Embed Size (px)
Citation preview
OROFACIAL NEURALGIES AND NEUROPATHIC PAIN
The International Association for the Study of Pain's widely used definition states: "Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage."
Pain is the most common symptom for which patients seek help. Approximately 40% of the British population only visit a dentist for pain relief.
Orofacial Pain1- Diseases of teeth and/or supporting tissues
2- Oral mucosal diseases.3- Diseases of the jaw.4- Pain in edentulous patient.5- Postoperative pain.6- Pain triggered by mastication.7- Referred pain.8- Neurological diseases.9- Psychogenic (atypical) facial pain.
Diseases of teeth and/or supporting tissues
1. Pulpitis.
2. Periapical periodontitis.
3. Dentine hypersensitivity, cracked tooth or cracked cusp syndrome.
4. Lateral (periodontal) abscess.
5. Acute necrotising ulcerative gingivitis.
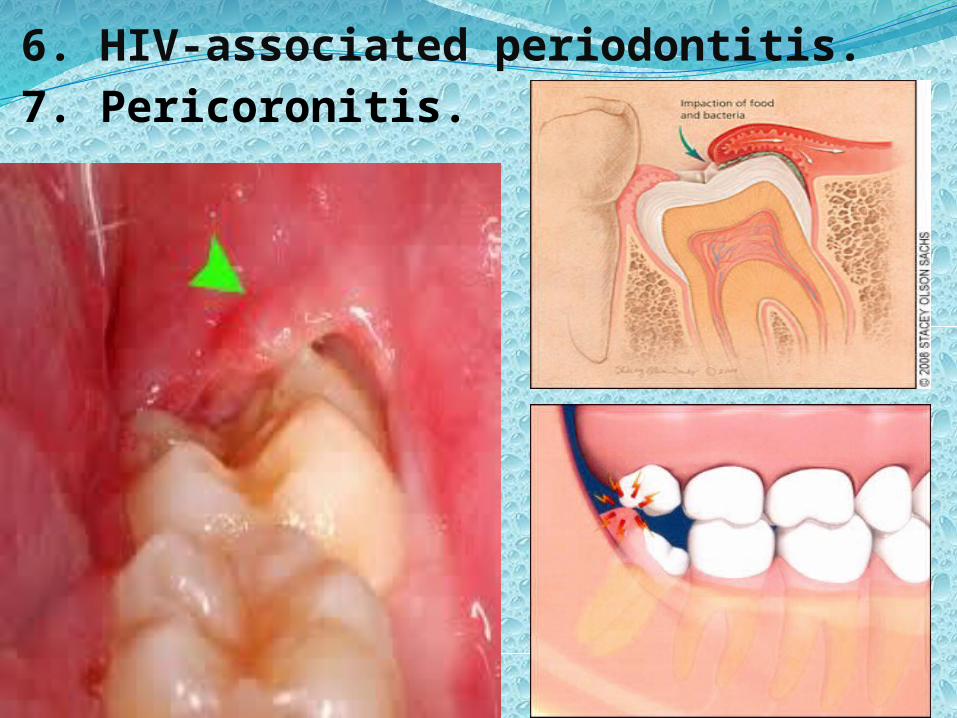
6. HIV-associated periodontitis.7. Pericoronitis.
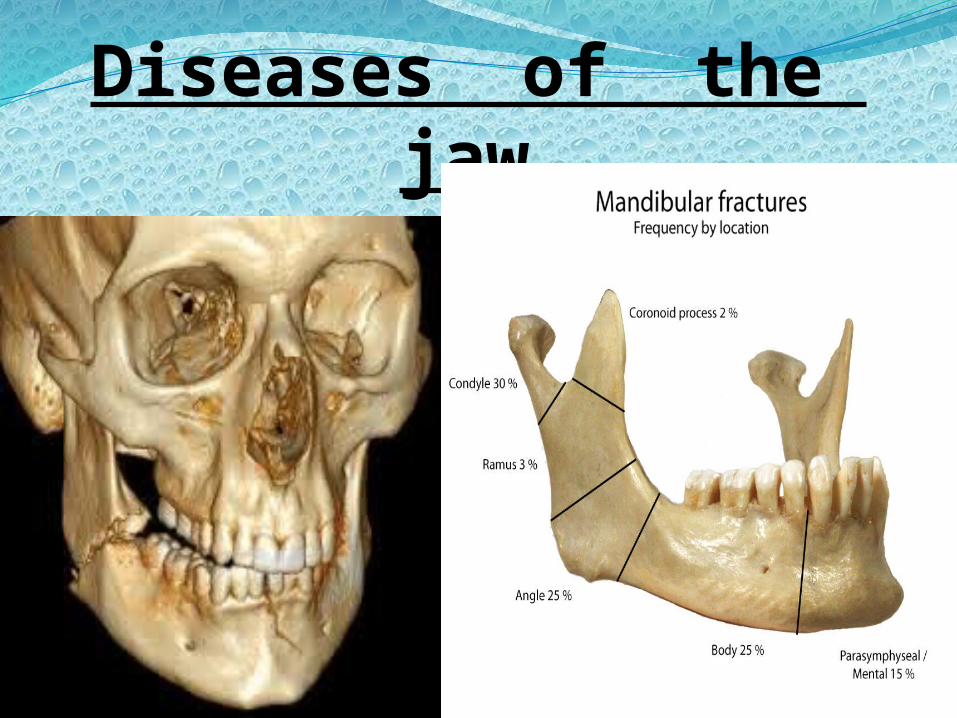
Diseases of the jaw1- Fractures.
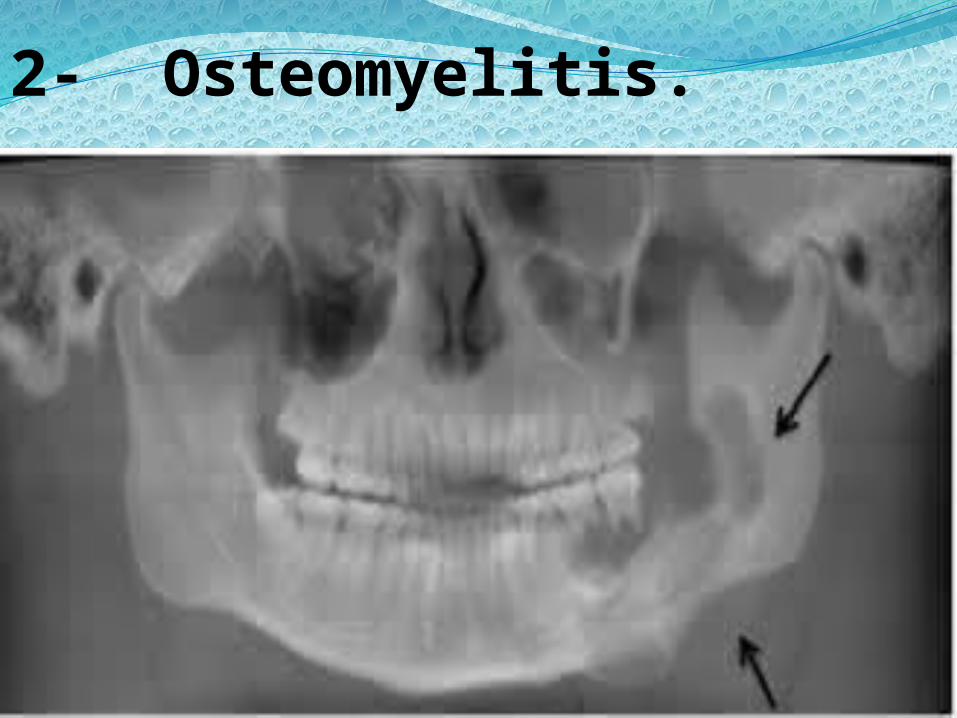
2- Osteomyelitis.
