Embed Size (px)
Citation preview

KEY TERMS
alkalosis
edema
fluid rebound
high-ceiling diuretics
hyperaldosteronism
hypokalemia
osmotic pull
THIAZIDEDIURETICS
bendroflumethiazide
chlorothiazide
hydrochlorothiazide
hydroflumethiazide
methyclothiazide
trichlormethiazide
THIAZIDE-LIKEDIURETICS
chlorthalidone
indapamide
metolazone
quinethazone
LOOP DIURETICS
bumetanide
ethacrynic acid
furosemide
torsemide
CARBONICANHYDRASEINHIBITORS
acetazolamide
methazolamide
POTASSIUM-SPARINGDIURETICS
amiloride
spironolactone
triamterene
OSMOTIC DIURETICS
glycerin
isosorbide
mannitol
urea
Diuretic Agents
C H A P T E R 51
782

CHAPTER 51 — Diuretic Agents 783
There are five classes of diuretics, each working at aslightly different site in the nephron or using a dif-
ferent mechanism. Diuretic classes include the thiazideand thiazide-like diuretics, the loop diuretics, the carbonicanhydrase inhibitors, the potassium-sparing diuretics, andthe osmotic diuretics. For the most part, the overall nurs-ing care of a patient receiving any diuretic is similar (how-ever, see Box 51.1 for differences across the lifespan). Thediuretic classes are discussed in this chapter, starting withthe most frequently used drugs.
DIURETIC AGENTS
Diuretic agents are commonly thought of simply as drugsthat increase the amount of urine produced by the kid-neys. Most diuretics do increase the volume of urine pro-duced to some extent, but the greater clinical significanceof diuretics is their ability to increase sodium excretion.
Therapeutic Actions and Indications
Diuretics prevent the cells lining the renal tubules fromreabsorbing an excessive proportion of the sodium ions inthe glomerular filtrate. As a result, sodium and other ions
(and the water in which they are dissolved) are lost in theurine instead of being returned to the blood, where theywould cause increased intravascular volume and thereforeincreased hydrostatic pressure, which could result in leak-ing of fluids at the capillary level.
Diuretics are indicated for the treatment of edemaassociated with congestive heart failure (CHF), acutepulmonary edema, liver disease (including cirrhosis), andrenal disease and for the treatment of hypertension. Theyare also used to decrease fluid pressure in the eye(intraocular pressure), which is useful in treating glau-coma. Diuretics that decrease potassium levels mayalso be indicated in the treatment of conditions thatcause hyperkalemia.
CHF can cause edema as a result of several factors. Thefailing heart muscle does not pump sufficient blood tothe kidneys, causing activation of the renin–angiotensinsystem and resulting in increases in blood volume andsodium retention. Because the failing heart muscle cannotrespond to the usual reflex stimulation, the increased vol-ume is slowly pushed out into the capillary level as venouspressure increases because the blood is not being pumpedeffectively (see Chapter 44).
BOX 51.1
Drug Therapy Across the Lifespan: Diuretic Agents
CHILDREN
Diuretics are often used in children to treat edema associ-ated with heart defects, to control hypertension, and totreat edema associated with renal and pulmonary disorders.
Hydrochlorothiazide and chlorothiazide have estab-lished pediatric dosing guidelines. Furosemide is often usedwhen a stronger diuretic is needed; care should be takennot to exceed 6 mg/kg per day when using this drug.Ethacrynic acid may be used orally in some situations butshould not be used in infants. Bumetanide, although notrecommended for use in children, may be used for childrenwho are taking other ototoxic drugs, including antibiotics,and may cause less hypokalemia, making it preferable tofurosemide for children also taking digoxin. Spironolactoneis the only potassium-sparing diuretic that is recommendedfor use in children, but, as with adults, it should not be usedin the presence of severe renal impairment.
Because of the size and rapid metabolism of children,the effects of diuretics may be rapid and adverse effectsmay occur suddenly. The child receiving a diuretic shouldbe monitored for serum electrolyte changes; for evidence offluid volume changes; for rapid weight gain or loss, whichcould reflect fluid volume; and for signs of ototoxicity.
ADULTS
Adults may be taking diuretics for prolonged periods andneed to be aware of the signs and symptoms of fluid im-balance to report to their health care provider. Adults re-ceiving chronic diuretic therapy should weigh themselveson the same scale, in the same clothes, and at the same timeeach day to monitor for fluid retention or sudden fluid loss.They should be alerted to situations that could aggravate
fluid loss, such as diarrhea, vomiting, or excessive heat andsweating, which could change their need for the diuretic.They should also be urged to maintain their fluid intake tohelp balance their body’s compensatory mechanisms and toprevent fluid rebound.
Patients taking potassium-losing diuretics should be en-couraged to eat foods that are high in potassium and tohave their serum potassium levels checked periodically.Patients taking potassium-sparing diuretics should be cau-tioned to avoid those same foods.
The use of diuretics to change the fluid shifts associatedwith pregnancy is not appropriate. Women maintained onthese drugs for underlying medical reasons should not stoptaking the drug, but they need to be aware of the potentialfor adverse effects on the fetus. Women who are nursingand need a diuretic should find another method of feedingthe baby because of the potential for adverse effects on thebaby as well as the lactating mother.
OLDER ADULTS
Older adults often have conditions that are treated with di-uretics. They are also more likely to have renal or hepaticimpairment, which requires cautious use of these drugs.
Older adults should be started on the lowest possibledose of the drug, and the dosage should titrated slowlybased on patient response. Frequent serum electrolyte mea-surements should be done to monitor for adverse reactions.
The intake and activity level of the patient can alter theeffectiveness and need for the diuretic. High-salt diets andinactivity can aggravate conditions that lead to edema, andpatients should be encouraged to follow activity and dietaryguidelines if possible.

