Embed Size (px)
Citation preview
American College of Gastroenterology
Guideline on the Management of H. pylori
Infection (Am J Gastroenterol
2007;102:1808–1825)
Current concepts in management of
H.pylori pylori infection - The Maastricht III
consensus report
Sleisenger and fordtran 9th edition.
Wikepedia
Indian Journal of Gastroenterology 2006 Vol
25 January - February
Campylobacter pyloridis (1983)
C.pylori (1987)
H.pylori (1989)
Gram negative organism with following characteristics:Slow growing
Microaerophilic
Highly motile (multiple unipolarflagella)
Spiral
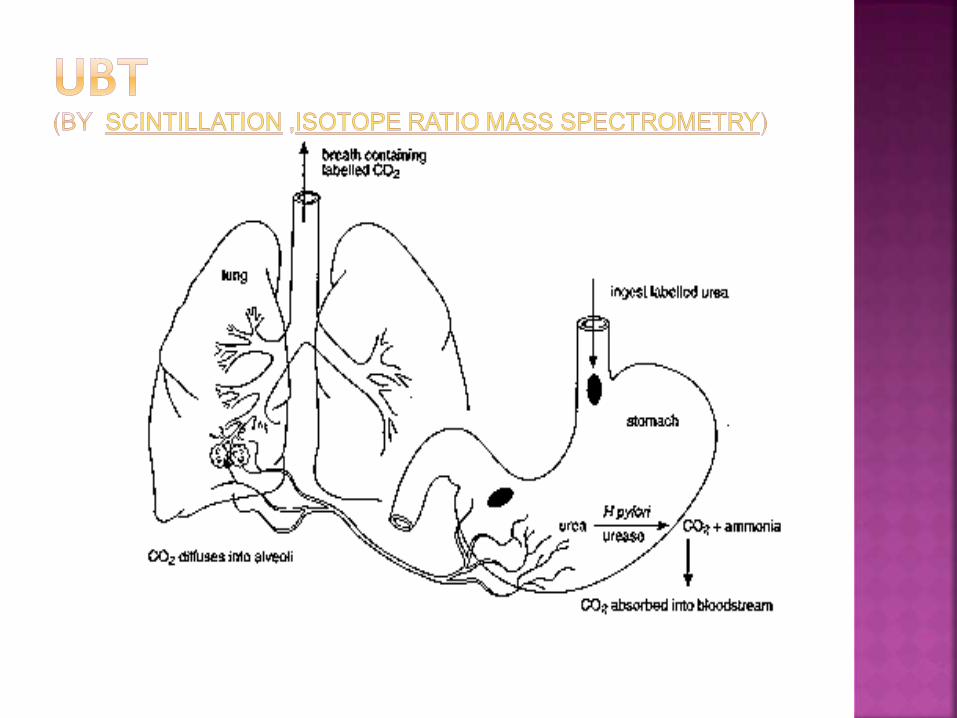
Urease producing
Urease
C=O(NH2)2 + H+ + 2H2O HCO3- + (NH4
+)
Urea Bicarbonate Ammonium
ions
And then…
HCO3- CO2 + OH-
0.5-0.9μm wide and 2-4μm long
7 flagellae, 12-15nm long, covering continuous with outer membrane of the body, terminal bulbs?function, thick outer glycocalyx
Bacillary to coccoid ; infectious form bacillary
Best known culture medium : oxoid brain heart infusion agar (BHI)
Notable for its high content of urease and alkaline phosphatase; produces catalase and cytochromeoxidase
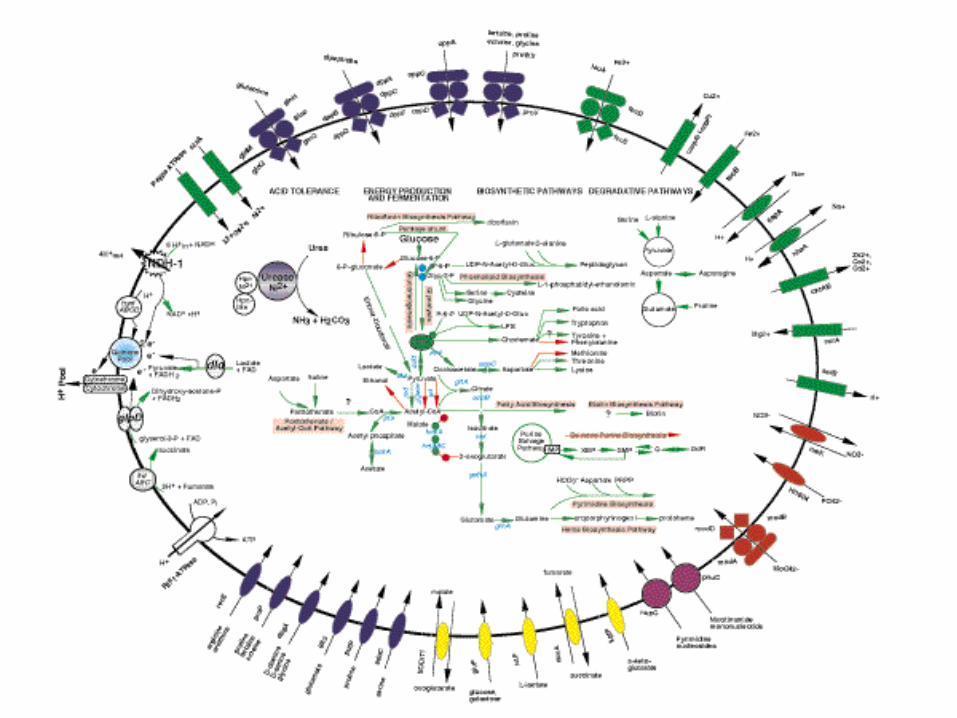
Single circular molecule, mean size of 1.7Mb