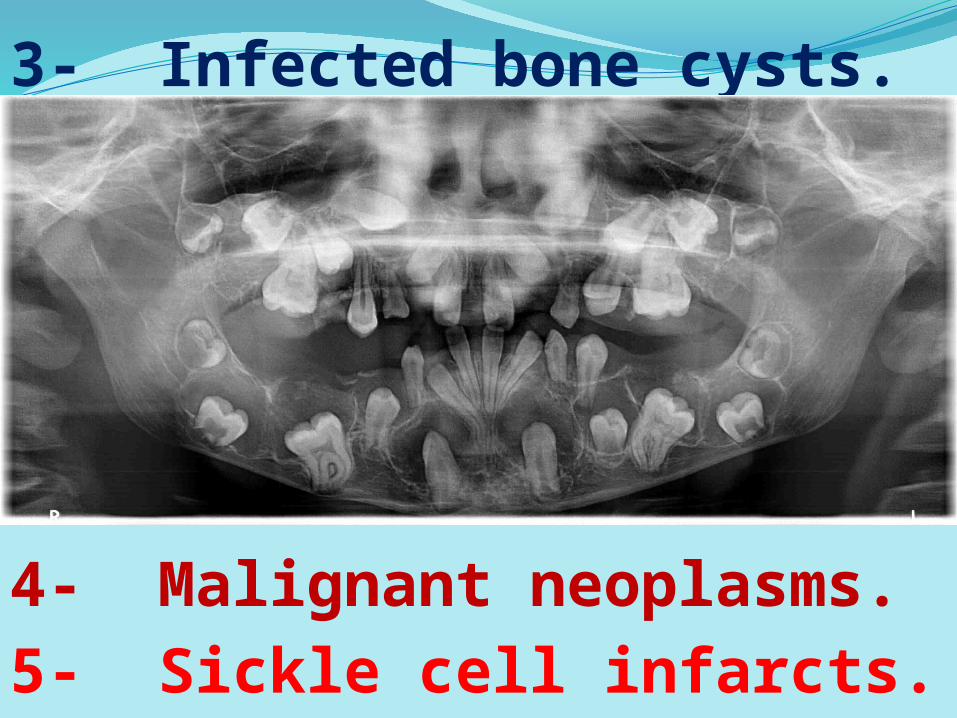
3- Infected bone cysts.
4- Malignant neoplasms.5- Sickle cell infarcts.
Pain in the edentulous patient1- Denture trauma (such as traumatic ulcers).
2- Excessive vertical dimension ( such as TMJ dysfunction syndrome ).
3- Diseases of the denture-bearing mucosa (such as denture induced candidiasis).
4- Diseases of the jaws (such as residual cyst).
5- Teeth or roots erupting under a denture.
Postoperative pain1- Alveolar osteitis
(dry socket)
2- Fracture of the
jaw
3- Damage to the temporomandibular joint
4- Osteomyelitis
5- Damage to nerve trunks or involvement of nerves in scar tissue
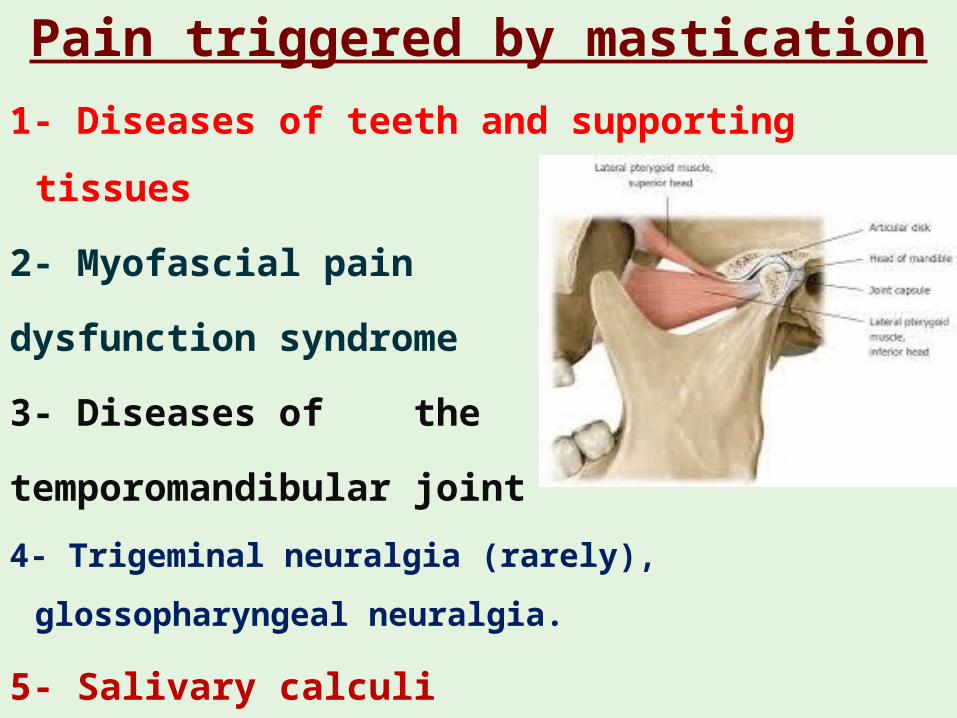
Pain triggered by mastication1- Diseases of teeth and supporting tissues
2- Myofascial pain
dysfunction syndrome
3- Diseases of the
temporomandibular joint4- Trigeminal neuralgia (rarely),
glossopharyngeal neuralgia.