Pulmonary edema, or left-sided CHF, develops whenthe increased volume of fluids backs up into the lungs.The fluid pushed out into the capillaries in the lungs in-terferes with gas exchange. If this condition developsrapidly, it can be life-threatening.
Patients with liver failure and cirrhosis often presentwith edema and ascites. This is caused by (1) reducedplasma protein production, which results in less oncoticpull in the vascular system and fluid loss at the capillarylevel, and (2) obstructed blood flow through the portalsystem, which is caused by increased pressure from con-gested hepatic vessels.
Renal disease produces edema because of the loss ofplasma proteins into the urine when there is damage to theglomerular basement membrane. Other types of renal dis-ease produce edema because of activation of the renin–angiotensin system as a result of decreasing volume (asso-ciated with the loss of fluid into the urine), which causes adrop in blood pressure, or because of failure of the renaltubules to regulate electrolytes effectively.
Hypertension is predominantly an idiopathic disorder;in other words, the underlying pathology is not known.Treatment of hypertension is aimed at reducing thehigher-than-normal blood pressure, which can damageend organs and lead to serious cardiovascular disorders.Diuretics were once the key element in antihypertensivetherapy, the goal of which was to decrease volume andsodium, which would then decrease pressure in the system.Now several other classes of drugs, including angiotensin-converting enzyme (ACE) inhibitors, angiotensin recep-tor blockers (ARBs), beta-blockers, and calcium channelblockers, are used more frequently for the initial treat-ment of hypertension; however, some studies have foundthat the use of diuretics is still the most effective way oftreating initial hypertension. Diuretics are also oftenused as an adjunct to improve the effectiveness of theseother drugs.
Glaucoma is an eye disease characterized by increasedpressure in the eye—known as intraocular pressure(IOP)—which can cause optic nerve atrophy and blind-ness. Diuretics are used to provide osmotic pull to re-move some of the fluid from the eye, which decreases theIOP, or as adjunctive therapy to reduce fluid volume andpressure in the cardiovascular system, which also de-creases pressure in the eye somewhat.
Contraindications and Cautions
Diuretic use is contraindicated in the presence of allergyto any of the drugs given. Other conditions in which di-uretics are contraindicated include fluid and electrolyteimbalances, which can be potentiated by the fluid and elec-trolyte changes caused by the diuretics, and severe renal dis-ease, which may prevent the diuretic from working or couldbe pushed into a crisis stage by the blood flow changes broughtabout by the diuretic.
784 PART IX — Drugs Acting on the Renal System
Caution should be used with the following condi-tions: systemic lupus erythematosus (SLE), which fre-quently causes glomerular changes and renal dysfunction thatcould precipitate renal failure in some cases; glucose toler-ance abnormalities or diabetes mellitus, which is worsenedby the glucose-elevating effects of many diuretics; gout, whichreflects an abnormality in normal tubule reabsorption and se-cretion; liver disease, which could interfere with the normalmetabolism of the drugs, leading to an accumulation of thedrug or toxicity; and pregnancy and lactation, which areconditions that could be jeopardized by changes in fluid andelectrolyte balance.
Adverse Effects
Adverse effects associated with diuretics are specific tothe particular class used. For details, see the section onadverse effects for each class of diuretics discussed in thischapter, and refer to Table 51.1. The most common ad-verse effects seen with diuretics include gastrointestinal(GI) upset, fluid and electrolyte imbalances (Box 51.2),hypotension, and electrolyte disturbances.
Clinically Important Drug–Drug Interactions
When diuretics are used, there is a potential for inter-actions with drugs that depend on a particular electro-lyte balance for their therapeutic effects (e.g., anti-arrhythmics such as digoxin), with drugs that dependon urine alkalinity for proper excretion (e.g., quini-dine), and with drugs that depend on normal reflexesto balance their effects (e.g., antihypertensives, anti-diabetic agents), because these factors are altered by theactions of diuretics.
Other specific drug–drug interactions that might re-late to the chemical makeup of a particular diuretic arenoted in the sections for each drug.
Focus Points
• Diuretics increase sodium excretion, and there-fore water excretion, from the kidneys.
• Diuretics help relieve edema associated withCHF and pulmonary edema, liver failure and cirrhosis, and various types of renal disease.They are also used in treating hypertension.
• Diuretics must be used cautiously wheneverchanges in fluid and electrolyte balance couldexacerbate a disorder.
• Electrolyte imbalance (potassium, sodium, chloride), hypotension and hypovolemia, hypoglycemia, and metabolic alkalosis are allpotential adverse effects of diuretic therapy.

CHAPTER 51 — Diuretic Agents 785
THIAZIDE AND THIAZIDE-LIKEDIURETICS
Hydrochlorothiazide (HydroDIURIL), the most fre-quently used of the thiazide diuretics, is often used incombination with other drugs for the treatment ofhypertension. It can be used in small doses because it ismore potent than chlorothiazide (Diuril), which is theoldest drug of this class, and it is considered the pro-totype. Other thiazides include bendroflumethiazide(Naturetin), hydroflumethiazide (Diucardin), methyclo-thiazide (Aquatensen), and trichlormethiazide (Diurese)(Table 51.2).
The thiazide-like diuretics include chlorthalidone(Hygroton), indapamide (Lozol), metolazone (Mykrox), andquinethazone (Hydromox). All of these drugs are used less
often than hydrochlorothiazide and are typically chosenaccording to the prescriber’s personal preference.
Therapeutic Actions and Indications
The thiazide diuretics belong to a chemical class of drugscalled the sulfonamides. Thiazide-like diuretics have aslightly different chemical structure but work in the sameway that thiazide diuretics do. Their action is to block thechloride pump. Chloride is actively pumped out of thetubule by cells lining the ascending limb of the loop ofHenle and the distal tubule. Sodium passively moves withthe chloride to maintain an electrical neutrality. (Chlorideis a negative ion, and sodium is a positive ion.) Blocking ofthe chloride pump keeps the chloride and the sodium in
Table 51.1 Comparison of Diuretics
Diuretic Class Major Site of Action Usual Indications Major Adverse Effects
Thiazide, thiazide-like
Loop
Carbonic anhydrase inhibitors
Potassium-sparing
Osmotic
Distal convoluted tubule
Loop of Henle
Proximal tubule
Distal tubule and collecting duct
Glomerulus, tubule
Edema of CHF, liver and renal diseaseAdjunct for hypertensionAcute CHFAcute pulmonary edemaHypertensionEdema of CHF, renal and liver diseaseGlaucomaDiuresis in CHFMountain sicknessEpilepsyAdjunct for edema of CHF, liver and
renal diseaseTreatment of hypokalemiaAdjunct for hypertensionHyperaldosteronismReduction of intracranial pressurePrevention of oliguric phase of renal
failureReduction of intraocular pressureRenal clearance of toxic substances
GI upset, CNS complications,hypovolemia
Hypokalemia, volume depletion,hypotension, CNS effects, GI upset, hyperglycemia
GI upset, urinary frequency
Hyperkalemia, CNS effects, diarrhea
Hypotension, GI upset, fluid andelectrolyte imbalances
BOX 51.2
Focus on Clinical Skills: Explaining Fluid Rebound
Care must be taken when using diuretics to avoid fluid re-bound, which is associated with fluid loss. If a patient stopstaking in water and takes the diuretic, the result will be aconcentrated plasma of smaller volume. The decreased vol-ume is sensed by the nephrons, which activate the renin–angiotensin cycle. When the concentrated blood is sensedby the osmotic center in the brain, antidiuretic hormone(ADH) is released to hold water and dilute the blood. Theresult can be a “rebound” edema as fluid is retained.
Many patients who are taking a diuretic markedly de-crease their fluid intake so as to decrease the number oftrips to the bathroom. The result is a rebound of water re-tention after the diuretic effect. This effect can also be seen
in many diets that promise “immediate results”; they fre-quently contain a key provision to increase fluid intake to8 to 10 full glasses of water daily. The reflex result of di-luting the system with so much water is a drop in ADH re-lease and fluid loss.
Some people can lose 5 lb in a few days by doing this.However, the body’s reflexes soon kick in, causing reboundretention of fluid to re-establish fluid and electrolyte bal-ance. Most people get frustrated at this point and give upthe fad diet.
It is important to be able to explain this effect. Teachingpatients about balancing the desired diuretic effect withthe actions of the normal reflexes is a clinical skills.