Complete sequence determined in 1997
Codes for about 1500 proteins
Many genes can be switched on and off
Genome changes continuously (DNA
importing)
Nature 388, 539 - 547 (07 August 1997)
The complete genome sequence of the gastric pathogen Helicobacter
pylori
JEAN-F. TOMB*, OWEN WHITE*, ANTHONY R. KERLAVAGE*, REBECCA A. CLAYTON*,
GRANGER G. SUTTON*, ROBERT D. FLEISCHMANN*, KAREN A. KETCHUM*,
HANS PETER KLENK*, STEVEN GILL*, BRIAN A. DOUGHERTY*, KAREN NELSON*,
JOHN QUACKENBUSH*, LIXIN ZHOU*, EWEN F. KIRKNESS*, SCOTT PETERSON*,
BRENDAN LOFTUS*, DELWOOD RICHARDSON*, ROBERT DODSON*, HANIF G. KHALAK*,
ANNA GLODEK*, KEITH MCKENNEY*, LISA M. FITZEGERALD*, NORMAN LEE*,
MARK D. ADAMS*, ERIN K. HICKEY*, DOUGLAS E. BERG†, JEANINE D. GOCAYNE*,
TERESA R. UTTERBACK*, JEREMY D. PETERSON*, JENNY M. KELLEY*,
MATTHEW D. COTTON*, JANICE M. WEIDMAN*, CLAIRE FUJII*, CHERYL BOWMAN*,
LARRY WATTHEY*, ERIK WALLIN‡, WILLIAM S. HAYES§, MARK BORODOVSKY§, *
The Institute for Genomic Research, 9712 Medical Center Drive, Rockville, Maryland 20850,
USA
One of the most common chronic bacterial
pathogen in human
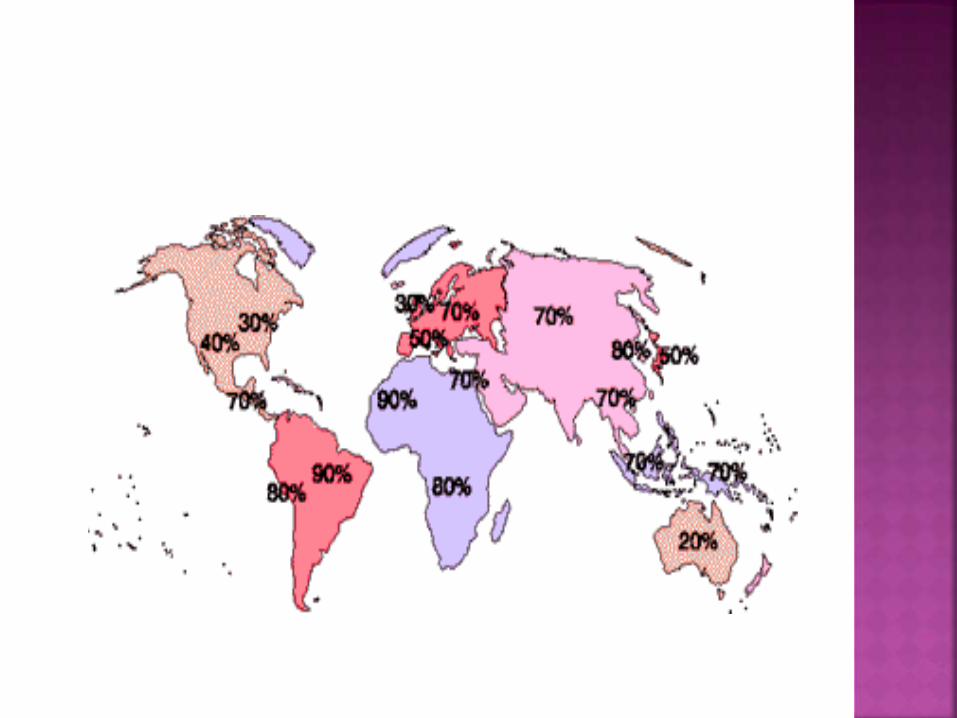
Approximately 50% of the world’s population is
infected.