5- Salivary calculi
7- Pain from extraoral diseases (referred pain)
Antral disease can cause pain felt in the upper teeth but aradiograph and clinical diagnosisshould provide the diagnosisSalivary gland and ear diseases typically cause preauricular pain. They may simulate temporomandibular joint symptoms but are rarely mistaken for dental problems.
8- Neurological diseases1. Trigeminal neuralgia
2. Glossopharyngeal neuralgia
3. Multiple sclerosis
4. Herpes zoster
5. Postherpetic neuralgia
6. Migrainous neuralgia
7. Intracranial tumours
8. Bell's palsy
Trigeminal neuralgiaThe typical features are elderly patients are affected.
The pain is paroxysmal, i.e. severe, sharp and stabbing in
character, but lasts only seconds or minutes
The severity of the pain may also make the patient depressed.
During an attack the patient's face is often distorted with
anguish, while between attacks the patient may appear
apprehensive at the thought of recurrence.
Stimuli to an area (trigger zone) within the distribution of the
trigeminal nerve can provoke an attack.
Common stimuli are touching, draughts of cold air, or
teeth brushing. Occasionally, masticatory effort induces
the pain.
Either the second or third division of the trigeminal
nerve is usually first affected, but pain soon involves
both. The first division is rarely affected and pain does
not spread to the opposite side.
Diagnosis, should be readily made from the features
described, with the absence of objective sensory loss
and absence of any detectable organic cause.
Treatment In the absence of disease, teeth should not be arbitrarily
extracted, as this only adds to the patient's misfortunes.
The most effective drugs are anticonvulsants, particularly
carbamazepine and to a lesser extent phenytoin.
Carbamazepine, with or without phenytoin, will usually
relieve the pain, at least for a time.
Abolition of the pain of T. N. by giving anticonvulsant,
such as carbamazepine, also helps to confirm the
diagnosis.
Carbamazepine ( l00mg/day gradually raised if necessary to 800mg/day ), must be given long-term (essentially prophylactically) to reduce the frequency and severity of attacks.
A few patients are unresponsive to carbamazepine or cannot tolerate the side-effects.
If drug treatment fails, the final resort is surgery. The simplest option is cryotherapy to the trigeminal nerve or, if this fails, cryotherapy at the base of the skull.
If these fail, microvascular decompression of the trigeminal ganglion may be required.
Glossopharyngeal neuralgiaThis rare condition is characterised by pain similar to
that of T. N. but felt in the base of the tongue and faces on one side.
It may also radiate deeply into the ear. The pain is sharp, lancinating and transient.
The pain is typically triggered by swallowing, chewing, or coughing.
It may be so severe that patients may be frightened to swallow their saliva and try to keep the mouth and tongue as completely immobile as possible.
Glossopharyngeal neuralgia sometimes responds to carbamazepine, but less often than T. N. .
Once an organic cause has been excluded, surgical treatment may be needed. However, like trigeminal neuralgia, there can be spontaneous remissions, sometimes for years.
Paraesthesia and Dysaesthesia of the lipParaesthesia of the lip can be caused by osteomyelitis or fracture of the jaw. Very occasionally it results from neurological disease.Prolonged anaesthesia or paraesthesia of the lip can occasionally follow inferior dental blocks, possibly as a result of damage to the nerve by the needle.
A jaw tumour causing pain or paraesthesia strongly suggests malignancy.
Herpes zoster affecting the trigeminal nerve can leave residual disturbances of sensation.
Disturbances of sensation of the face and other regions can be caused by multiple sclerosis.
Tetany is the result of hypocalcaemic states and causes heightened neuromuscular excitability together with minor disorders of sensation such as paraesthesia of the lip.