786 PART IX — Drugs Acting on the Renal System
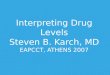
the tubule to be excreted in the urine, thus preventingthe reabsorption of both chloride and sodium in thevascular system (Figure 51.1). Because these segmentsof the tubule are impermeable to water, there is littleincrease in the volume of urine produced, but it will besodium rich, a saluretic effect. Thiazides are consideredto be mild diuretics compared with the more potent loopdiuretics.
Thiazide and thiazide-like diuretics are usually in-dicated for the treatment of edema associated with
CHF or with liver or renal disease. These drugs alsoare used as monotherapy or as adjuncts for the treat-ment of hypertension.
Pharmacokinetics
These drugs are well absorbed from the GI tract, withonset of action ranging from 1 to 3 hours. They are me-tabolized in the liver and excreted in the urine. These di-uretics cross the placenta and enter breast milk. Routine
Table 51.2 Drugs in Focus
Thiazide Diuretics
Drug Name Usual Dosage Usual Indications
Thiazide diuretics
bendroflumethiazide (Naturetin )
chlorothiazide (Diuril )
hydrochlorothiazide (HydroDIURIL )
hydroflumethiazide (Diucardin )
methyclothiazide (Aquatensen )
trichlormethiazide (Diurese )
Thiazide-like diuretics
chlorthalidone (Hygroton )
indapamide (Lozol )
metolazone (Mykrox, Zaroxolyn )
quinethazone(Hydromox )
2.5–5 mg/d PO for edema; 2.5–15 mg/d PO for hypertension
Adult: 0.5–2 g PO or IV, q.d.–b.i.d. for edema; 0.5–2 g/d PO for hypertension
Pediatric (<6 mo): up to 33 mg/kg per d POPediatric (>6 mo): 22 mg/kg per d PO in two
divided dosesAdult: 25–100 mg/d PO or intermittently, up to
200 mg/d maximum for edema; 25–100 mg/dPO for hypertension
Pediatric (<6 mo): up to 3.3 mg/kg per d PO in twodivided doses
Pediatric (6 mo–2 y): 12.5–37.5 mg/d PO in two divided doses
Pediatric (2–12 y): 37.6–100 mg/d PO in two divided doses
25–200 mg PO b.i.d. for edema; 50–100 mg/d POfor hypertension
2.5–10 mg/d PO for edema; 2.5–5 mg/d PO for hypertension
2–4 mg/d PO for edema or hypertension
50–100 mg/d PO for edema; 25–100 mg/d PO forhypertension
2.5–5 mg/d PO for edema or hypertension, basedon patient response
Mykrox: 0.5–1 mg/d PO for mild hypertensionZaroxolyn: 2.5–5 mg/d PO for hypertension;
5–20 mg/d PO for edema, based on patient response
50–200 mg/d PO based on patient response
All of the thiazide diuretics are indicated for the treatment ofedema caused by congestive heartfailure (CHF), liver disease, or renaldisease, and for adjunctive treat-ment of hypertension
All of the thiazide-like diuretics areindicated for the treatment ofedema caused by CHF or by liveror renal disease, and for adjunctivetreatment of hypertension

CHAPTER 51 — Diuretic Agents 787
use during pregnancy is not appropriate; these drugsshould be reserved for situations in which the mother haspathological reasons for use, not pregnancy manifesta-tions or complications, and only if the benefit to themother clearly outweighs the risk to the fetus. If one ofthese drugs is needed during lactation, another methodof feeding the baby should be used, because of the poten-tial for adverse effects on fluid and electrolyte changes inthe baby.
Contraindications and Cautions
Thiazide and thiazide-like diuretics are contraindicatedwith allergy to thiazides or sulfonamides, fluid or elec-trolyte imbalances, and renal and liver disease. Additionalcautions include gout, systemic lupus erythematosus, dia-betes, hyperparathyroidism, bipolar disorder, pregnancy,and lactation.
Adverse Effects
Adverse effects of thiazide use are related to interferencewith the normal regulatory mechanisms of the nephron.Potassium is lost at the distal tubule because of the ac-tions on the pumping mechanism, and hypokalemia(low blood levels of potassium) may result. Signs andsymptoms of hypokalemia include weakness, musclecramps, and arrhythmias. Another adverse effect is decreased calcium excretion, which leads to increasedcalcium levels. Uric acid excretion also is decreased, be-
cause the thiazides interfere with its secretory mecha-nism. High levels of uric acid can result in a conditioncalled gout.
If these drugs are used over a prolonged period, bloodglucose levels may increase. This may result from thechange in potassium levels (which keeps glucose out ofthe cells), or it may relate to some other mechanism ofglucose control.
Urine will be slightly alkalinized when the thiazidesare used, because they block the reabsorption of bicar-bonate. This effect can cause problems for patients whoare susceptible to bladder infections and for those takingquinidine, which requires an acid urine for excretion.
Clinically Important Drug–Drug Interactions
Decreased absorption of these drugs may occur if theyare combined with cholestyramine or colestipol. If thiscombination is used, the drugs should be taken separatedby at least 2 hours.
The risk of digoxin toxicity increases due to potentialchanges in potassium levels; serum potassium should bemonitored if this combination is used.
Decreased effectiveness of antidiabetic agents mayoccur related to the changes in glucose metabolism;dosage adjustment of those agents may be needed.
The risk of lithium toxicity may increase if thesedrugs are combined. Serum lithium levels should bemonitored and appropriate dosage adjustment made asneeded.
Spironolactone
Thiazides
AmilorideTriamterene
Loopdiuretics
Carbonicanhydraseinhibitors
FIGURE 51.1 Sites of action ofdiuretics in the nephrons.

788 PART IX — Drugs Acting on the Renal System
LOOP DIURETICS
Loop diuretics are so named because they work in theloop of Henle. Four loop diuretics are currently available(Table 51.3). Furosemide (Lasix), the most commonlyused loop diuretic, is less powerful than the new loop di-uretics, bumetanide (Bumex) and torsemide (Demadex),and therefore has a larger margin of safety for home use(see Case Study and Focused Follow-up 51-1). Ethacrynic
acid (Edecrin), the first loop diuretic introduced, is usedless frequently in the clinical setting because of the im-proved potency and reliability of the newer drugs.
Focus on the Prototype:Hydrochlorothiazide
Indications: Adjunctive therapy for edema associ-ated with CHF, cirrhosis, corticosteroid or estro-gen therapy, and renal dysfunction; treatment ofhypertension as monotherapy or in combinationwith other antihypertensives
Actions: Inhibits reabsorption of sodium and chlo-ride in distal renal tubules, increasing the excretionof sodium, chloride, and water by the kidneys
Pharmacokinetics:Route Onset Peak DurationOral 2 hr 4–6 hr 6–12 hr
T1/2: 5.6 to 14 hr; metabolized in the liver and excreted in urine
Adverse effects: Dizziness, vertigo, orthostatic hypotension, nausea, anorexia, vomiting, drymouth, diarrhea, polyuria, nocturia, musclecramps or spasms
Table 51.3 Drugs in Focus
Loop Diuretics
Drug Name Usual Dosage Usual Indications
bumetanide (Bumex )
ethacrynic acid (Edecrin )
furosemide (Lasix )
torsemide (Demadex )
0.5–2 mg/d PO as a single dose repeated to a maximum of 10 mg; 0.5–1 mg IM or IV given over 1–2 min, may berepeated in 2–3 h, do not exceed 10 mg/d
Geriatric or renal-impaired patient: 12 mg by continuous IVinfusion over 12 h may be most effective and least toxic
50–200 mg/d PO based on patient response; 0.5–1 mg/kg IVslowly
Pediatric: 25 mg PO with slow titration up as needed; do notuse with infants
20–80 mg/d PO, up to 600 mg/d may be given; 20–40 mg IMor IV given slowly; 40 mg IV over 1–2 min for acute pul-monary edema, increase to 80 mg after 1 h if response isnot adequate; 40 mg PO b.i.d. for hypertension
Geriatric or renal-impaired patient: 2–2.5 g/d POPediatric: 2 mg/kg per day PO for hypertension, do not
exceed 6 mg/kg per day; 1 mg/kg IV or IM for edema, in-crease by 1 mg/kg as needed; do not exceed 6 mg/kg
10–20 mg/d PO for IV for CHF or chronic renal failure; 5–10 mg/d PO for hypertension
All of the loop diuretics are indicatedfor the treatment of acute congestiveheart failure (CHF); acute pulmonaryedema; hypertension; and edema ofCHF, renal disease, or liver disease
Focus on Patient SafetyName confusion has been reported betweenfurosemide and torsemide; the dosage andstrength of effect of these two drugs are verydifferent. Use extreme caution to make sure youare using the prescribed drug and dosage.
Therapeutic Actions and Indications
Loop diuretics are also referred to as high-ceiling di-uretics because they cause a greater degree of diuresisthan other diuretics do. These drugs block the chloridepump in the ascending loop of Henle, where normally30% of all filtered sodium is reabsorbed. This action de-creases the reabsorption of sodium and chloride. The loopdiuretics have a similar effect in the descending loop ofHenle and in the distal convoluted tubule, resulting in theproduction of a copious amount of sodium-rich urine.These drugs work even in the presence of acid–base dis-turbances, renal failure, electrolyte imbalances, or nitro-gen retention.
Because they can produce a loss of fluid of up to 20 lb/day, loop diuretics are the drugs of choice when arapid and extensive diuresis is needed. In cases of severeedema or acute pulmonary edema, it is important to re-member that these drugs can have an effect only on the

