and balance.
Older adults are also more likely to have renal and/or he-patic impairment related to underlying medical conditions,which could interfere with the metabolism and excretion ofthese drugs. The dosage for older adults should be startedat a lower level than recommended for younger adults. Thepatient should be monitored very closely, and dosage ad-justment should be based on the patient’s response.
These patients also need to be alerted to the potentialfor toxic effects when using OTC preparations and shouldbe advised to check with their health care provider beforebeginning any OTC drug regimen.
Focus on the Prototype:Dextromethorphan
Indications: Control of nonproductive coughActions: Depresses the cough center in the medulla
to control cough spasmsPharmacokinetics:
Route Onset Peak DurationOral 25–30 min 2 hr 3–6 hr
T1/2: 2–4 hr; metabolized in the liver and excretedin urine
Adverse effects: Dizziness, respiratory depression,dry mouth
NURSING CONSIDERATIONS FOR PATIENTS RECEIVINGANTITUSSIVES
Assessment: History and Examination
Screen for the following conditions, which could be cautionsor contraindications to use of the drug: any history of allergyto any component of the drug or drug vehicle; cough thatpersists longer than 1 week or is accompanied by othersigns and symptoms; and pregnancy or lactation.
Physical assessment should be done to establish baselinedata for assessing the effectiveness of the drug and the occur-rence of any adverse effects associated with drug therapy.Assess the following: temperature, to evaluate for possibleunderlying infection; respirations and adventitious sounds,to assess drug effectiveness and to monitor for accumulation ofsecretions; and orientation and affect, to monitor for CNSeffects of the drug.

Nursing Diagnoses
The patient receiving an antitussive may have the fol-lowing nursing diagnoses related to drug therapy:• Ineffective Airway Clearance related to excessive
drug effects• Disturbed Sensory Perception related to CNS effects• Deficient Knowledge regarding drug therapy
Implementation With Rationale
• Ensure that the drug is not taken any longer than rec-ommended to prevent serious adverse effects and increasedrespiratory tract problems.
• Arrange for further medical evaluation for coughsthat persist or are accompanied by high fever, rash,or excessive secretions to detect the underlying cause ofthe cough and to arrange for appropriate treatment of theunderlying problem.
• Provide other measures to help relieve cough (e.g., hu-midity, cool temperatures, fluids, use of topical loz-enges) as appropriate.
• Provide thorough patient teaching, including the drugname and prescribed dosage, measures to help avoidadverse effects, warning signs that may indicate prob-lems, and the need for periodic monitoring and eval-uation, to enhance patient knowledge about drug therapyand to promote compliance.
• Offer support and encouragement to help the patientcope with the disease and the drug regimen.
Evaluation
• Monitor patient response to the drug (control ofnonproductive cough).
• Monitor for adverse effects (respiratory depression,dizziness, sedation).
• Evaluate the effectiveness of the teaching plan (patientcan name drug, dosage, adverse effects to watch for,
specific measures to avoid adverse effects, measures totake to increase the effectiveness of the drug).
• Monitor effectiveness of other measures to relievecough.
DECONGESTANTS
Decongestants are drugs, usually adrenergics or sympatho-mimetics, that cause local vasoconstriction and thereforedecrease the blood flow to the irritated and dilated capil-laries of the mucous membranes lining the nasal passagesand sinus cavities. This vasoconstriction leads to a shrink-ing of swollen membranes and tends to open clogged nasalpassages, providing relief from the discomfort of a blockednose and promoting drainage of secretions and improvedair flow. An adverse effect that accompanies frequent orprolonged use of these drugs is a rebound congestion, of-ficially called rhinitis medicamentosa. The reflex reac-tion to vasoconstriction is a rebound vasodilation, whichoften leads to prolonged overuse of decongestants.
Topical steroids are also used as decongestants. Topicalsteroids act to directly block the effects of inflammation onthe nasal mucous membranes. This blocks the swelling,congestion, and increased secretions that accompany in-flammation. The end result is an opening of the nasal pas-sages and an increase in air flow. These drugs take severalweeks to be really effective and are more often used incases of chronic rhinitis.
Topical Nasal Decongestants
The topical nasal decongestants include ephedrine(Kondon’s Nasal ), oxymetazoline (Afrin, Allerest, andothers), phenylephrine (Coricidin and many others),tetrahydrozoline (Tyzine), and xylometazoline (Otrivin)(Table 54.2). Many of these are available as over-the-counter (OTC) preparations. The choice of a topicalnasal decongestant is individual. Some patients may haveno response to one and respond very well to another.
CHAPTER 54 — Drugs Acting on the Upper Respiratory Tract 825
Table 54.1 Drugs in Focus
Antitussives
Drug Name Usual Dosage Usual Indications
benzonatate(Tessalon)
codeine(generic)
dextromethorphan(Benylin and others)
hydrocodone(Hycodan )
Adult and pediatric (>10 y): 100–200 mg PO t.i.d.
Adult: 10–20 mg PO q4–6hPediatric (6–12 y): 5–10 mg PO q4–6hPediatric (2–6 y): 2.5–5 mg PO q4–6hAdult: 10–30 mg PO q4–8h; 60 mg PO b.i.d. for
sustained action Pediatric (6–12 y): 5–10 mg PO q4h; 30 mg PO
b.i.d. for sustained action Pediatric (2–6 y): 2.5–7.5 mg PO q4–8h; 15 mg PO
b.i.d. for sustained action Adult: 5–10 mg PO q4–6hPediatric (2–12 y): 1.25–5 mg PO q4–6h
All of the antitussives are indicated fortreatment of nonproductive cough

Therapeutic Actions and Indications
Topical decongestants are sympathomimetics, meaningthat they imitate the effects of the sympathetic nervoussystem to cause vasoconstriction, leading to decreasededema and inflammation of the nasal membranes. Becausethese drugs are applied topically, the onset of action is al-most immediate and there is less chance of systemic ef-fects. They are available as nasal sprays that are used torelieve the discomfort of nasal congestion that accom-panies the common cold, sinusitis, and allergic rhinitis.These drugs can also be used when dilation of the nares isdesired to facilitate medical examination or to relieve thepain and congestion of otitis media. Opening the nasalpassage allows better drainage of the eustachian tube,relieving pressure in the middle ear.
Pharmacokinetics
Although they are not generally absorbed systemically,any portion of these topical decongestants that is absorbedis metabolized in the liver and excreted in urine. There areno studies regarding the effects of these topical drugsin pregnancy or lactation. As with any drug used duringpregnancy or lactation, caution should be used.
Contraindications and Cautions
Caution should be used when there is any lesion or ero-sion in the mucous membranes that could lead to systemic ab-sorption. Caution should also be used in patients with anycondition that might be exacerbated by sympathetic ac-tivity, such as glaucoma, hypertension, diabetes, thyroid
disease, coronary disease, or prostate problems, becausethese agents have adrenergic properties.
Adverse Effects
Adverse effects associated with topical decongestants in-clude local stinging and burning, which may occur thefirst few times the drug is used. If the sensation does notpass, the drug should be discontinued, because it may in-dicate lesions or erosion of the mucous membranes. Usefor longer than 3 to 5 days can lead to a rebound conges-tion. (Rebound congestion occurs when the nasal pas-sages become congested as the drug effect wears off. Asa result, patients tend to use more drug to decrease thecongestion, thus initiating a vicious cycle of congestion–drug–congestion, which leads to abuse of the decon-gestant.) Sympathomimetic effects (e.g., increased pulse,blood pressure; urinary retention) should be monitoredbecause some systemic absorption may occur, althoughthese effects are less likely with topical administrationthan with other routes.
Clinically Important Drug–Drug Interactions
The use of topical nasal decongestants is contraindicatedwith concurrent use of cyclopropane or halothane anes-thesia because serious cardiovascular effects could occur.Combined use with any other sympathomimetic drug orsympathetic-blocking drug could result in toxic or non-effective responses. Monitor the use of these combina-tions carefully.
826 PART X — Drugs Acting on the Respiratory System
Table 54.2 Drugs in Focus
Topical Nasal Decongestants
Drug Name Usual Dosage Usual Indications
ephedrine(Kondon’s Nasal)
oxymetazoline(Afrin, Allerest)
phenylephrine(Coricidin)
tetrahydrozoline(Tyzine)
xylometazoline(Otrivin)
Instill solution in each nostril q4h, do not use forchildren <6 y unless advised by physician
Adult and pediatric (>6 y): two to three sprays ordrops in each nostril b.i.d.
Pediatric (2–5 y): two to three drops of 0.05%solution in each nostril b.i.d.
Adult and pediatric (>6 y): one to two sprays ineach nostril q3–4h
Adult and pediatric (>6 y): two to four drops ineach nostril t.i.d.–q.i.d.
Pediatric (2–6 y): two to three drops of 0.05% solution in each nostril q4–6h
Adult: two to three sprays or two to three dropsin each nostril q8–10h
Pediatric (2–12 y): two to three drops of 0.05%solution q8–12h
Relief of the discomfort of nasal congestion asso-ciated with the common cold, sinusitis, allergicrhinitis; relief of pressure of otitis media
Relief of the discomfort of nasal congestion asso-ciated with the common cold, sinusitis, allergicrhinitis
Relief of the discomfort of nasal congestion asso-ciated with the common cold, sinusitis, allergicrhinitis
Relief of the discomfort of nasal congestion asso-ciated with the common cold, sinusitis, allergicrhinitis; relief of pressure of otitis media
Relief of the discomfort of nasal congestion asso-ciated with the common cold, sinusitis, allergicrhinitis; relief of pressure of otitis media