Developing countries > Developed countries
In developing nations prevalence reaches >80% by
the age of 50.
Earlier age of acquisition.
United States:
30% of total population infected
• Of those, ~1% per year develop duodenal
ulcer
• ~1/3 eventually have peptic ulcer
disease(PUD)
70% gastric ulcer cases colonized with H.
pylori.
Prevalence of H. pylori strongly varies
between developing and developed
countries, where prevalence among adults is
typically around 80–90% and < 40%,
respectively.
Furthermore, Helicobacter pylori is the main
cause of gastritis, responsible for 80% of
gastric and 95% of duodenal ulcers.
90%-95% of Indian subjects with DU are
positive for H. pylori compared to 80% of
asymptomatic healthy individuals in the
community.
Duodenal-to-gastric ulcer ratio was 12:1.
Helicobacter pylori was present in 11/13
(84.6%) subjects with peptic ulcer.(Epidemiology of Helicobacter pylori and peptic ulcer in
India Journal of gastroenterology and
hepatology ISSN 0815-9319 Source / Source
2002, vol. 17, no6, pp. 659-665 (41 ref.))
Risk factors: Age, Socio-economic status,
Overcrowding, lack of hot or running water.
In developed countries, age related increase
in prevalence – just a birth cohort
phenomenon.
Genetic factors :
Monozygotic twins reared apart had a
higher rate of concordance of infection than
did age-matched dizygotic twins.
Reservoir:
Humans – major
Domestic cats, sheep – minor
Transmission: MODES
fecal-oral,
oral-oral,
gastro-oral
Helicobacter pylori is the main cause of
gastritis, responsible for 80% of gastric and
95% of duodenal ulcers.
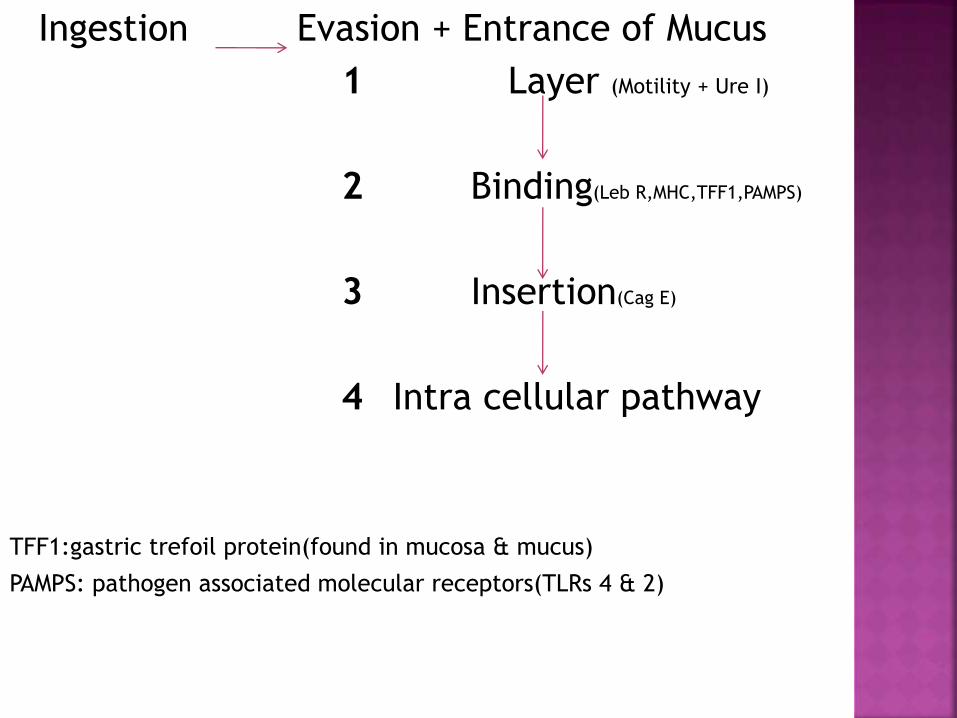
Ingestion Evasion + Entrance of Mucus
1 Layer (Motility + Ure I)
2 Binding(Leb R,MHC,TFF1,PAMPS)
3 Insertion(Cag E)
4 Intra cellular pathway
TFF1:gastric trefoil protein(found in mucosa & mucus)
PAMPS: pathogen associated molecular receptors(TLRs 4 & 2)
Type IV secretions apparatus(1) (translocate cagA)
Possible insertion by needle like organelle coated with a sheath (Cag 7 protein) [Rohde et al]
Cag A translocates into the host cell cytoplasm & tyrosine phosphorylated by Src kinase and through the interaction mantains epithelial morphology
Cytokine Production Growth Factor
IL- 8+ chemokines Like cellular response
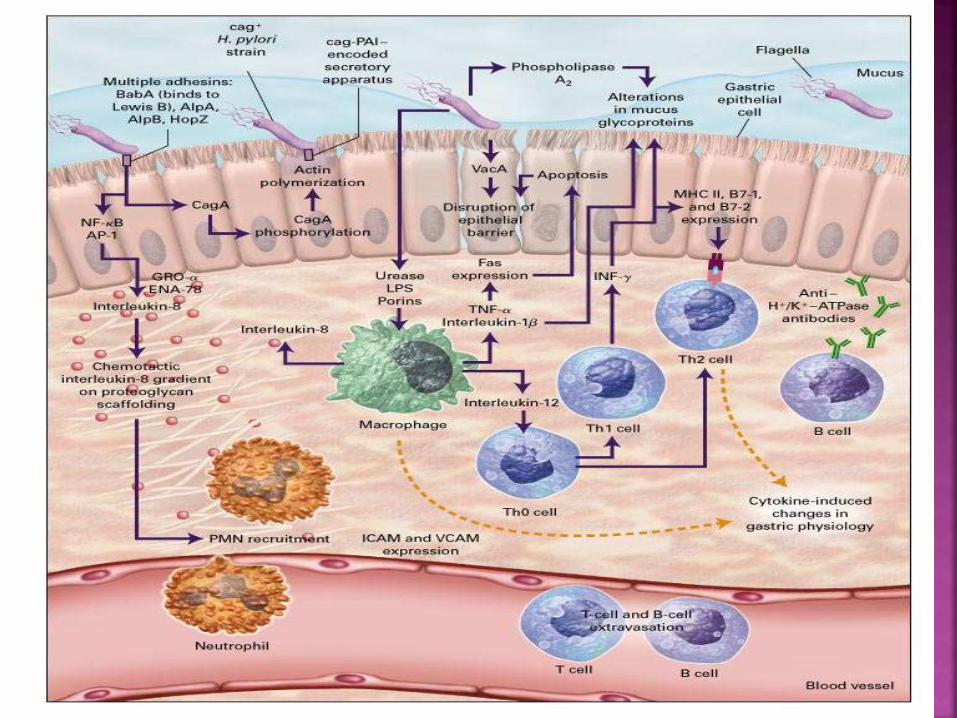