CHAPTER 51 — Diuretic Agents 789
• What is the nature of M.R.’s reported allergy, andwhat other options could be tried?
• Think about the physiology of mitral valve diseaseand the progression of CHF in this patient. How doesfurosemide work in the body?
• What additional activities will be important to helpmaintain some balance in this patient’s cardiac status?
Case Study and Focused Follow-up to 51-1
Using Furosemide (Lasix) in Congestive Heart Failure
CRITICAL THINKING
quent rest periods. Her potassium level should be moni-tored regularly (this is especially important because sheis also taking digoxin, which is very sensitive to potas-sium levels), her edematous limbs should be elevated pe-riodically during the day, and she should monitor hersodium intake.
When M.R. was questioned about her reported allergy,it was discovered that her “allergic reaction” was actuallyincreased urination (a therapeutic effect). M.R. needs tolearn about the actions of the drug. She also needs infor-mation about the timing of administration so that the re-sultant diuresis will not interfere with rest or with herdaily activities. CHF is a progressive, incurable disease,so patient education is a very important part of the over-all management regimen.
Over time, an incompetent mitral valve leads to an en-larged and overworked left ventricle as the backup ofblood “waiting to be pumped” continues to progress. Drugtherapy for a patient with this disorder is usually aimed atdecreasing the workload of the heart as much as possibleto maintain cardiac output. Digoxin increases the contrac-tility of the heart muscle, which should lead to better per-fusion of the kidneys. Furosemide, a loop diuretic, acts onthe loop of Henle to block the reabsorption of sodium andwater and lead to a diuresis, which decreases the volumeof blood the heart needs to pump and makes the blood thatis pumped more efficient. This blood then has an oncoticpull to move fluid from the tissue into circulation, where itcan be acted on by the kidney, leading to further diuresis.
M.R. should be encouraged to maintain fluid intake andto engage in activity as much as possible, but to take fre-
DISCUSSION
IMPLEMENTATIONObtain daily weights, and monitor urine output.Provide comfort and safety measures: sugarless lozenges,
mouth care, safety precautions, skin care, nutrition.Administer drug with food, early in day.Provide support and reassurance to deal with drug
effects and lifestyle changes.Provide patient teaching regarding drug name, dosage,
side effects, precautions, warnings to report, dailyweighing, and recording dietary changes as needed.
EVALUATIONEvaluate drug effects: urinary output, weight changes,
status of edema, blood pressure changes.Monitor for adverse effects: hypotension, hypokalemia
hyperkalemia, hypocalcemia, hypercalcemia, hyper-glycemia, increased uric acid levels.
Monitor for drug–drug interactions as indicated.Evaluate effectiveness of patient teaching program and
comfort and safety measures.
ASSESSMENT: HISTORY AND EXAMINATIONAssess M.R.’s health history including allergies to diuretics,fluid or electrolyte disturbances, gout, glucose toleranceabnormalities, liver disease, systemic lupus erythematosus,pregnancy and breast-feeding.
Focus the physical examination on the following areas:Neuro: orientation, reflexes, strengthSkin: color, texture, edemaCV: blood pressure, pulse, cardiac auscultationGI: liver evaluationGU: urinary outputLaboratory tests: hematology; serum electrolytes,
glucose, uric acid; liver function tests
NURSING DIAGNOSESRisk for Deficient Fluid Volume related to diuretic effectImpaired Urinary EliminationImbalanced Nutrition: Less than Body Requirements,
related to GI upset and metabolic changesDeficient Knowledge regarding drug therapy
NURSING CARE GUIDE FOR M.R.: DIURETIC AGENTS
(continued)
10 days with the new prescription, M.R. calls to tell youthat she is allergic to the new medicine and can’t take itany more. She reports extensive ankle swelling and diffi-culty breathing. You refer her to a cardiologist for imme-diate review.
M.R. is a 68-year-old woman with rheumatic mitral valveheart disease. She has refused any surgical interventionand has developed progressively worsening congestiveheart failure (CHF). Recently furosemide (Lasix), 40 mg/d PO, was prescribed for her along with digoxin. After
THE SITUATION