NURSING CONSIDERATIONS FORPATIENTS RECEIVING TOPICALNASAL DECONGESTANTS
Assessment: History and Examination
Screen for the following conditions, which could becautions or contraindications to use of the drug: any his-tory of allergy to the drug or a component of the drugvehicle; glaucoma, hypertension, diabetes, thyroiddisease, coronary disease, and prostate problems, allof which could be exacerbated by the sympathomimetic ef-fects; and pregnancy or lactation, which require cautioususe of the drug.
Physical assessment should be done to establish base-line data for assessing the effectiveness of the drug and theoccurrence of any adverse effects associated with drug ther-apy. Assess the following: skin color and temperature,to assess sympathetic response; orientation and reflexes, toevaluate CNS effects of the drug; pulse, blood pressure,and cardiac auscultation, to monitor cardiovascular andsympathomimetic effects; respirations and adventitiousbreath sounds, to assess effectiveness of drug and potentialexcess effect; bladder percussion, to monitor for urinaryretention related to sympathomimetic effects; and nasalmucous membrane evaluation, to monitor for lesions thatcould lead to systemic absorption and to evaluate deconges-tant effect.
Nursing Diagnoses
The patient receiving a topical nasal decongestant mayhave the following nursing diagnoses related to drugtherapy:• Acute Pain related to GI, CNS, or local effects of drug• Disturbed Sensory Perception (Kinesthetic) re-
lated to CNS effects (less likely with this route ofadministration)
• Deficient Knowledge regarding drug therapy
Implementation With Rationale
• Teach the patient the proper administration of thedrug to ensure therapeutic effect (Box 54.2). The pa-tient should be instructed to clear the nasal passagesbefore use, to tilt the head back when applying thedrops or spray, and to keep it tilted back for a fewseconds after administration. This technique helpsensure contact with the affected mucous membranes anddecreases the chances of letting the drops trickle down theback of throat, which may lead to more systemic effects.
• Caution patients not to use the drug for longer than5 days and to seek medical care if signs and symp-toms persist after that time to facilitate detection of un-derlying medical conditions that may require treatment.
CHAPTER 54 — Drugs Acting on the Upper Respiratory Tract 827
Focus on the Prototype:Ephedrine
Indications: Symptomatic relief of nasal and nasopharyngeal mucosal congestion due to thecommon cold, hay fever, or other respiratory allergies; adjunctive therapy of middle ear infections to decrease congestion around the eustachian ostia
Actions: Sympathomimetic effects, partly due to release of norepinephrine from nerve terminals;vasoconstriction leads to decreased edema and inflammation of the nasal membranes
Pharmacokinetics:Route Onset DurationTopical (nasal spray) Immediate 4–6 hr
T1/2: 0.4–0.7 hr; metabolized in the liver and ex-creted in urine; little is usually absorbed for sys-temic metabolism
Adverse effects: Disorientation, confusion, light-headedness, nausea, vomiting, fever, dyspnea, rebound congestion
BOX 54.2
Focus on Clinical Skills: Administering Nasal Medications
Proper administration technique is very important for as-suring that drugs given nasally have the desired thera-peutic effect. It is important to periodically check thenares for any signs of erosion or lesions, which couldallow systemic absorption of the drug. Most patients pre-fer to self-administer nasal drugs, so patient teaching isvery important. Explain the technique and then observethe patient using the technique.
NASAL SPRAYTeach the patient to sit upright and press a finger over onenares to close it. Hold the spray bottle upright and placethe tip of the bottle about 1⁄2 inch into the open nares. Firmlysqueeze the bottle to deliver the drug. Caution the patientnot to squeeze too forcefully, which could send the drugup into the sinuses, causing more problems. Repeat withthe other nares.
NASAL AEROSOLTeach the patient to place the medication cartridge intothe plastic nasal adapter and shake it well. Remove theplastic cap from the applicator and place the tip inside thenostril. Have the patient sit upright and tilt the head back.The patient should firmly press on the canister once to de-liver the drug; inhale; and hold his or her breath for a fewseconds. Then exhale. The patient should be encouragedto keep the head titled back for a few minutes and re-minded not to blow his or her nose for at least 2 minutes.

• Caution patients that these drugs are found in manyOTC preparations and that care should be taken notto inadvertently combine drugs with the same ingre-dients, leading to overdose.
• Provide safety measures if dizziness or sedation occuras a result of drug therapy to prevent patient injury.
• Institute other measures to help relieve the discomfortof congestion (e.g., humidity, increased fluid intake,cool environment, avoidance of smoke-filled areas)as appropriate.
• Provide thorough patient teaching, including the drugname and prescribed dosage, measures to help avoidadverse effects, warning signs that may indicate prob-lems, and the need for periodic monitoring and eval-uation, to enhance patient knowledge about drug therapyand to promote compliance.
• Offer support and encouragement to help the patientcope with the disease and the drug regimen.
Evaluation
• Monitor patient response to the drug (relief of nasalcongestion).
• Monitor for adverse effects (local burning and sting-ing; adrenergic effects such as increased pulse, bloodpressure, urinary retention, cool and clammy skin).
• Evaluate the effectiveness of the teaching plan (patientcan name drug, dosage, adverse effects to watch for,specific measures to avoid adverse effects, measures totake to increase the effectiveness of the drug, properadministration technique).
• Monitor the effectiveness of comfort and safety mea-sures and compliance with the regimen.
Oral Decongestants
Oral decongestants are drugs that are taken orally todecrease nasal congestion related to the common cold, sinusitis, and allergic rhinitis. They are also used to relievethe pain and congestion of otitis media. Opening of thenasal passage allows better drainage of the eustachian tube,relieving pressure in the middle ear. The only oral decon-gestant currently available for use is pseudoephedrine(Dorcol, Decofed, and others) (Table 54.3).
Therapeutic Actions and Indications
Oral decongestants shrink the nasal mucous membraneby stimulating the alpha-adrenergic receptors in the nasalmucous membranes. This shrinkage results in a decreasein membrane size, promoting drainage of the sinuses andimproving air flow. Because this drug is taken systemi-cally, adverse effects related to the sympathomimeticeffects (e.g., cardiac stimulation, feelings of anxiety) aremore likely to occur.
Pharmacokinetics
Pseudoephedrine is generally well absorbed and reachespeak levels quickly—in 20 to 45 minutes. It is widely dis-tributed in the body, metabolized in the liver, and pri-marily excreted in urine. There are no adequate studiesabout its use during pregnancy and lactation, and such useshould be reserved for situations in which the benefit tothe mother outweighs any potential risk to the fetus orneonate.
Contraindications and Cautions
Because pseudoephedrine has adrenergic properties, cau-tion should be used in patients with any condition thatmight be exacerbated by sympathetic activity, such as glaucoma,
828 PART X — Drugs Acting on the Respiratory System
Table 54.3 Drugs in Focus
Oral Decongestant
Drug Name Usual Dosage Usual Indications
pseudoephedrine(Dorcol, Decofed)
Adult: 60 mg PO q4–6hPediatric: 6–12 y—30 mg PO q4–6h; 2–5 y—15 mg PO q4–6h; 1–2 y—0.02 mL/kg PO q4–6h; 3–12 mo—
3 drops/kg PO q4–6h
Decrease nasal congestion associatedwith the common cold, allergic rhini-tis; relief of pain and congestion ofotitis media
Focus on Patient SafetyIn late 2000, the U.S. Food and Drug Admin-istration removed the oral decongestant phenyl-propanolamine (PPA) from the market. This drug,which had been the center of controversy formany years, was found to be associated with anincreased number of strokes in young womenwho took the drug. The drug had been an ingre-dient in many over-the-counter cold, allergy, andflu remedies. After a short absence, most of theseproducts reappeared on the market with the drugpseudoephedrine taking the place of PPA. Thisdrug, a sympathomimetic, is also known to causesympathetic effects, including increased bloodpressure and increased heart rate. Close follow-up of the effects of this drug will be done to mon-itor for any increased risk associated with its use.