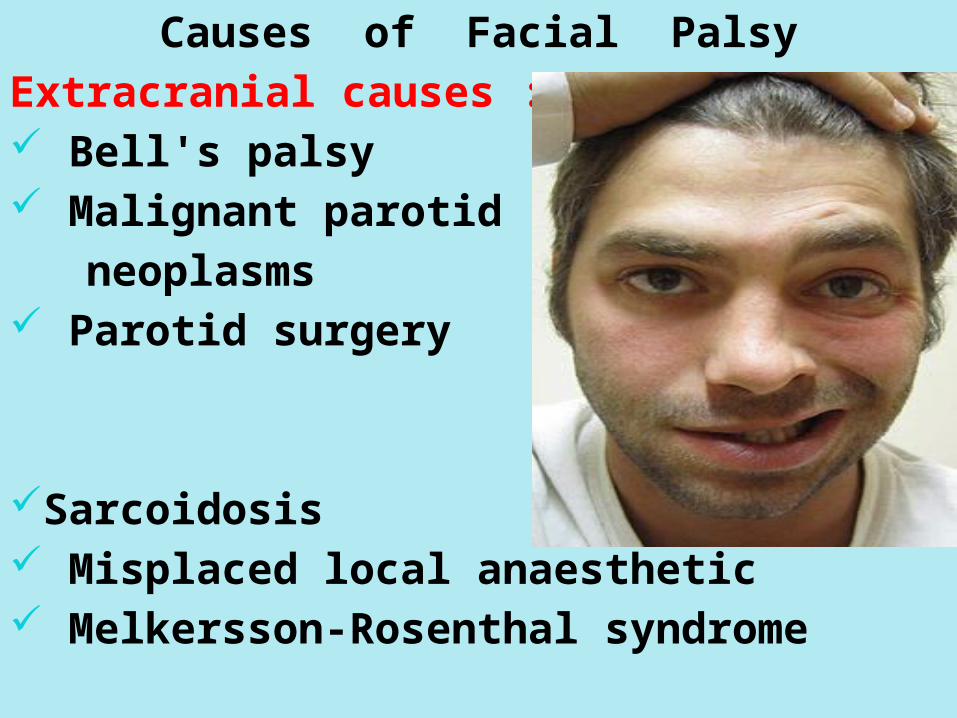
Causes of Facial PalsyExtracranial causes :- Bell's palsy Malignant parotid neoplasms Parotid surgery
Sarcoidosis Misplaced local anaesthetic Melkersson-Rosenthal syndrome
Intracranial causes :- Strokes Cerebral tumours and other neurological diseases
Multiple sclerosis HIV infection Lyme disease Ramsay Hunt syndrome Trauma to the base of the skullFacial paralysis is the general term for used to describe the loss of the ability to move one side of the face, while Bell's palsy is a specific type of facial paralysis.
Bell's palsy is a common cause of facial paralysis. It probably results from compression of the facial nerve in its canal as a result of inflammation and swelling. A viral infection, particularly herpes simplex, is suspected as the cause.
pain in the jaw sometimes precedes the paralysis or there may be numbness in the side of the tongue.
Function of the facial nerve is tested by asking the patient to perform facial movements. When asked to close the eyes, the lids on the affected side cannot be brought together but the eyeball rolls up normally, since the oculomotor nerves are unaffected.
When the patient is asked to smile, the corner of the mouth on the affected side is not pulled upwards and the normal lines of expression are absent.
The wrinkling round the eyes which accompanies smiling is also not seen on the affected side and the eye remains staring.
This is a lower motor neurone lesion unlike the upper motor neurone lesion seen, for example, after a stroke.
The majority of patients recover fully or partially without treatment. At least 10% of patients with Bell's palsy are unhappy about the final outcome because of permanent disfigurement or other complications.
Full recovery is usual in patients with an incomplete palsy seen within a week of onset, but more than half of those with a complete lesion fail to recover completely.
Electromyography and other electrodiagnostic techniques can be used to measure the degree of functional impairment as a guide to the need for treatment.
Prednisolone, by mouth ( 20 mg four times a day ) may be given for 5-10 days and then tapered off over the following 4 days, and may be effective if given within 24 hours of the onset. The addition of acyclovir appears to produce more reliable results and also suggests a role for a herpes virus.