BOX 51.3
Hormone-like Treatment for CongestiveHeart Failure
The U.S. Food and Drug Administration recently approvednesiritide (Natrecor ), a recombinant form of natriureticpeptide. This drug acts like natriuretic hormone, a naturalsubstance, probably produced by the hypothalamus, whichcauses a decrease in sodium reabsorption from the distalrenal tubules with a resultant dilute urine or increased vol-ume. Natriuretic hormone is normally released in responseto fluid overload or hemodilution. In studies, this drug waseffective in the treatment congestive heart failure (CHF),reducing volume and cardiac workload.
Nesiritide is given as an IV bolus of 2 mcg/kg followedby a continuous infusion of 0.01 mcg/kg per minute forup to 48 hours. It is approved for the treatment of patientswith acutely decompensated CHF who have dyspnea atrest or with minimal activity. After therapy with nesiritide,patients reported increased activity tolerance and easierbreathing at rest.
790 PART IX — Drugs Acting on the Renal System
blood that reaches the nephrons. A rapid diuresis occurs,producing a more hypertonic intravascular fluid. In pul-monary edema, this fluid then circulates back to thelungs, pulls fluid out of the interstitial spaces by its on-cotic pull, and delivers this fluid to the kidneys, where thewater is pulled out, completing the cycle. In the treat-ment of pulmonary edema, it can sometimes take hoursto move all of the fluid out of the lungs, because the fluidmust be pulled out of the interstitial spaces in the lungsbefore it can be circulated to the kidneys for removal.Remembering how the drugs work and the way in whichfluid moves in the vascular system will make it easier tounderstand the effects to anticipate.
Loop diuretics are commonly indicated for the treat-ment of acute CHF, acute pulmonary edema, edema as-sociated with CHF or with renal or liver disease, andhypertension. Box 51.3 describes nesiritide, a recombi-nant form of natriuretic peptide that was approved in 2001for the treatment of CHF and that can cause diuresis.
Pharmacokinetics
These drugs are metabolized and excreted primarilythrough urine. There are no well-controlled studies of the effects of these drugs during pregnancy. They havebeen associated with fetal and maternal deaths in animal
studies, and they should not be used during pregnancyunless the benefit to the mother far outweighs the po-tential risk. These drugs enter breast milk; if one of thesedrugs is needed during lactation, a decision should bemade about whether to discontinue nursing or to dis-
Case Study and Focused Follow-up to 51-1 (Continued)
Using Furosemide (Lasix) in Congestive Heart Failure
• Dizziness, feeling faint on arising, drowsiness: Lossof fluid can lower blood pressure and cause thesefeelings. Change positions slowly; if you feeldrowsy, avoid driving or other dangerous activi-ties. These feelings are often increased if alcohol isconsumed; avoid this combination or take specialprecautions if you combine them.
• Increased thirst: As fluid is lost, you may experi-ence a feeling of thirst. Sucking on sugarlesslozenges and frequent mouth care might help alle-viate this feeling. Do not drink an excessiveamount of fluid while taking a diuretic. Try tomaintain your usual fluid intake.
• Report any of the following to your health careprovider: muscle cramps or pain, loss or gain ofmore than 3 lb in one day, swelling in your fingersor ankles, nausea or vomiting, unusual bleeding orbruising, trembling or weakness.
■■ Avoid the use of any over-the-counter (OTC) medica-tion without first checking with your health careprovider. Several OTC medications can interfere withthe effectiveness of this drug.
■■ Tell any doctor, nurse, or other health care providerinvolved in your care that you are taking this drug.
■■ Keep this drug, and all medications, out of the reachof children.
■■ A diuretic, or “water pill,” such as furosemide (Lasix)will help to reduce the amount of fluid that is in yourbody by causing the kidneys to pass larger amountsof water and salt into your urine. By removing thisfluid, the diuretic helps to decrease the work of theheart, lower blood pressure, and get rid of edema orswelling in your tissues.
■■ This drug can be taken with food, which may elimi-nate possible stomach upset. When taking a diuretic,you should maintain your usual fluid intake and tryto avoid excessive intake of salt.
■■ Furosemide is a diuretic that causes potassium loss,so you should eat foods that are high in potassium(e.g., orange juice, raisins, bananas). If your diureticis one that causes potassium retention, you shouldavoid foods high in potassium as well as salt substi-tutes, as appropriate. You also may be asked to takea potassium substitute.
■■ Weigh yourself each day, at the same time of day andin the same clothing. Record these weights on a calen-dar. Report any loss or gain of 3 lb or more in 1 day.
■■ Common effects of this drug include the following.• Increased volume and frequency of urination: Have
ready access to bathroom facilities. Once you areused to the drug, you will know how long theeffects last for you.
PATIENT TEACHING FOR M.R.

CHAPTER 51 — Diuretic Agents 791
continue the drug. Safety for use in children youngerthan 18 years of age has not been established. If one ofthese drugs is used for a child, careful monitoring of thechild’s fluid and electrolyte balance is needed, and emer-gency support measures should be on standby.
Contraindications and Cautions
Among the contraindications to these drugs are allergyto a loop diuretic, electrolyte depletion, anuria, severerenal failure, hepatic coma, and pregnancy and lactation.Cautious use is recommended for patients with SLE,gout, or diabetes mellitus.
Adverse Effects
Adverse effects are related to the imbalance in elec-trolytes and fluid that these drugs cause. Hypokalemia isa very common adverse effect, because potassium is lostwhen the transport systems in the tubule try to save someof the sodium being lost. Alkalosis, or a drop in serumpH to an alkaline state, may occur as bicarbonate is lostin the urine. Calcium is also lost in the tubules along withthe bicarbonate, which may result in hypocalcemia andtetany. The fast loss of fluid can result in hypotensionand dizziness if it causes a rapid imbalance in fluid levels.Long-term use of these drugs may also result in hyper-glycemia because of the diuretic effect on blood glucoselevels, so susceptible patients need to be monitored forthis effect. Ototoxicity and even deafness have been re-ported with these drugs, but the loss of hearing is usuallyreversible after the drug is stopped. This may be an ef-fect of electrolyte changes on the conduction of fragilenerves in the central nervous system.
Clinically Important Drug–Drug Interactions
The risk of ototoxicity increases if loop diuretics are com-bined with aminoglycosides or cisplatin. Anticoagulationeffects may increase if these drugs are given with antico-agulants. There may also be a decreased loss of sodiumand decreased antihypertensive effects if these drugs arecombined with indomethacin, ibuprofen, salicylates, orother nonsteroidal anti-inflammatory agents; the patient
receiving this combination should be monitored closelyand appropriate dosage adjustments should be made.
Table 51.4 Drugs in Focus
Carbonic Anhydrase Inhibitors
Drug Name Usual Dosage Usual Indications
acetazolamide (Diamox )
methazolamide (Neptazane )
500 mg IV repeated in 2–4 h, then 250 mg–1 g per dayin divided doses q6–8h for glaucoma; 8–30 mg/kgper day in divided doses for epilepsy
50–100 mg PO b.i.d.–t.i.d.
Treatment of glaucoma; adjunctive treatment of epilepsy, mountain sickness
Treatment of glaucoma
Focus on the Prototype:Furosemide
Indications: Treatment of edema associated withCHF, acute pulmonary edema, hypertension
Actions: Inhibits the reabsorption of sodium andchloride from the proximal and distal renaltubules and the loop of Henle, leading to asodium-rich diuresis
Pharmacokinetics:Route Onset Peak DurationOral 60 min 60–120 min 6–8 hrIV, IM 5 min 30 min 2 hr
T1/2: 120 min; metabolized in the liver and excretedin urine
Adverse effects: Dizziness, vertigo, paresthesias,blurred vision, orthostatic hypotension, thrombo-phlebitis, photosensitivity, rash, urticaria, nausea,anorexia, vomiting, constipation, glycosuria, urinary bladder spasm, leucopenia, anemia,thrombocytopenia, muscle cramps, and spasms
CARBONIC ANHYDRASE INHIBITORS
The carbonic anhydrase inhibitors are relatively mild di-uretics. Most often, they are used to treat glaucoma, be-cause the inhibition of carbonic anhydrase results indecreased secretion of aqueous humor of the eye. Avail-able agents include acetazolamide (Diamox) and metha-zolamide (Neptazane) (Table 51.4).
Focus on Patient SafetyName confusion has occurred between acetazo-lamide and acetohexamide—an antidiabeticagent—and between Diamox (acetazolamide)and Dymelor (acetohexamide). Use caution ifeither of these drugs is prescribed for your patient; make sure that the diagnosis and thetreatment are appropriate.