hypertension, diabetes, thyroid disease, coronary disease,and prostate problems.
Adverse Effects
Adverse effects associated with pseudoephedrine includerebound congestion. Sympathetic effects include feelingsof anxiety, tenseness, restlessness, tremors, hypertension,arrhythmias, sweating, and pallor.
Clinically Important Drug–Drug Interactions
Many OTC products, including cold remedies, allergymedications, and flu remedies, may contain pseudo-ephedrine. Taking many of these products concurrentlycan cause serious adverse effects. Teach patients to read theOTC labels to avoid inadvertent overdose.
NURSING CONSIDERATIONS FOR PATIENTS RECEIVING AN ORAL DECONGESTANT
Assessment: History and Examination
Screen for the following conditions, which could be cautionsor contraindications to use of the drug: any history of allergyto the drug and pregnancy or lactation, which are contra-indications to drug use; hypertension or coronary arterydisease, which require cautious use; and hyperthyroidism,diabetes mellitus, or prostate enlargement, all of whichcould be exacerbated by these drugs.
Physical assessment should be done to establish base-line data for assessing the effectiveness of the drug and theoccurrence of any adverse effects associated with drug ther-apy. Assess the following: skin color and lesions, tomonitor for adverse reactions; orientation, reflexes, andaffect, to monitor CNS effects of the drug; blood pressure,pulse, and auscultation, to monitor cardiovascular stimu-lations; respiration and adventitious sounds, to monitordrug effectiveness; and urinary output, to evaluate for uri-nary retention.
Nursing Diagnoses
The patient receiving an oral decongestant may have thefollowing nursing diagnoses related to drug therapy:• Acute Pain related to GI, CNS, or skin effects of drug• Increased Cardiac Output related to sympathomimetic
actions of the drug• Disturbed Sensory Perception (Kinesthetic) related
to CNS effects• Deficient Knowledge regarding drug therapy
Implementation With Rationale
• Note that this drug is found in many OTC products,especially combination cold and allergy preparations;care should be taken to prevent inadvertent overdose orexcessive adverse effects.
• Provide safety measures as needed if CNS effectsoccur, to prevent patient injury.
• Monitor pulse, blood pressure, and cardiac responseto the drug, especially in patients who are at risk forcardiac stimulation, to detect adverse effects early andarrange to reduce dosage or discontinue the drug.
• Encourage the patient not to use this drug for longerthan 1 week and to seek medical evaluation if symp-toms persist after that time to encourage the detection ofunderlying medical conditions that could be causing thesesymptoms and to arrange for appropriate treatment.
• Provide thorough patient teaching, including the drugname and prescribed dosage, measures to help avoidadverse effects, warning signs that may indicate prob-lems, and the need for periodic monitoring and eval-uation, to enhance patient knowledge about drug therapyand to promote compliance.
• Offer support and encouragement to help the patientcope with the disease and the drug regimen.
Evaluation
• Monitor patient response to the drug (improvementin nasal congestion).
• Monitor for adverse effects (sympathomimetic reac-tions including increased pulse, blood pressure, pallor,sweating, arrhythmias, feelings of anxiety, tension, dryskin).
• Evaluate the effectiveness of the teaching plan (patientcan name drug, dosage, adverse effects to watch for,specific measures to avoid adverse effects, measures totake to increase the effectiveness of the drug).
• Monitor the effectiveness of comfort and safety mea-sures and compliance with the regimen.
Topical Nasal Steroid Decongestants
Topical nasal steroid decongestants are currently verypopular for the treatment of allergic rhinitis. They havebeen found to be effective in patients who are no longergetting a response with other decongestants. The topi-cal nasal steroid decongestants include beclomethasone(Beclovent and others), budesonide (Rhinocort), dexametha-sone (Decaderm and others), flunisolide (AeroBid andothers), fluticasone (Flovent), and triamcinolone (Kenacort)(Table 54.4).
Therapeutic Actions and Indications
The exact mechanism of action of topical steroids is notknown. Their anti-inflammatory action results from their
CHAPTER 54 — Drugs Acting on the Upper Respiratory Tract 829

ability to produce a direct local effect that blocks many ofthe complex reactions responsible for the inflammatoryresponse. Because they are applied topically, there is lessof a chance of systemic absorption and associated adverseeffects. The onset of action is not immediate, and theymay actually require up to a week to cause any changes.If no effects are seen after 3 weeks, the drug should be dis-continued. Topical nasal steroidal preparations are usedto treat seasonal allergic rhinitis for patients who are notgetting any response from other decongestant prepara-tions. They are frequently used to relieve inflammationafter the removal of nasal polyps.
Pharmacokinetics
Because these drugs are not generally absorbed systemi-cally, their pharmacokinetics are not reported. If they wereto be absorbed systemically, they would have the samepharmacokinetics as other steroids (see Chapter 36).
Contraindications and Cautions
Because nasal steroids block the inflammatory response, theiruse is contraindicated in the presence of acute infections.Increased incidence of Candida albicans infection has beenreported with their use, related to the anti-inflammatoryand anti-immune activities associated with steroids.Caution should be used in any patient who has an activeinfection, including tuberculosis, because systemic absorp-tion would interfere with the inflammatory and immuneresponses. Patients using nasal steroids should avoid ex-posure to any airborne infection, such as chickenpox ormeasles.
Adverse Effects
The most common adverse effects associated with the useof topical nasal steroids are local burning, irritation, sting-ing, dryness of the mucosa, and headache. Because heal-ing is suppressed by steroids, patients who have recentlyexperienced nasal surgery or trauma should be monitoredclosely until healing has occurred.
830 PART X — Drugs Acting on the Respiratory System
Table 54.4 Drugs in Focus
Topical Steroid Nasal Decongestants
Drug Name Usual Dosage Usual Indications
beclomethasone(Beclovent)
budesonide(Rhinocort)
dexamethasone(Decaderm)
flunisolide(AeroBid)
fluticasone(Flovent)
triamcinolone(Kenacort)
Adult: one inhalation in each nostril b.i.d.–q.i.d.Pediatric (<12 y): one inhalation in each nostril
b.i.d.–q.i.d.
Adult and pediatric (>6 y): two sprays in each nos-tril morning and evening or four sprays in eachnostril in the morning
Adult: two sprays in each nostril b.i.d.–t.i.d.Pediatric: one to two sprays in each nostril b.i.d.Adult: two sprays in each nostril b.i.d.Pediatric (6–14 y): one spray in each nostril t.i.d.
to two sprays in each nostril b.i.d.Adult: 88–440 mcg b.i.d.
Adult: two sprays in each nostril every day
All of the topical steroid nasal decongestants areindicated for treatment of seasonal allergicrhinitis in patients who are not obtaining a re-sponse with other decongestants or prepara-tions and for relief of inflammation after theremoval of nasal polyps
Focus on the Prototype:Flunisolide
Indications: Treatment of seasonal allergic rhinitis for patients who are not getting any re-sponse from other decongestant preparations;relief of inflammation after the removal of nasalpolyps.
Actions: Anti-inflammatory action, which results from the ability to produce a direct local effect that blocks many of the complex reactions responsible for the inflammatory response
Pharmacokinetics:Route Onset Peak DurationTopical (nasal Immediate 10–30 min 4–6 hr
spray)T1/2: Not generally absorbed systemicallyAdverse effects: Local burning, irritation, stinging,
dryness of the mucosa, headache, increased riskof infection