Polymorphisms in the regions controlling IL-
1β : gastric cancer and reduced incidence of
DU, Reduced acid secretion
Genes that regulate magnitude of
inflammation:
IL-10,
IL-1B
Tumor necrosis factor-α (TNF-α), and
IL-8
Oip A: outer inflammatory protein A
Increased bacterial density,
Mucosal IL-8 levels, and
Neutrophil infiltration,
More severe clinical consequences
Type IV secretion system – peptidoglycan--
NOD 1 – activation of NF-kB – IL-8
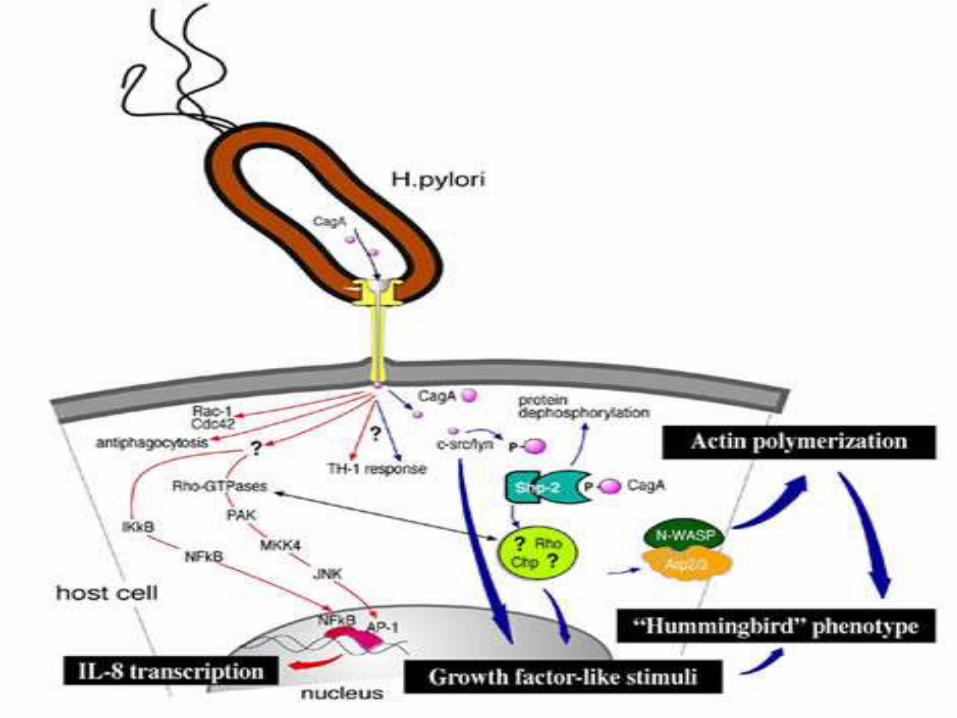
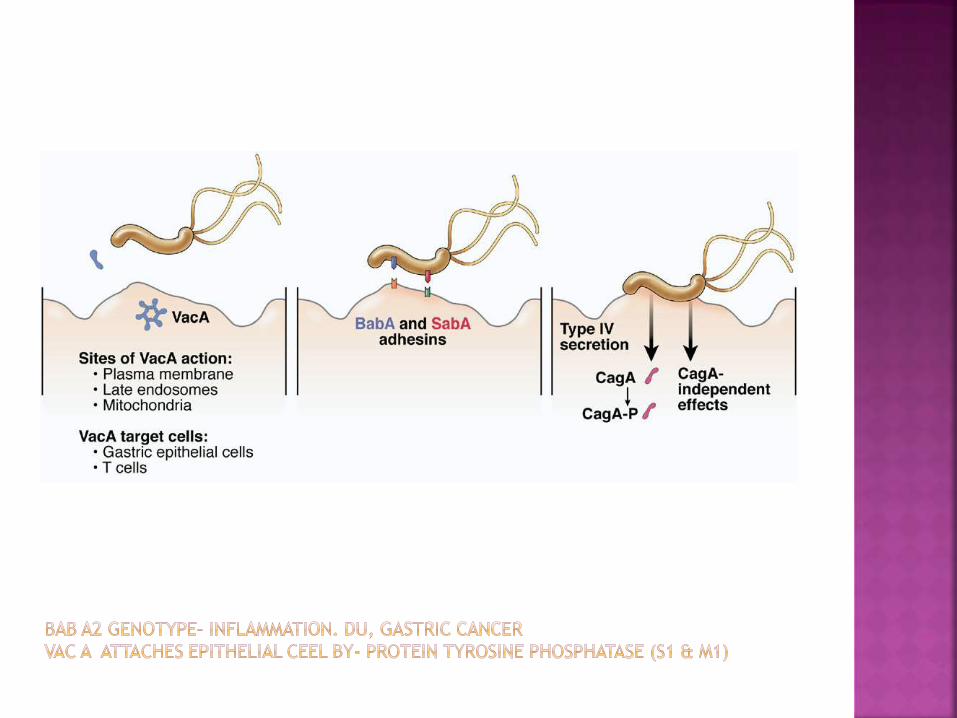
The Helicobacter pylori virulence factor
CagA is implicated in the pathogenesis of
gastric disorders such as chronic gastritis,
peptic ulcers and gastric cancer. CagA is
translocated into H. pylori-infected cells,
where it interacts with cellular scaffolding
and signalling proteins, causing host-cell
elongation and dispersal, and giving rise to
the so-called 'scattering/hummingbird'
phenotype
Role of oxidative stress:
Regultes gene expression
Redox factor-1(apurinic-apyrimidinic
endonuclease-1): involved in redox sensitive
signaling and contibuting to activation of NF-
kB & AP-1.