792 PART IX — Drugs Acting on the Renal System
Therapeutic Actions and Indications
The enzyme carbonic anhydrase is a catalyst for the for-mation of sodium bicarbonate, which is stored as the al-kaline reserve in the renal tubule, and for the excretionof hydrogen, which results in a slightly acidic urine.Diuretics that block the effects of carbonic anhydraseslow down the movement of hydrogen ions; as a result,more sodium and bicarbonate are lost in the urine.
These drugs are used as adjuncts to other diureticswhen a more intense diuresis is needed. Acetazolamide isused to treat glaucoma, in conjunction with other drugs totreat epilepsy, and to treat mountain sickness. Metha-zolamide is used primarily for the treatment of glaucoma.
Pharmacokinetics
These drugs are rapidly absorbed and widely distributed.They are excreted in urine. Some of these agents havebeen associated with fetal abnormalities, and they shouldnot be used during pregnancy. Because of the potentialfor adverse effects on the baby, another method of feed-ing the infant should be used if one of these drugs isneeded during lactation.
Contraindications and Cautions
Allergy to the drug, or to antibacterial sulfonamides orthiazides, or chronic noncongestive angle closure glau-coma are contraindications for use. Cautious use is rec-ommended in patients who are breast-feeding or whohave fluid or electrolyte imbalances, renal or hepatic dis-ease, adrenocortical insufficiency, respiratory acidosis, orchronic obstructive pulmonary disease.
Adverse Effects
Adverse effects of carbonic anhydrase inhibitors are re-lated to the disturbances in acid–base and electrolytebalances. Metabolic acidosis is a relatively common andpotentially dangerous effect that occurs when bicarbon-ate is lost. Hypokalemia is also common, because potas-sium excretion is increased as the tubule loses potassiumin an attempt to retain some of the sodium that is beingexcreted. Patients also complain of paresthesias (tingling)of the extremities, confusion, and drowsiness, all of whichare probably related to the neural effect of the electrolytechanges.
Clinically Important Drug–Drug Interactions
There may be an increased excretion of salicylates andlithium if they are combined with these drugs. Cautionshould be used to monitor serum levels of patients takinglithium.
POTASSIUM-SPARING DIURETICS
The potassium-sparing diuretics include amiloride(Midamor), spironolactone (Aldactone), and triamterene(Dyrenium) (Table 51.5). These diuretics are used for pa-tients who are at high risk for hypokalemia associatedwith diuretic use (e.g., patients receiving digitalis, patientswith cardiac arrhythmias). They are not as powerful asthe loop diuretics, but they retain potassium instead ofwasting it.
Therapeutic Actions and Indications
Certain diuretics cause a loss of sodium while retainingpotassium. Spironolactone acts as an aldosterone antag-onist, blocking the actions of aldosterone in the distaltubule. Amiloride and triamterene block potassium se-cretion through the tubule. The diuretic effect of thesedrugs comes from the balance achieved in losing sodiumto offset potassium retained.
Potassium-sparing diuretics are often used as adjunctswith thiazide or loop diuretics or in patients who are es-pecially at risk if hypokalemia develops, such as patientstaking certain antiarrhythmics or digoxin and those whohave particular neurological conditions. Spironolactone,the most frequently prescribed of these drugs, is the drugof choice for treating hyperaldosteronism, a conditionseen in cirrhosis of the liver and nephrotic syndrome.
Focus on the Prototype:Acetazolamide
Indications: Adjunctive treatment of open-angleglaucoma, secondary glaucoma; preoperative usein acute angle-closure glaucoma when delay ofsurgery is indicated; edema caused by CHF,drug-induced edema; centrencephalic epilepsy;prophylaxis and treatment of acute altitude sickness
Actions: Inhibits carbonic anhydrase, which decreases aqueous humor formation in the eye, intraocular pressure, and hydrogen secretion bythe renal tubules
Pharmacokinetics:Route Onset Peak DurationOral 1 hr 2–4 hr 6–12 hrSustained- 2 hr 8–12 hr 18–24 hr
release oralIV 1–2 min 15–18 min 4–5 hr
T1/2: 5 to 6 hr; excreted unchanged in urineAdverse effects: Weakness, fatigue, rash, anorexia,
nausea, urinary frequency, renal calculi, bonemarrow suppression, weight loss

CHAPTER 51 — Diuretic Agents 793
Pharmacokinetics
These drugs are well absorbed, protein bound, andwidely distributed. They are metabolized in the liver andprimarily excreted in urine. These diuretics cross theplacenta and enter breast milk. Routine use during preg-nancy is not appropriate, and they should be saved forsituations in which the mother has pathological reasonsfor use, not pregnancy manifestations or complications,and the benefit to the mother clearly outweighs the riskto the fetus. If one of these drugs is needed during lacta-tion, another method of feeding the baby should be used,because of the potential for adverse effects on fluid andelectrolyte changes in the baby.
Contraindications and Cautions
These drugs are contraindicated for use in patients withallergy to the drug, hyperkalemia, renal disease, or anuria.They are also contraindicated in patients taking amilorideor triamterene. They are given cautiously during preg-nancy and lactation.
Adverse Effects
The most common adverse effect of potassium-sparingdiuretics is hyperkalemia, which can cause lethargy, con-fusion, ataxia, muscle cramps, and cardiac arrhythmias.Patients taking these drugs need to be evaluated regu-
larly for signs of increased potassium and informedabout the signs and symptoms to watch for. They alsoshould be advised to avoid foods that are high in potas-sium (Box 51.4).
Clinically Important Drug–Drug Interactions
The diuretic effect decreases if potassium-sparing di-uretics are combined with salicylates. Dosage adjustmentmay be necessary to achieve therapeutic effects.
Table 51.5 Drugs in Focus
Potassium-Sparing Diuretics
Drug Name Usual Dosage Usual Indications
amiloride (Midamor )
spironolactone (Aldactone )
triamterene (Dyrenium )
15–20 mg/d PO with monitoring of electrolytes
100–200 mg/d PO for edema;100–400 mg/dPO for hyperaldosteronism; 50–100 mg/dPO for hypertension
Pediatric: 3.3 mg/kg per day PO100 mg/d PO b.i.d.
All of the potassium-sparing diuretics are indi-cated for the adjunctive treatment of edemacaused by congestive heart failure, liver disease, or renal disease; hypertension; hyperkalemia; and hyperaldosteronism
Special considerations: Not for use in childrenSpecial considerations: Can be used in chil-
dren with careful monitoring of electrolytes
Special considerations: Not for use in children
BOX 51.4
Potassium-Rich Foods
avocados bananas broccoli cantaloupe dried fruitsgrapefruit lima beans nuts navy beans orangespeaches potatoes prunes rhubarb Sanka coffeesunflower seeds spinach tomatoes watermelon
Focus on the Prototype:Spironolactone
Indications: Primary hyperaldosteronism, adjunctivetherapy in the treatment of edema associated withCHF, nephritic syndrome, hepatic cirrhosis;treatment of hypokalemia or prevention of hy-pokalemia in patients at high risk if hypokalemiaoccurs; essential hypertension
Actions: Competitively blocks the effects of aldos-terone in the renal tubule, causing loss of sodiumand water and retention of potassium
Pharmacokinetics:Route Onset Peak DurationOral 24–48 hr 48–72 hr 48–72 hr