NURSING CONSIDERATIONS FORPATIENTS RECEIVING TOPICALSTEROID NASAL DECONGESTANTS
Assessment: History and Examination
Screen for the following conditions, which could be cau-tions or contraindications to use of the drug: any history ofallergy to steroid drugs or any components of the drugvehicle, which would be a contraindication, and acute in-fection, which would require cautious use.
Physical assessment should be done to establish base-line data for assessing the effectiveness of the drug and the occurrence of any adverse effects associated with drug therapy.Intranasal examination should be performed to deter-mine the presence of any lesions that would increase the riskof systemic absorption of drug. Assess the following: respi-ration and adventitious sounds, to evaluate drug effec-tiveness; and temperature, to monitor for the possibility ofacute infection.
Nursing Diagnoses
The patient receiving topical steroid nasal deconges-tants may have the following nursing diagnoses relatedto drug therapy:• Acute Pain related to local effects of the drug• Risk for Injury related to suppression of inflamma-
tory reaction• Deficient Knowledge regarding drug therapy
Implementation With Rationale
• Teach the patient how to administer these drugs prop-erly, which is very important to ensure effectiveness andprevent systemic effects. A variety of preparations areavailable (e.g., sprays, aerosols, powder disks). Advisethe patient about the proper administration techniquefor whichever preparation is recommended.
• Have the patient clear nasal passages before usingthe drug, to improve the effectiveness of the drug.
• Encourage the patient to continue using the drug reg-ularly, even if results are not seen immediately, becausebenefits may take 2 to 3 weeks to appear.
• Monitor the patient for the development of acuteinfection that would require medical intervention.Encourage the patient to avoid areas where air-borne infections could be a problem because steroiduse decreases the effectiveness of the immune and in-flammatory responses.
• Provide thorough patient teaching, including thedrug name and prescribed dosage, measures to helpavoid adverse effects, warning signs that may indicateproblems, and the need for periodic monitoring and
evaluation, to enhance patient knowledge about drugtherapy and to promote compliance.
• Offer support and encouragement to help the patientcope with the disease and the drug regimen.
Evaluation
• Monitor patient response to the drug (relief of nasalcongestion).
• Monitor for adverse effects (local burning andstinging).
• Evaluate the effectiveness of the teaching plan (patientcan name drug, dosage, adverse effects to watch for,specific measures to avoid adverse effects, measures totake to increase the effectiveness of the drug).
• Monitor the effectiveness of comfort and safety mea-sures and compliance with the regimen.
CHAPTER 54 — Drugs Acting on the Upper Respiratory Tract 831
Focus Points
• Antitussive drugs suppress the cough reflex byacting centrally, to suppress the medullarycough center, or locally, as an anesthetic or toincrease secretion and buffer irritation.
• Decongestants cause local vasoconstriction,thereby reducing blood flow to the mucousmembranes of the nasal passages and sinuscavities.
• Rebound vasodilation (rhinitis medicamentosa)is an adverse effect of excessive or long-termdecongestant use.
• Topical nasal decongestants are preferred forpatients who need to avoid systemic adrenergiceffects associated with oral decongestants.
• Topical nasal steroid decongestants block theinflammatory response and are preferred forpatients with allergic rhinitis for whom systemic steroid therapy is undesirable.
ANTIHISTAMINES
Antihistamines are found in multiple OTC preparationsthat are designed to relieve respiratory symptoms andto treat allergies. These agents block the effects of hista-mine, bringing relief to patients suffering from itchy eyes,swelling, congestion, and drippy nose.
Numerous antihistamines are available, includingfirst- and second-generation agents (Table 54.5). First-generation antihistamines have greater anticholinergiceffects, with resultant drowsiness. These drugs includeazelastine (Astelin), brompheniramine (available in com-bination products), buclizine (Bucladin-S), cetirizine(Reactine), chlorpheniramine (Aller-Chlor and others),clemastine (Tavist), cyclizine (Marezine), cyproheptadine

832 PART X — Drugs Acting on the Respiratory System
Table 54.5 Drugs in Focus
Antihistamines
Drug Name Usual Dosage Usual Indications
First-generation
azelastine(Astelin)
brompheniramine
buclizine(Bucladin-S)
cetirizine(Reactine)
chlorpheniramine(Aller-Chlor, others)
clemastine(Tavist)
cyclizine(Marezine)
cyproheptadine(Periactin)
dexchlorpheniramine(Dexchlor)
dimenhydrinate(Dimentabs, others)
diphenhydramine(Benadryl, others)
Two sprays per nostril b.i.d.
Adult and pediatric (>12 y): 6–12 mg PO q12hPediatric (6–12 y): 6 mg/d PO50–150 mg/d PO; use caution with elderly pa-
tientsAdult and pediatric (>12 y): 5–10 mg/d PO; use
5 mg with hepatic or renal impairmentPediatric (6–11 y): 5 PO or 10 mg/dPediatric (6 mo–5 y): 2.5 mg PO q12h or
5 mg/d POAdult and pediatric (>12 y): 4 mg PO q4–6h;
8–12 mg at bedtime for sustained release;use caution in elderly patients
Pediatric (6–12 y): 2 mg PO q4–6hPediatric (2–5 y): 1 mg PO q4–6h
Sustained release: 6–12 y—8 mg PO at bedtime; <6 y—not recommended
Adult and pediatric (>12 y): 1.34 mg PO b.i.d.;use caution with elderly patients
Pediatric (6–12 y): 0.67 mg PO b.i.d.Pediatric (<6 y): not recommended
Adult: 50 mg PO q4–6h; use caution withelderly patients
Pediatric (6–12 y): 25 mg PO t.i.d.Adult: 4–20 mg/d POPediatric (7–14 y): 4 mg PO b.i.d.–t.i.d.Pediatric (2–6 y): 2 mg PO b.i.d.–t.i.d.
Adult and pediatric (>12 y): 4–6 mg PO at bedtime or q8–10h during the day
Pediatric (6–11 y): 4 mg/g PO at bedtime
Adult and pediatric (>12 y): 50–100 mg PO q4–6h or 50 mg IM as neededPediatric: <2 y—1.25 mg/kg IM q.i.d.; 2–6 y
—25 mg PO q6–8h; 6–12 y—25–50 mg POq6–8h
Adult: 25–50 mg PO q4–6h or 10–50 mg IM or IV
Pediatric: 12.5–25 mg PO t.i.d.–q.i.d. or 5 mg/kgper day IM or IV
Geriatric: use caution
Relief of symptoms of seasonal and perennialallergic rhinitis
Relief of symptoms of seasonal and perennialallergic rhinitis
Relief of nausea and vomiting associated withmotion sickness
Relief of symptoms of seasonal and perennialallergic rhinitis; management of chronicurticaria
Relief of symptoms of seasonal and perennialallergic rhinitis; allergic conjunctivitis;uncomplicated urticaria and angioedema;amelioration of allergic reactions; relief ofdiscomfort associated with dermographism;and as an adjunctive therapy in anaphylacticreactions
Relief of symptoms of seasonal and perennialallergic rhinitis; allergic conjunctivitis;uncomplicated urticaria and angioedema;amelioration of allergic reactions; relief ofdiscomfort associated with dermographism;and as an adjunctive therapy in anaphylacticreactions
Relief of nausea and vomiting associated withmotion sickness
Relief of symptoms of seasonal and perennialallergic rhinitis; allergic conjunctivitis;uncomplicated urticaria and angioedema;amelioration of allergic reactions; relief ofdiscomfort associated with dermographism;and as an adjunctive therapy in anaphylacticreactions
Relief of symptoms of seasonal and perennialallergic rhinitis; allergic conjunctivitis;uncomplicated urticaria and angioedema;amelioration of allergic reactions; relief ofdiscomfort associated with dermographism;and as an adjunctive therapy in anaphylacticreactions
Relief of nausea and vomiting associated withmotion sickness
Relief of symptoms of seasonal and perennialallergic rhinitis; allergic conjunctivitis;uncomplicated urticaria and angioedema;amelioration of allergic reactions; relief ofdiscomfort associated with dermographism;and as an adjunctive therapy in anaphylacticreactions; sleeping aid; parkinsonism
(continued)