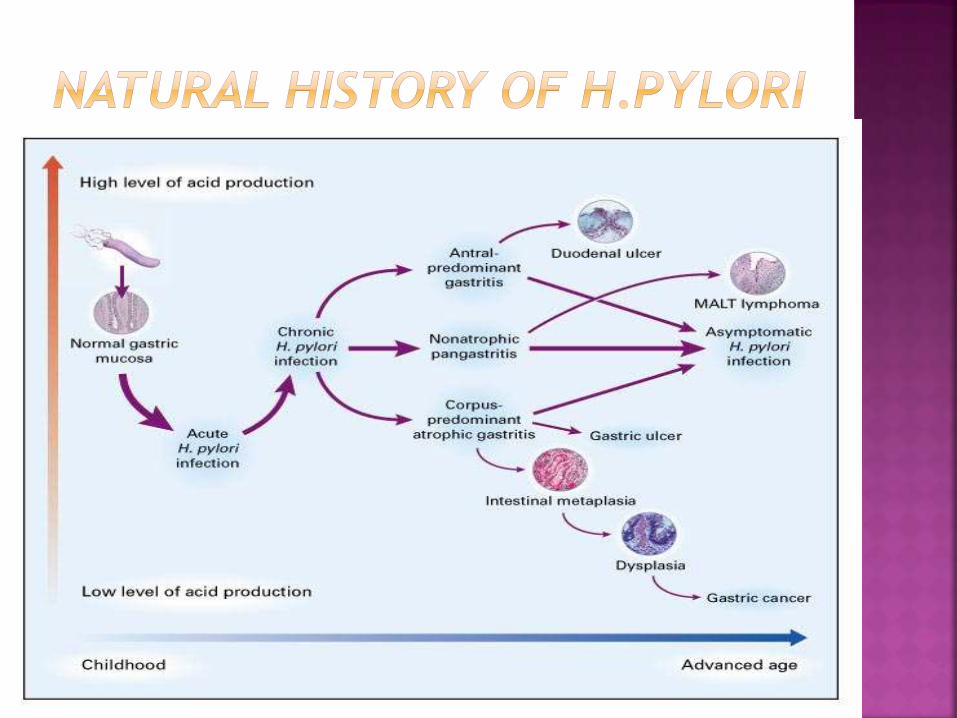
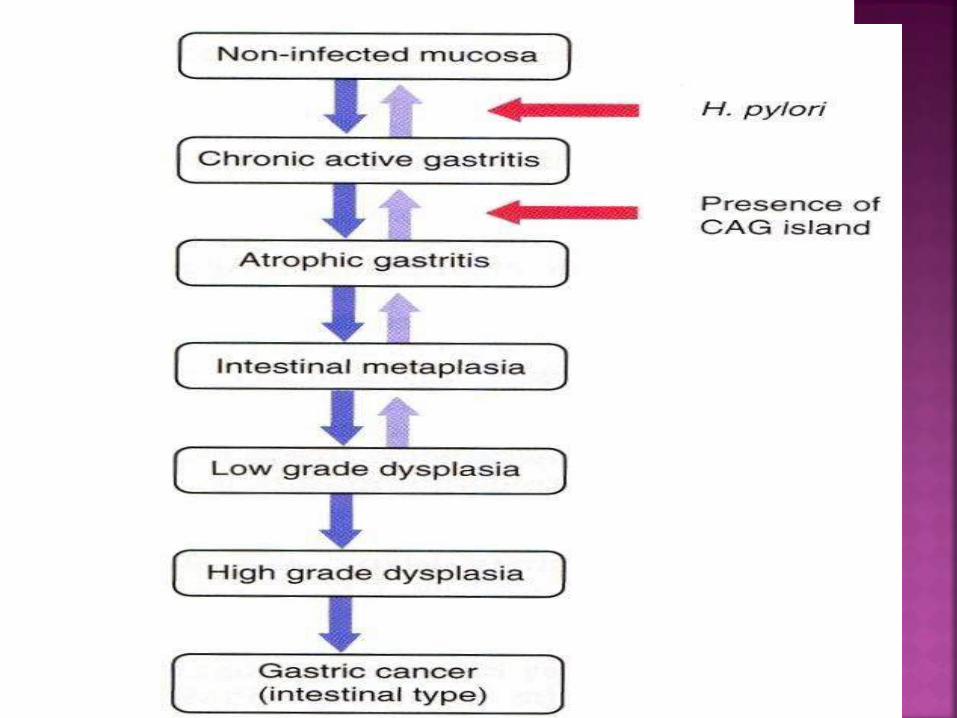
Chronic active gastritis
Precursor lesions of gastric adenocarcinoma
are atrophic gastritis , intestinal metaplasia,
and dysplasia.
CagA positive strains are associated with
reduced frequency of Barrett’s esophagus
and esophgeal adenocarcinoma.