794 PART IX — Drugs Acting on the Renal System
the vascular system from extravascular spaces, includingthe aqueous humor. Therefore, these drugs are oftenused in acute situations when it is necessary to decreaseintraocular pressure before eye surgery or during acuteattacks of glaucoma. Mannitol is also used to decrease in-tracranial pressure, to prevent the oliguric phase of renalfailure, and to promote the movement of toxic sub-stances through the kidneys.
Pharmacokinetics
These drugs are freely filtered at the renal glomerulus,poorly reabsorbed by the renal tubule, not secreted by thetubule, and resistant to metabolism. Their action dependson the concentration of the osmotic activity in the solu-tion. It is not known whether these drugs can cause fetalharm, so their use during pregnancy should be limited tosituations in which the benefit to the mother outweighsthe potential risk to the fetus. Effects of these drugs dur-ing lactation are not well understood; because of the po-tential for risk to the neonate or changes in the fluidbalance of the mother, caution should be used if one ofthese drugs is needed during lactation.
Contraindications and Cautions
Renal disease and anuria from severe renal disease, pul-monary congestion, intracranial bleeding, dehydration,and CHF are contraindications to use.
Adverse Effects
The most common and potentially dangerous adverse ef-fect related to osmotic diuretics is the sudden drop in fluidlevels. Nausea, vomiting, hypotension, light-headedness,confusion, and headache can be accompanied by cardiacdecompensation and even shock. Patients receiving thesedrugs should be closely monitored for fluid and electrolyteimbalance.
Table 51.6 Drugs in Focus
Osmotic Diuretics
Drug Name Usual Dosage Usual Indications
glycerin (Osmoglyn )
isosorbide (Ismotic)
mannitol(Osmitrol )
urea (Ureaphil )
1–1.5 mg/kg PO for glaucoma
1.5 g/kg PO b.i.d.–q.i.d.
50–100 g IV for oliguria; 1.5–2 g/kg IV to reduce intracranial pressure; dosage not establishedfor children <12 y
1–1.5 g/kg IV, do not exceed 120 g/dPediatric: 0.5–1.5 mg/kg IV; as little as
0.1 mg/kg may be sufficient in children <2 y
Treatment of elevated intracranial pressure (IV);glaucoma (PO)
Treatment of glaucoma
Treatment of elevated intracranial pressure; renalfailure; acute glaucoma
Treatment of elevated intracranial pressure; acuteglaucoma
T1/2: 20 hr; metabolized in the liver and excreted inurine
Adverse effects: Dizziness, headache, drowsiness,rash, cramping, diarrhea, hyperkalemia, hirsutism,gynecomastia, deepening of the voice, irregularmenses
OSMOTIC DIURETICS
Osmotic diuretics pull water into the renal tubule withoutsodium loss. They are the diuretics of choice in cases of in-creased cranial pressure or acute renal failure due toshock, drug overdose, or trauma. The osmotic diureticsinclude two mild agents, glycerin (Osmoglyn) and isosor-bide (Ismotic), and two powerful ones, mannitol (Osmitrol )and urea (Ureaphil) (Table 51.6). Glycerin can be givenintravenously to treat elevated intracranial pressure andis used orally to treat glaucoma. Isosorbide is availableonly in oral form and is a preferred drug for the treatmentof glaucoma. Mannitol, which is available only for intra-venous use, is the mainstay for treatment of elevated in-tracranial pressure and acute renal failure. Urea also isavailable only for intravenous use; it is indicated for re-duction of intracranial pressure and in the treatment ofacute glaucoma.
Therapeutic Actions and Indications
Some nonelectrolytes are used intravenously to increasethe volume of fluid produced by the kidneys. Mannitol,for example, is a sugar that is not well reabsorbed by thetubules; it acts to pull large amounts of fluid into theurine by the osmotic pull of the large sugar molecule.Because the tubule is not able to reabsorb all of the sugarpulled into it, large amounts of fluid are lost in the urine.The effects of these osmotic drugs are not limited to thekidneys, because the injected substance pulls fluid into

NURSING CONSIDERATIONS FORPATIENTS RECEIVING DIURETICS
Assessment: History and Examination
Screen for the following conditions, which could be cau-tions or contraindications to use of the drug: any known al-lergies to diuretics; fluid or electrolyte disturbances,which could be exacerbated by the diuretic or render the di-uretic ineffective; gout, which reflects an abnormal tubulefunction and could be worsened by the diuretic or reflect acondition that would render the diuretic ineffective; glucosetolerance abnormalities, which may be exacerbated bythe glucose-elevating effects of some diuretics; liver disease,which could alter the metabolism of the diuretic, leading totoxic levels; systemic lupus erythematosus, which fre-quently affects the glomerulus and could be exacerbated by theuse of a diuretic; and pregnancy or lactation, which couldbe affected by the change in fluid and electrolyte balance.
Physical assessment should include the following:thorough skin examination (including color, texture,and the presence of edema), to provide a baseline as a ref-erence for drug effectiveness; assessment of blood pres-sure, pulse, and cardiac auscultation, to provide a baselinefor effects on blood pressure and volume; assessment of body
weight, to provide a baseline to monitor fluid load; liverevaluation, to determine potential problems in drug metab-olism; check of urinary output, to establish a baseline ofrenal function; and evaluation of blood tests, to provide abaseline reference for electrolyte balance, glucose levels, uricacid levels, and liver function tests.
Nursing Diagnoses
The patient receiving a diuretic may have the follow-ing nursing diagnoses related to drug therapy:• Risk for Deficient Fluid Volume related to diuretic
effect• Impaired Urinary Elimination related to diuretic
effect• Imbalanced Nutrition: Less Than Body Require-
ments related to GI upset and metabolic changes• Deficient Knowledge regarding drug therapy
Implementation With Rationale
• Administer oral drug with food or milk, to buffer thedrug effect on the stomach lining if GI upset is a problem.
• Administer intravenous drug slowly, to prevent severechanges in fluid and electrolytes; protect the drug fromlight, because disintegration can occur; discard diluteddrug after 24 hours, to prevent contamination or in-effective drug use.
• Continuously monitor urinary output, cardiac re-sponse, and heart rhythm of patients receiving intra-venous diuretics, to monitor for rapid fluid switch andpotential electrolyte disturbances leading to cardiac ar-rhythmia. Switch to the oral form, which is less potentand easier to monitor, as soon as possible.
• Administer early in the day, so that increased urinationwill not interfere with sleep.
• Monitor the dose carefully and reduce the dosageof one or both drugs if given with antihypertensiveagents; loss of fluid volume can precipitate hypotension.
• Monitor the patient response to the drug (e.g., bloodpressure, urinary output, weight, serum electrolytes,hydration, periodic blood glucose monitoring), toevaluate the effectiveness of the drug and monitor for ad-verse effects.
• Provide comfort measures, including skin care andnutrition consultation, to increase compliance to drugtherapy and decrease severity of adverse effects; providesafety measures if dizziness and weakness are aproblem.
• Provide potassium-rich or potassium-poor diet asappropriate for drug being given, to maintain elec-trolyte balance and replace lost potassium.
• Provide thorough patient teaching, including mea-sures to avoid adverse effects and warning signs ofproblems and ways to incorporate the diuretic’s effect
CHAPTER 51 — Diuretic Agents 795
Focus on the Prototype:Mannitol
Indications: Prevention and treatment of oliguricphase of renal failure; reduction of intracranialpressure and treatment of cerebral edema; reduc-tion of elevated intraocular pressure; promotionof urinary excretion of toxic substances; diagnos-tic use for measurement of glomerular filtrationrate; irrigant in transurethral prostatic resectionand other transurethral procedures
Actions: Elevates the osmolarity of the glomerularfiltrate, leading to a loss of water, sodium, andchloride; creates an osmotic gradient in the eye,reducing intraocular pressure; creates an osmoticeffect that decreases swelling after transurethralsurgery
Pharmacokinetics:Route Onset Peak DurationIV 30–60 min 1 hr 6–8 hrIrrigant Rapid Rapid Short
T1/2: 15 to 100 min; excreted unchanged in urineAdverse effects: Dizziness, headache, hypotension,
rash, nausea, anorexia, dry mouth, thirst, diuresis,fluid and electrolyte imbalances