(Periactin), dexchlorpheniramine (Dexchlor), dimenhydri-nate (Dimentabs and others), diphenhydramine (Benadryland others), hydroxyzine (Vistaril and others), meclizine(Bonine), phenindamine (Nolahist), and promethazine(Phenergan and others). Second-generation antihistamines,including desloratadine (Clarinex), fexofenadine (Allegra),and loratadine (Claritin), have fewer anticholinergic effectsthan do first-generation agents.
When choosing an antihistamine, the individual pa-tient’s reaction to the drug is usually the governing factor.If a person needs to be alert, one of the second-generation,nonsedating antihistamines would be the drug of choice.Because of their OTC availability, these drugs are oftenmisused to treat colds and influenza.
Therapeutic Actions and Indications
The antihistamines selectively block the effects of histamine at the histamine-1 receptor sites, decreasingthe allergic response. They also have anticholinergic
(atropine-like) and antipruritic effects. Antihistaminesare used for the relief of symptoms associated with sea-sonal and perennial allergic rhinitis, allergic conjunc-tivitis, uncomplicated urticaria, and angioedema. Theyare also used for amelioration of allergic reactions to bloodor blood products, for relief of discomfort associated withdermographism, and as adjunctive therapy in anaphylac-tic reactions. Other uses that are being explored includerelief of exercise- and hyperventilation-induced asthmaand histamine-induced bronchoconstriction in asthmat-ics. They are most effective if used before the onset ofsymptoms.
Pharmacokinetics
The oral antihistamines are well absorbed orally, with anonset of action ranging from 1 to 3 hours. They are gen-erally metabolized in the liver, with excretion in fecesand urine. These drugs cross the placenta and enterbreast milk, so their use should be avoided in pregnancy
CHAPTER 54 — Drugs Acting on the Upper Respiratory Tract 833
Table 54.5 Drugs in Focus (Continued)
Antihistamines
Drug Name Usual Dosage Usual Indications
Relief of symptoms of seasonal and perennialallergic rhinitis; allergic conjunctivitis;uncomplicated urticaria and angioedema;amelioration of allergic reactions; relief ofdiscomfort associated with dermographism;and as an adjunctive therapy in anaphylacticreactions; sedation
Relief of nausea and vomiting associated withmotion sickness
Temporary relief of allergic rhinitis; hay fever
Relief of symptoms of seasonal and perennialallergic rhinitis; allergic conjunctivitis;uncomplicated urticaria and angioedema;amelioration of allergic reactions; relief ofdiscomfort associated with dermographism;and as an adjunctive therapy in anaphylacticreactions; sedation
Relief of symptoms of seasonal allergic rhinitis;chronic idiopathic urticaria
Relief of symptoms of seasonal and perennialallergic rhinitis
Relief of symptoms of seasonal and perennialallergic rhinitis; allergic conjunctivitis;uncomplicated urticaria and angioedema;amelioration of allergic reactions; relief ofdiscomfort associated with dermographism;and as an adjunctive therapy in anaphylacticreactions
hydroxyzine(Vistaril, others)
meclizine(Bonine)
phenindamine(Nolohist)
promethazine(Phenergan)
Second-generation (nonsedating)
desloratadine(Clarinex)
fexofenadine(Allegra)
loratadine(Claritin)
Adult: 25–100 mg PO t.i.d.–q.i.d. or 25–100 mgIM q4–6h
Pediatric (>6 y): 50–100 mg/day PO in divideddoses
Pediatric (<6 y): 50 mg/d PO in divided dosesor 1.1 mg/kg per dose IM
Adult and pediatric (>12 y): 25–100 mg/dPO; use caution with elderly patients
Adult and pediatric (>12 y): 25 mg PO q4–6hPediatric (<12 y): 12.5 mg PO q 4–6hAdult: 25 mg PO, PR, IM, or IVPediatric: 6.25–25 mg PO or PR
Adult and pediatric (>12 y): 5 mg/d POHepatic or renal impairment: 5 mg PO every
other dayAdult and pediatric (>12 y): 60 mg PO b.i.d.Geriatric or renal-impaired patient: 60 mg PO
every day Pediatric (6–11 y): 30 mg PO b.i.d.Adult and pediatric (>12 y): 10 mg/d POGeriatric or hepatic-impaired patient: 10 mg PO
every other dayPediatric (6–11 y): 10 mg PO every dayPediatric (2–5 y): 5 mg/d PO

and lactation unless the benefit to the mother outweighsthe potential risk to the fetus or baby.
Contraindications and Cautions
Antihistamines are contraindicated during pregnancy orlactation. They should be used with caution in renal orhepatic impairment, which could alter the metabolism andexcretion of the drug. Special care should be taken whenthese drugs are used by any patient with a history of ar-rhythmias or prolonged Q-T intervals because fatal car-diac arrhythmias have been associated with the use of certainantihistamines and drugs that increase Q-T intervals, includ-ing erythromycin.
Adverse Effects
The adverse effects most often seen with antihistamineuse are drowsiness and sedation (Case Study and FocusedFollow-up 54-1), although second-generation antihista-mines are less sedating in many people. The anticholin-ergic effects that can be anticipated include drying of therespiratory and GI mucous membranes, GI upset andnausea, arrhythmias, dysuria, urinary hesitancy, and skineruption and itching associated with dryness.
Drug–Drug Interactions
Drug–drug interactions vary among the antihistamines;for example, anticholinergic effects may be prolongedif diphenhydramine is taken with a monoamine inhibitorand the interaction of fexofenadine with ketoconazoleor erythromycin may raise fexofenadine concentra-tions to toxic levels. For more information, consult anursing drug handbook or package insert for individ-ual details.
NURSING CONSIDERATIONS FOR PATIENTS RECEIVINGANTIHISTAMINES
Assessment: History and Examination
Screen for the following conditions, which could be cautionsor contraindications to use of the drug: any history of allergyto antihistamines; pregnancy or lactation; and prolongedQ-T interval, which are contraindications to the use of thedrug; and renal or hepatic impairment, which requires cau-tious use of the drug.
Physical assessment should be done to establish base-line data for assessing the effectiveness of the drug and the occurrence of any adverse effects associated with drug therapy.Assess the following: skin color, texture, and lesions,to monitor for anticholinergic effects or allergy; orientation,affect, and reflexes, to monitor for changes due to CNS effects;respirations and adventitious sounds, to monitor drugeffects; and serum liver and renal function tests, to mon-itor for factors that could affect the metabolism or excretionof the drug.
Nursing Diagnoses
The patient receiving antihistamines may have the fol-lowing nursing diagnoses related to drug therapy:• Acute Pain related to GI, CNS, or skin effects of the
drug• Disturbed Sensory Perception (Kinesthetic) related
to CNS effects• Deficient Knowledge regarding drug therapy
Implementation With Rationale
• Administer the drug on an empty stomach, 1 hourbefore or 2 hours after meals, to increase the absorptionof the drug; the drug may be given with meals if GIupset is a problem.
• Note that a patient may have poor response to one ofthese agents but a very effective response to another;the prescriber may need to try several different agentsto find the one that is most effective.
• Because of the drying nature of antihistamines, pa-tients often experience dry mouth, which may leadto nausea and anorexia; suggest sugarless candies orlozenges to relieve some of this discomfort.
834 PART X — Drugs Acting on the Respiratory System
Focus on the Prototype:Diphenhydramine
Indications: Symptomatic relief of perennial andseasonal rhinitis, vasomotor rhinitis, allergic conjunctivitis, urticaria, and angioedema; also used for treating motion sickness and parkinsonism, and as a nighttime sleep aid and to suppress coughs
Actions: Competitively blocks the effects of histamineat H1-receptor sites; has atropine-like antipruriticand sedative effects
Pharmacokinetics:Route Onset Peak DurationOral 15–30 min 1–4 hr 4–7 hrIM 20–30 min 1–4 hr 4–8 hrIV Rapid 30–60 min 4–8 hr
T1/2: 2.5–7 hr; metabolized in the liver and excretedin urine
Adverse effects: Drowsiness, sedation, dizziness, epigastric distress, thickening of bronchial secretions, urinary frequency, rash, bradycardia