WEAK ASSOCIATION BETTER LEVEL OF EVIDENCE
Raynaud’s
Phenomenon
Sclerodema
ITP
Acne rosacea
Migraines
Thyroiditis
GBS
CAD
ITP
IDA
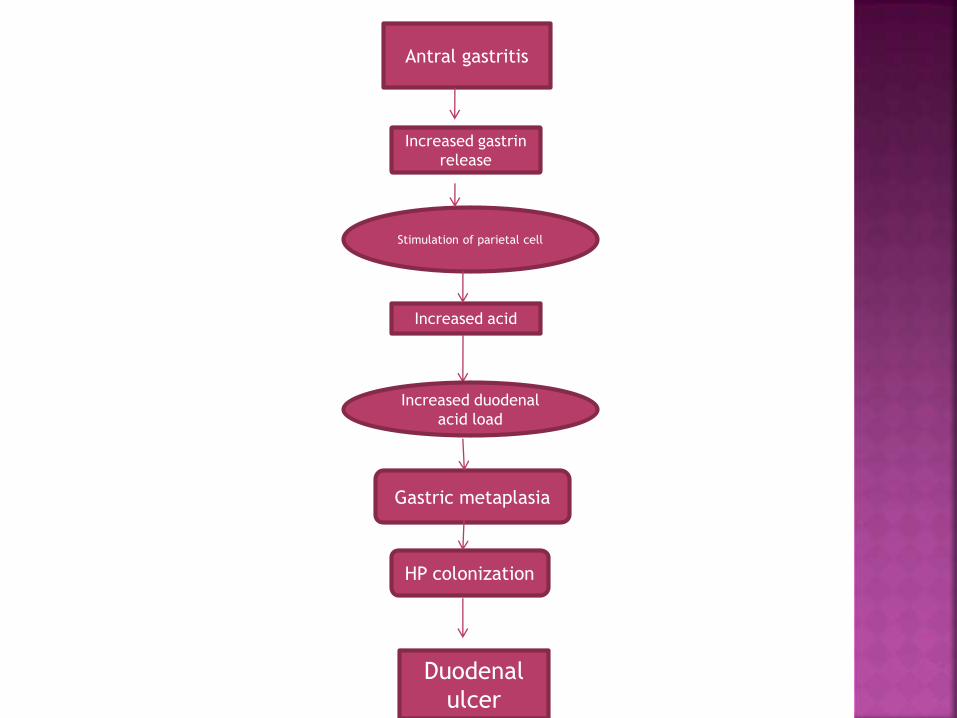
Antral gastritis
Increased gastrin
release
Stimulation of parietal cell
Increased acid
Increased duodenal
acid load
Gastric metaplasia
HP colonization
Duodenal
ulcer
Established• Active peptic ulcer disease (gastric or duodenal ulcer)
• Confirmed history of peptic ulcer disease (not previously treated for H. pylori)
• Gastric MALT lymphoma (low grade)
• After endoscopic resection of early gastric cancer
• Uninvestigated dyspepsia (depending upon H. Pylori prevalence)
Controversial• Nonulcer dyspepsia
• Gastroesophageal reflux disease
• Persons using nonsteroidal antiinflammatory drugs
• Unexplained iron deficiency anemia
• Populations at higher risk for gastric cancer
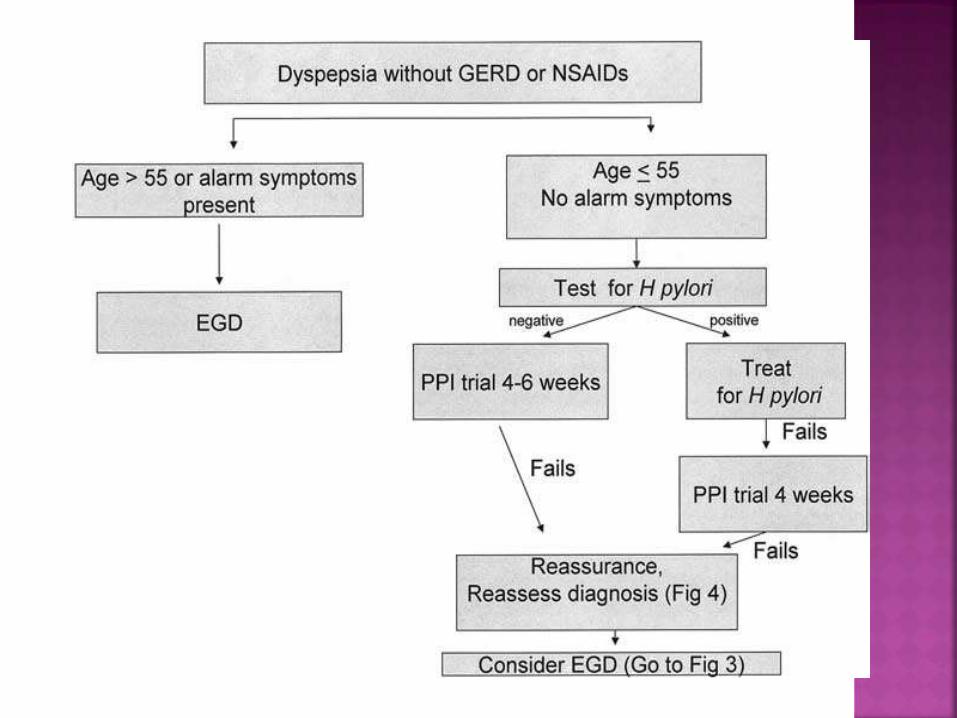
For patients with uninvestigated dyspepsia who are <55 yr and have no “alarm features”
ALARM FEATURES
Bleeding,
Anemia,
Early satiety,
Unexplained weight loss,
Progressive dysphagia,
Odynophagia,
Recurrent vomiting,
Family history of GI cancer,
Previous esophagogastric malignancy
Patients with
Peptic ulcer disease and
low grade MALT lymphoma;
Atrophic gastritis;
First degree relatives of patients with gastric
cancer;
Patients with unexplained IDA;
Patients with chronic ITP
For localized gastric MALT lymphoma, H.