loss of water, sodium, and potassium. Thesedrugs are the most potent diuretics and are usedin acute situations as well as chronic conditionsnot responsive to milder diuretics.
• Carbonic anhydrase inhibitors work to block theformation of carbonic acid and bicarbonate inthe renal tubule. These drugs can cause an alka-line urine and loss of the bicarbonate buffer.Carbonic anhydrase inhibitors are used in com-bination with other diuretics when a stronger di-uresis is needed, and they are frequently used totreat glaucoma because they decrease theamount of aqueous humor produced in the eye.
• Potassium-sparing diuretics are mild diureticsthat act to spare potassium in exchange for theloss of sodium and water in the urine. These di-uretics are preferable if potassium loss could bedetrimental to a patient’s cardiac or neuro-muscular condition. Patients must be careful notto become hyperkalemic while taking these drugs.
• Osmotic diuretics use hypertonic pull to re-move fluid from the intravascular spaces andto deliver large amounts of water into the renaltubule. There is a danger of sudden change of fluid volume and massive fluid loss withsome of these drugs. These drugs are used to decrease intracranial pressure, to treat glaucoma, and to help push toxic substancesthrough the kidney.
• Patients receiving diuretics need to be moni-tored for fluid loss and retention (daily weights,blood pressure, skin evaluation, urinary output);have periodic electrolyte evaluations and bloodglucose determinations; and have evaluations ofthe effectiveness of their teaching program.
GETTING READY FOR THE NCLEX
Answers to the questions in this chapter may be foundin “Answers to NCLEX Review Questions” on theCD-ROM in the front of the book.
Multiple Choice Questions
1. Diuretics are not currently recommended for thetreatment ofa. hypertension.b. renal disease.c. obesity.d. severe liver disease.
2. Most diuretics act in the body to causea. loss of water.b. loss of sodium.c. retention of potassium.d. retention of chloride.
796 PART IX — Drugs Acting on the Renal System
in planning the day’s activities, to enhance patientknowledge about drug therapy and to promote compliance.
Evaluation
• Monitor patient response to the drug (weight, uri-nary output, edema changes, blood pressure).
• Monitor for adverse effects (electrolyte imbalance, or-thostatic hypotension, rebound edema, hyperglycemia,increased uric acid levels, acid–base disturbances,dizziness).
• Evaluate the effectiveness of the teaching plan (pa-tient can name drug, dosage, adverse effects to watchfor, specific measures to avoid adverse effects).
• Monitor the effectiveness of comfort measures andcompliance to the regimen
WEB LINKS
Health care providers and patients may want to consultthe following Internet sources:
http://www.tmc.edu/thi/diurmeds.html Informationon diuretics, good teaching guides and aids.
http://www.americanheart.org andhttp://www.nhlbi.nih.gov Information on CHF,pathophysiology, treatment, and research.
http://cpmcnet.columbia.edu/dept/gi/other.htmlInformation on liver disease and related treatment.
Points to Remember
• Diuretics are drugs that increase the excretion ofsodium, and therefore water, from the kidneys.
• Diuretics are used in the treatment of edemaassociated with CHF and pulmonary edema,liver failure and cirrhosis, and various types ofrenal disease, and as adjuncts in the treatmentof hypertension.
• Diuretics must be used cautiously in any condi-tion that would be exacerbated by changes influid and electrolyte balance.
• Adverse effects associated with diuretics includeelectrolyte imbalance (potassium, sodium, chloride); hypotension and hypovolemia; hypoglycemia; and metabolic alkalosis.
• Classes of diuretics differ in their site of actionand intensity of effects. Thiazide diuretics workto block the chloride pump in the distal convo-luted tubule. This effect leads to a loss of sodiumand potassium and a minor loss of water.Thiazides are frequently used alone or in combi-nation with other drugs to treat hypertension.They are considered to be mild diuretics.
• Loop diuretics work in the loop of Henle andhave a powerful diuretic effect, leading to the

3. Diuretics cause a loss of blood volume in the body.The drop in volume activates compensatorymechanisms to restore the volume, includinga. suppression of ADH release.b. suppression of aldosterone release.c. activation of the renin–angiotensin system
with increased ADH and aldosterone.d. stimulation of the countercurrent mechanism.
4. Thiazide diuretics are considered mild diureticsbecausea. they block the sodium pump in the loop of
Henle.b. they block the chloride pump, which causes
loss of sodium and chloride but little water.c. they do not cause a fluid rebound when they
work in the kidneys.d. they have no effect on electrolytes.
5. A loop diuretic would be the drug of choice intreatinga. hypertension.b. shock.c. pulmonary edema.d. fluid retention of pregnancy.
6. Any patient receiving a loop diuretic needs tohave regular monitoring ofa. sodium levels.b. bone marrow function.c. calcium levels.d. potassium levels.
7. The diuretic of choice for treating hyperaldo-steronism would bea. spironolactone.b. furosemide.c. hydrochlorothiazide.d. acetazolamide.
8. A patient with severe glaucoma who is about toundergo eye surgery would benefit from a de-crease in intraocular fluid. This is often bestaccomplished by giving the patienta. a loop diuretic.b. a thiazide diuretic.c. a carbonic anhydrase inhibitor.d. an osmotic diuretic.
9. Routine nursing care of a patient receiving a di-uretic would not includea. daily weights.b. tight fluid restrictions.c. periodic electrolyte evaluations.d. monitoring of urinary output.
10. Patients receiving diuretics should be taught toreporta. yellow vision.b. weight loss of 1 lb/day.
c. muscle pain or cramping.d. increased urination.
Definitions
Define the following terms.
1. edema ____________________________________
2. fluid rebound ______________________________
3. thiazide diuretic ____________________________
4. hypokalemia _______________________________
5. high-ceiling diuretics ________________________
6. alkalosis ___________________________________
7. hyperaldosteronism _________________________
8. osmotic pull _______________________________
Matching
Match the diuretic with the appropriate class. (Someclasses will be used more than once.)
1. ____________ glycerin
2. ____________ acetazolamide
3. ____________ furosemide
4. ____________ benzthiazide
5. ____________ indapamide
6. ____________ mannitol
7. ____________ spironolactone
8. ____________ hydrochlorothiazide
9. ____________ amiloride
10. ____________ bumetanide
A. OsmoticB. ThiazideC. LoopD. Potassium-sparingE. Carbonic anhydrase inhibitor
BIBLIOGRAPHY AND REFERENCES
Bullock, B. L. (2000). Focus on pathophysiology. Philadelphia:Lippincott Williams & Wilkins.
Drug facts and comparisons. (2004). St. Louis: Facts and Comparisons.Gilman, A., Hardman, J. G., & Limbird, L. E. (Eds.). (2002).
Goodman and Gilman’s the pharmacological basis of therapeutics(10th ed.). New York: McGraw-Hill.
Karch, A. M. (2004). 2005 Lippincott’s nursing drug guide.Philadelphia: Lippincott Williams & Wilkins.
Professional’s guide to patient drug facts. (2004). St. Louis: Facts andComparisons.
CHAPTER 51 — Diuretic Agents 797