CHAPTER 54 — Drugs Acting on the Upper Respiratory Tract 835
If K.E. is self-medicating for the signs and symptoms ofseasonal rhinitis, what could be causing his drowsi-ness and dizziness?
What teaching points should be emphasized with thispatient and his wife?
What is the best approach for this patient?What crucial patient history questions should you ask
before proceeding any further?If you do not know this patient, given his presenting
story, what medical conditions would need to beruled out before proceeding further?
Case Study and Focused Follow-up to 54-1
Dangers of Self-medicating for Seasonal Rhinitis
CRITICAL THINKING
gestants, or other upper respiratory tract agents. Thenurse should encourage K.E.—and all patients—to checkthe labels of any OTC medications being taken and tocheck with the health care provider if there are any ques-tions. K.E. and his wife should receive written informationabout the drugs that K.E. is taking. They also should beshown how to read OTC bottles or boxes for informationon the contents of various preparations. In addition, theyshould be encouraged to use alternative methods to re-lieve the discomfort of seasonal rhinitis (e.g., using a hu-midifier, drinking lots of liquids, avoiding smoky areas)to allay the belief that many OTC drugs are needed. Finally,K.E. and his wife should be advised to check with theirhealth care provider if they have any questions about anOTC or prescription drugs, or if they have continuedproblems coping with seasonal allergic reactions. Otherprescription medication may prove more effective.
The first impression of K.E.’s condition is that it is a neu-rological disorder. K.E. should be evaluated by a healthcare provider to rule out significant neurological prob-lems. However, after a careful patient history and physi-cal examination, K.E.’s condition seemed to be related tohigh levels of over-the-counter (OTC) medications.
There are a multitude of OTC cold and allergy reme-dies, most of which contain the same ingredients in vary-ing proportions. A patient may be taking one to stop hisnasal drip, another to help his cough, another to relievehis congestion, and so on. By combining OTC medica-tions like this, a patient is at great risk for inadvertentlyoverdosing or at least allowing the medication to reachtoxic levels.
In this situation, the first thing to determine is exactlywhat medication is being taken and how often. K.E. seemsto have received toxic levels of antihistamines, decon-
DISCUSSION
IMPLEMENTATIONProvide comfort and safety measures, e. g., give drug
with meals; teach about mouth care; increase humid-ity; institute safety measures if dizziness occurs.
Provide support and reassurance to deal with drugeffects and allergy.
Provide patient teaching regarding drug name, dosage,adverse effects, precautions, and warning signs toreport.
EVALUATIONEvaluate drug effects, i. e., relief of respiratory symptoms.Monitor for adverse effects: CNS effects, thickening of
secretions, urinary retention, glaucoma.Monitor for drug–drug interactions as indicated.Evaluate effectiveness of support and encouragement
strategies, patient teaching program, and comfortand safety measures.
ASSESSMENT: HISTORY AND EXAMINATIONAssess K.E.’s health history for allergies and GI stenosis orobstruction, bladder obstruction, narrow-angle glaucoma,benign prostatic hypertrophy and concurrent use of mono-amine oxidase inhibitors and OTC allergy or cold products.
Focus the physical examination on the following areas:Neurological: orientation, reflexes, affect, coordinationSkin: lesionsCV: blood pressure, pulse, peripheral perfusionGI: bowel sounds, abdominal examHematological: CBCRespiratory: respiratory rate and character, nares,
adventitious soundsGU: urinary output
NURSING DIAGNOSESAcute Pain related to GI effects or dry mouthDecreased Cardiac OutputImpaired Sensory Perception (Kinesthetic)Impaired Urinary Elimination related to thickening mucusDeficient Knowledge regarding drug therapy
NURSING CARE GUIDE FOR K.E.: ANTIHISTAMINES
(continued)
has lost his balance several times, and is very drowsy.He isunable to drive to work or to stay awake. She wants to takehim to the emergency department of the local hospital.
K.E. isa46-year-oldbusinessmanwhohas been self-treatingfor seasonal rhinitis and a cold. His wife calls the physi-cian’s office; she is concerned that her husband is dizzy,
THE SITUATION

• Provide safety measures as appropriate, if CNS effectsoccur, to prevent patient injury.
• Increase humidity and push fluids to decrease the prob-lem of thickened secretions and dry nasal mucosa.
• Have the patient void before each dose to decreaseurinary retention if this is a problem.
• Provide skin care as needed if skin dryness and lesionsbecome a problem to prevent skin breakdown.
• Caution the patient to avoid excessive dosage and to check OTC drugs for the presence of antihista-mines, which are found in many OTC preparations andwhich could cause toxicity.
• Caution the patient to avoid alcohol while takingthese drugs because serious sedation can occur.
• Provide thorough patient teaching, including the drugname and prescribed dosage, measures to help avoidadverse effects, warning signs that may indicate prob-lems, and the need for periodic monitoring and eval-uation, to enhance patient knowledge about drug therapyand to promote compliance.
• Offer support and encouragement to help the patientcope with the disease and the drug regimen.
Evaluation
• Monitor patient response to the drug (relief of thesymptoms of allergic rhinitis).
• Monitor for adverse effects (skin dryness, GI upset, se-dation and drowsiness, urinary retention, thickenedsecretions, glaucoma).
• Evaluate the effectiveness of the teaching plan (patientcan name drug, dosage, adverse effects to watch for,specific measures to avoid adverse effects, measures totake to increase the effectiveness of the drug).
• Monitor the effectiveness of comfort and safety mea-sures and compliance with the regimen.
EXPECTORANTS
Expectorants liquefy the lower respiratory tract secretions,reducing the viscosity of these secretions and making it eas-ier for the patient to cough them up. Expectorants areavailable in many OTC preparations, making them widelyavailable to the patient without advice from a health careprovider. The only available expectorant is guaifenesin(Anti-Tuss and others) (Table 54.6).
Therapeutic Actions and Indications
Guaifenesin enhances the output of respiratory tract flu-ids by reducing the adhesiveness and surface tension ofthese fluids, allowing easier movement of the less viscoussecretions. The result of this thinning of secretions is a
836 PART X — Drugs Acting on the Respiratory System
Case Study and Focused Follow-up to 54-1 (Continued)
Dangers of Self-medicating for Seasonal Rhinitis
• Report any of the following to your health careprovider: difficulty breathing, rash, hives, difficultyin voiding, abdominal pain, visual changes, dis-orientation or confusion.
■■ Avoid the use of alcoholic beverages while you aretaking this drug. Serious drowsiness or sedation canoccur if these are combined.
■■ Avoid the use of any over-the-counter medicationwithout first checking with your health care provider.Several of these medications contain drugs that caninterfere with the effectiveness of this drug or theycan contain very similar drugs and you could experi-ence toxic effects.
■■ Tell any doctor, nurse, or other health care providerinvolved in your care that you are taking this drug.
■■ Take this drug only as prescribed. Do not give thisdrug to anyone else, and do not take similar prepara-tions that have been prescribed for someone else.Keep this drug, and all medications, out of the reachof children.
■■ Antihistamines are commonly used to treat the signsand symptoms of various allergic reactions. Becausethese drugs work throughout the body, many sys-temic effects can occur with their use (e.g., drymouth, dizziness, drowsiness).
■■ Take this drug only as prescribed. Do not increasethe dosage if symptoms are not relieved. Instead,consult your health care provider.
■■ Common effects of this drug include:• Drowsiness, dizziness: Do not drive or operate dan-
gerous machinery if this occurs. Use caution toprevent injury.
• Gastrointestinal upset, nausea, vomiting, heart-burn: Taking the drug with food may help thisproblem.
• Dry mouth: Frequent mouth care and sucking sug-arless lozenges may help.
• Thickening of the mucus, difficulty coughing, tight-ening of the chest: Use a humidifier or, if you donot have one, place pans of water throughout thehouse to increase the humidity of the room air;avoid smoke-filled areas; drink plenty of fluids.
PATIENT TEACHING FOR K.E.

more productive cough and thus decreased frequency ofcoughing. Expectorants are used for the symptomatic re-lief of respiratory conditions characterized by a dry,nonproductive cough, including the common cold, acutebronchitis, and influenza.
Pharmacokinetics
Guaifenesin is very old, and its pharmacokinetics havenot been reported.
Adverse Effects
The most common adverse effects associated with expec-torants are GI symptoms (e.g., nausea, vomiting, anorexia).Some patients experience headache, dizziness, or both; oc-casionally, a mild rash develops. The most important con-sideration in the use of these drugs is discovering the causeof the underlying cough. Prolonged use of the OTCpreparations could result in the masking of importantsymptoms of a serious underlying disorder. These drugsshould not be used for more than 1 week; if the cough per-sists, encourage the patient to seek health care.
NURSING CONSIDERATIONS FOR PATIENTS RECEIVINGEXPECTORANTS
Assessment: History and Examination
Screen for the following conditions, which could be cau-tions or contraindications to use of the drug: any history ofallergy to the drug; persistent cough due to smoking,asthma, or emphysema, which would be cautions to the useof the drug; and very productive cough, which would in-dicate an underlying problem that should be evaluated.
Physical assessment should be done to establish base-line data for assessing the effectiveness of the drug and the oc-currence of any adverse effects associated with drug therapy.Assess the following: skin, for presence of lesions and color(to monitor for any adverse reaction); temperature (to mon-itor for an underlying infection); respirations and adven-titious sounds (to evaluate the respiratory response to thedrug effects); and orientation and affect (to monitor CNSeffects of the drug).
Nursing Diagnoses
The patient receiving an expectorant may have the fol-lowing nursing diagnoses related to drug therapy:• Acute Pain related to GI, CNS, or skin effects of the
drug• Disturbed Sensory Perception (Kinesthetic) related
to CNS effects• Deficient Knowledge regarding drug therapy
Implementation With Rationale
• Caution the patient not to use these drugs for longerthan 1 week and to seek medical attention if the coughstill persists after that time to evaluate for any underlyingmedical condition and to arrange for appropriate treatment.
• Advise the use of small, frequent meals to alleviatesome of the GI discomfort associated with these drugs.
• Advise the patient to avoid driving or performingdangerous tasks if dizziness and drowsiness occur toprevent patient injury.
CHAPTER 54 — Drugs Acting on the Upper Respiratory Tract 837
Table 54.6 Drugs in Focus
Expectorant
Drug Name Usual Dosage Usual Indications
guaifenesin(Anti-Tuss, others)
Adult and pediatric (>12 y): 100–400 mg PO q4hPediatric (6–12 y): 100–200 mg PO q4hPediatric (2–6 y): 50–100 mg PO q4h
Symptomatic relief of dry, nonproduc-tive cough
Focus on the Prototype:Guaifenesin
Indications: Symptomatic relief of respiratory conditions characterized by dry, nonproductivecough and in the presence of mucus in the respiratory tract
Actions: Enhances the output of respiratory tractfluid by reducing the adhesiveness and surfacetension of the fluid, facilitating the removal ofviscous mucus
Pharmacokinetics:Route Onset Peak DurationOral 30 min Unknown 4–6 hr
T1/2: Unknown; metabolism and excretion are alsounknown
Adverse effects: Nausea, vomiting, headache, dizziness, rash

• Alert the patient that these drugs may be found inOTC preparations and that care should be taken toavoid excessive dosage.
• Provide thorough patient teaching, including the drugname and prescribed dosage, measures to help avoidadverse effects, warning signs that may indicate prob-lems, and the need for periodic monitoring and eval-uation, to enhance patient knowledge about drug therapyand to promote compliance.
• Offer support and encouragement to help the patientcope with the disease and the drug regimen.
Evaluation
• Monitor patient response to the drug (improvedeffectiveness of cough).
• Monitor for adverse effects (skin rash, GI upset,CNS effects).
• Evaluate the effectiveness of the teaching plan (patientcan name drug, dosage, adverse effects to watch for,specific measures to avoid adverse effects, measures totake to increase the effectiveness of the drug).
• Monitor the effectiveness of comfort and safety mea-sures and compliance with the regimen.
MUCOLYTICS
Mucolytics work to break down mucus in order to aid thehigh-risk respiratory patient in coughing up thick, tena-cious secretions. The medication may be administeredby nebulization or by direct instillation into the tracheavia an endotracheal tube or tracheostomy. The mucolyt-ics include acetylcysteine (Mucomyst and others) anddornase alfa (Pulmozyme) (Table 54.7).
Therapeutic Actions and Indications
Mucolytics are usually reserved for patients who havedifficulty mobilizing and coughing up secretions, such asindividuals with chronic obstructive pulmonary disease
(COPD), cystic fibrosis, pneumonia, or tuberculosis.These drugs are also indicated for patients who developatelectasis because of thick mucus secretions. They canbe used during diagnostic bronchoscopy to clear the air-way and to facilitate the removal of secretions, as well aspostoperatively and in patients with tracheostomies tofacilitate airway clearance and suctioning.
Acetylcysteine is used orally to protect liver cells frombeing damaged during episodes of acetaminophen tox-icity because it normalizes hepatic glutathione levelsand binds with a reactive hepatotoxic metabolite of acet-aminophen. Acetylcysteine affects the mucoproteinsin the respiratory secretions by splitting apart disulfidebonds that are responsible for holding the mucus ma-terial together. The result is a decrease in the tenacityand viscosity of the secretions. Acetylcysteine is metab-olized in the liver and excreted somewhat in urine. It isnot known whether it crosses the placenta or entersbreast milk.
Dornase alfa is a mucolytic prepared by recombinantDNA techniques that selectively break down respiratorytract mucus by separating extracellular DNA from pro-teins. It has a long duration of action, and its fate in thebody is not known. There are no data on its effects inpregnancy or lactation. This drug is used to relieve thebuildup of secretions in cystic fibrosis, to help keep theairways open and functioning longer.
Contraindications and Cautions
Caution should be used in cases of acute bronchospasm,peptic ulcer, and esophageal varices because the increasedsecretions could aggravate the problem.
Adverse Effects
Adverse effects most commonly associated with mucolyticdrugs include GI upset, stomatitis, rhinorrhea, bron-chospasm, and occasionally a rash.
838 PART X — Drugs Acting on the Respiratory System
Table 54.7 Drugs in Focus
Mucolytics
Drug Name Usual Dosage Usual Indications
acetylcysteine(Mucomyst)
dornase alfa(Pulmozyme)
By nebulization, 2–20 mL of 10% solution q2–6h;by direct instillation, 1–2 mL of 10–20% solu-tion q1–4h; 140 mg/kg PO loading dose, then17 doses of 70 mg/kg PO q4h as an antidote
2.5 mg inhaled through nebulizer, may increaseto 2.5 mg b.i.d. if needed
Liquefaction of secretions in patientswho have difficulty moving secre-tions; clearing of secretions for diag-nostic tests; postoperatively tofacilitate clearing of secretions;orally to protect liver from acet-aminophen toxicity
To relieve the buildup of secretions incystic fibrosis to keep airways openlonger

NURSING CONSIDERATIONS FORPATIENTS RECEIVING MUCOLYTICS
Assessment: History and Examination
Screen for the following conditions, which could be cau-tions or contraindications to use of the drug: any history ofallergy to the drug and the presence of acute bron-chospasm, which are contraindications to the use of thesedrugs; and peptic ulcer and esophageal varices, whichwould require careful monitoring and cautious use.
Physical assessment should be done to establishbaseline data for assessing the effectiveness of the drug and the occurrence of any adverse effects associated with drugtherapy. Assess the following: skin color and lesions,to monitor for adverse reactions; blood pressure andpulse, to evaluate cardiac response to drug treatment; andrespirations and adventitious sounds, to monitor drugeffectiveness.
Nursing Diagnoses
The patient receiving a mucolytic may have the fol-lowing nursing diagnoses related to drug therapy:• Acute Pain related to GI, CNS, or skin effects of the
drug• Disturbed Sensory Perception (Kinesthetic) related
to CNS effects• Ineffective Airway Clearance related to bronchospasm• Deficient Knowledge regarding drug therapy
Implementation With Rationale
• Avoid combining with other drugs in the nebulizerto avoid the formation of precipitates and potential loss ofeffectiveness of either drug.
• Dilute the concentrate with sterile water for injec-tion if buildup becomes a problem that could impede drugdelivery.
• Note that patients receiving acetylcysteine by facemask should have the residue wiped off the facemask and off their face with plain water to preventskin breakdown.
• Review the use of the nebulizer with patients re-ceiving dornase alfa at home to ensure the most effec-tive use of the drug. Patients should be cautioned tostore the drug in the refrigerator, protected fromlight.
• Caution cystic fibrosis patients receiving dornase alfaabout the need to continue all therapies for their cys-tic fibrosis because dornase alfa is only a palliative therapythat improves respiratory symptoms, and other therapiesare still needed.
• Provide thorough patient teaching, including the drugname and prescribed dosage, measures to help avoidadverse effects, warning signs that may indicate prob-lems, and the need for periodic monitoring and eval-uation, to enhance patient knowledge about drug therapyand to promote compliance.
• Offer support and encouragement, to help the patientcope with the disease and the drug regimen.
Evaluation
• Monitor patient response to the drug (improvementof respiratory symptoms, loosening of secretions).
• Monitor for adverse effects (CNS effects, skin rash,bronchospasm, GI upset).
• Evaluate the effectiveness of the teaching plan (patientcan name drug, dosage, adverse effects to watch for,specific measures to avoid adverse effects, measures totake to increase the effectiveness of the drug).
• Monitor the effectiveness of comfort and safety mea-sures and compliance with the regimen.
WEB LINKS
Health care providers and patients may want to consultthe following Internet sources:
http://www.rhinitisinfo.com Information on allergicrhinitis and seasonal rhinitis, including supportgroups, research, and treatment.
http://www.healthy.net Information on educationprograms, research, and other information related toallergies and seasonal rhinitis.
CHAPTER 54 — Drugs Acting on the Upper Respiratory Tract 839
Focus on the Prototype:Acetylcysteine
Indications: Mucolytic adjunctive therapy for abnor-mal, viscid, or inspissated mucous secretions inacute and chronic bronchopulmonary disorders;to lessen hepatic injury in cases of acetaminophentoxicity
Actions: Splits links in the mucoproteins containedin the respiratory mucus secretions, decreasingthe viscosity of the secretions; protects liver cellsfrom acetaminophen effects
Pharmacokinetics:Route Onset Peak DurationInstillation 1 min 5–10 min 2–3 hr
inhalationOral 30–60 min 1–2 hr Unknown
T1/2: 6.25 hr; metabolized in the liver and excretedin urine
Adverse effects: Nausea, stomatitis, urticaria, bronchospasm, rhinorrhea

http://www.niaid.nih.gov/research.htm Informationabout allergy research and treatment.
http://allergy.mcg.edu/media/rhinit.htmlInformation for patients, including special pediatricinformation on seasonal allergies and hay fever, resources, and references.
http://www.cff.org Information on cystic fibrosis, including research, treatments, and resources:
fluids, to use a humidifier if possible, to avoidsmoke-filled rooms, and to use good skin careand moisturizers.
• Antihistamines should be avoided with any pa-tient who has a prolonged Q-T interval becauseserious cardiac complications and even deathhave occurred.
• Expectorants are drugs that liquefy the lowerrespiratory tract secretions. They are used for the symptomatic relief of respiratory conditions characterized by a dry, non-productive cough.
• Mucolytics work to break down mucus in orderto aid high-risk respiratory patients in coughingup thick, tenacious secretions.
• Many of the drugs that act on the upper respira-tory tract are found in various OTC cough andallergy preparations. Patients need to be advisedto always read the labels carefully to avoid inadvertent overdose and toxicity.
GETTING READY FOR THE NCLEX
Answers to the questions in this chapter may be foundin “Answers to NCLEX Review Questions” on theCD-ROM in the front of the book.
Multiple Choice
1. A patient with sinus pressure and pain related toa seasonal rhinitis would benefit from takinga. an antitussive.b. an expectorant.c. a mucolytic.d. a decongestant.
2. Antitussives are useful in blocking the cough reflexand preserving the energy associated with pro-longed, nonproductive coughing. Antitussives arebest used witha. postoperative patients.b. asthma patients.c. patients with a dry, irritating cough.d. COPD patients who tire easily.
3. Patients with seasonal rhinitis experience irrita-tion and inflammation of the nasal passages andpassages of the upper airways. Treatment for thesepatients might includea. systemic corticosteroids.b. mucolytic agents.c. an expectorant.d. topical nasal steroids.
4. A patient taking an OTC cold medication and anOTC allergy medicine is found to be taking dou-ble doses of pseudoephedrine. As a result, thepatient might exhibit
840 PART X — Drugs Acting on the Respiratory System
Points to Remember
• The classes of drugs that affect the upper respi-ratory system work to keep the airways openand gases moving efficiently.
• Antitussives are drugs that suppress the coughreflex. They can act centrally, to suppress themedullary cough center, or locally, to increasesecretion and buffer irritation or to act as localanesthetics. These drugs should not be usedlonger than 1 week; patients with persistentcough after that time should seek medical evaluation.
• Decongestants are drugs that cause local vaso-constriction and therefore decrease the bloodflow to the irritated and dilated capillaries of themucous membranes lining the nasal passagesand sinus cavities.
• An adverse effect that accompanies frequent orprolonged use of decongestants is rebound vasodilation, called rhinitis medicamentosa. Thereflex reaction to vasoconstriction is a reboundvasodilation, which often leads to prolongedoveruse of decongestants.
• Topical nasal decongestants are preferable inpatients who need to avoid systemic adrenergiceffects. Oral decongestants are associated withsystemic adrenergic effects and require cautionin patients with cardiovascular disease, hyper-thyroidism, or diabetes mellitus.
• Topical nasal steroid decongestants block the inflammatory response from occurring. Thesedrugs, which take several days to weeks toreach complete effectiveness, are preferred forpatients with allergic rhinitis who need to avoidthe complications of systemic steroid therapy.
• The antihistamines selectively block the effectsof histamine at the histamine-1 receptor sites,decreasing the allergic response. Antihistaminesare used for the relief of symptoms associatedwith seasonal and perennial allergic rhinitis, al-lergic conjunctivitis, uncomplicated urticaria, orangioedema.
• Patients taking antihistamines may react to dry-ness of the skin and mucous membranes. Thenurse should encourage them to drink plenty of

a. ear pain.b. restlessness, tenseness, tremors, and palpita-
tions.c. sinus pressure.d. an irritating cough.
5. Common adverse effects associated with the useof topical nasal steroids would not includea. local burning and stinging.b. dryness of the mucosa.c. headache.d. constipation and urinary retention.
6. An antihistamine would not be the drug of choicefor treatinga. itchy eyes.b. irritating cough.c. nasal congestion.d. drippy nose.
7. Antihistamines should be used very cautiously inpatients witha. a history of arrhythmias or prolonged Q-T
intervals because fatal cardiac arrhythmiascan occur.
b. COPD.c. asthma.d. angioedema.
8. Additional nursing interventions for patients re-ceiving antihistamines probably would not includea. use of a humidifier.b. sucking sugarless lozenges to help the dry
mouth.c. limiting fluid intake to decrease swelling.d. provision of safety measures to prevent falls or
injury.9. A patient is not getting a response to the anti-
histamine that was prescribed. Appropriate actionmight includea. switching to a decongestant.b. stopping the drug and increasing fluids.c. trying a different antihistamine.d. switching to a corticosteroid.
10. Dornase alfa (Pulmozyme), because of its mecha-nism of action, is reserved for use ina. clearing secretions before diagnostic tests.b. facilitating removal of secretions postopera-
tively.
c. protecting the liver from acetaminophentoxicity.
d. relieving the buildup of secretions in cysticfibrosis.
Web Exercise
R.W. recently moved to the area and has developedseasonal rhinitis. He had asthma as a child and is con-cerned that it might be returning. He asks for up-to-date information on the two disorders and how tosurvive the discomfort. Go to the Internet and find in-formation that would be useful in preparing a teach-ing program for R.W.
Word Scramble
Unscramble the following letters to form the namesof drugs commonly used to treat upper respiratorytract problems.
1. mactelseni _________________________________
2. extramodernphhot __________________________
3. inpeerhed _________________________________
4. hatzooterylriden ____________________________
5. heednoripesuepd ___________________________
6. dobnudesie ________________________________
7. catflunisoe ________________________________
8. mazetileso _________________________________
BIBLIOGRAPHY AND REFERENCES
Bullock, B. L. (2000). Focus on pathophysiology. Philadelphia:Lippincott Williams & Wilkins.
Drug facts and comparisons. (2004). St. Louis: Facts and Comparisons.Gilman, A., Hardman, J. G., & Limbird, L. E. (Eds.). (2002).
Goodman and Gilman’s the pharmacological basis of therapeutics(10th ed.). New York: McGraw-Hill.
Karch, A. M. (2004). 2005 Lippincott’s nursing drug guide.Philadelphia: Lippincott Williams & Wilkins.
The medical letter on drugs and therapeutics. (2004). New Rochelle, NY:Medical Letter.
Professional’s guide to patient drug facts. (2004). St. Louis: Facts andComparisons.
CHAPTER 54 — Drugs Acting on the Upper Respiratory Tract 841