pylori treatment achieves tumor regression
in 60–90% of patients
H. pylori eradication may offer a treatment
option not only for low grade MALToma but
also for early-stage H. pylori-positive gastric
DLBCL (MALT)
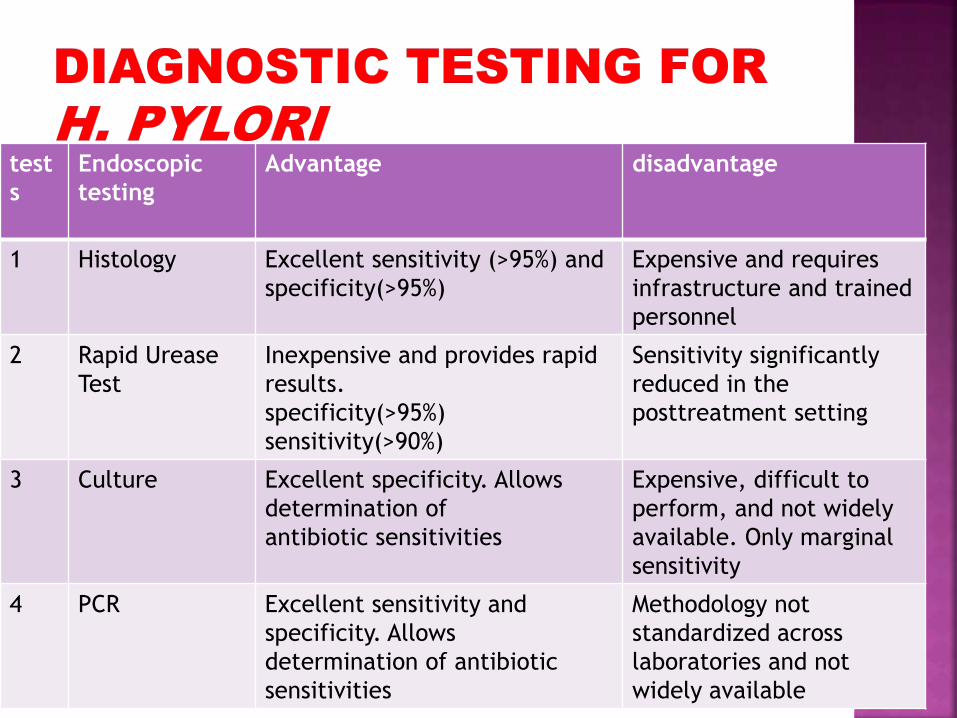
test
s
Endoscopic
testing
Advantage disadvantage
1 Histology Excellent sensitivity (>95%) and
specificity(>95%)
Expensive and requires
infrastructure and trained
personnel
2 Rapid Urease
Test
Inexpensive and provides rapid
results.
specificity(>95%)
sensitivity(>90%)
Sensitivity significantly
reduced in the
posttreatment setting
3 Culture Excellent specificity. Allows
determination of
antibiotic sensitivities
Expensive, difficult to
perform, and not widely
available. Only marginal
sensitivity
4 PCR Excellent sensitivity and
specificity. Allows
determination of antibiotic
sensitivities
Methodology not
standardized across
laboratories and not
widely available

To maximize the diagnostic yield of histology a
minimum of three biopsies be obtained.
One from the anglularis,
One from the greater curvature of the
corpus,
One from the greater curvature of the
antrum.
A recent study found that PCR was able to
detect H. pylori in approximately 20% of
gastric biopsies with chronic gastritis but no
identifiable organisms by histology
PCR also provides a means of identifying
mutations associated with antimicrobial
resistance
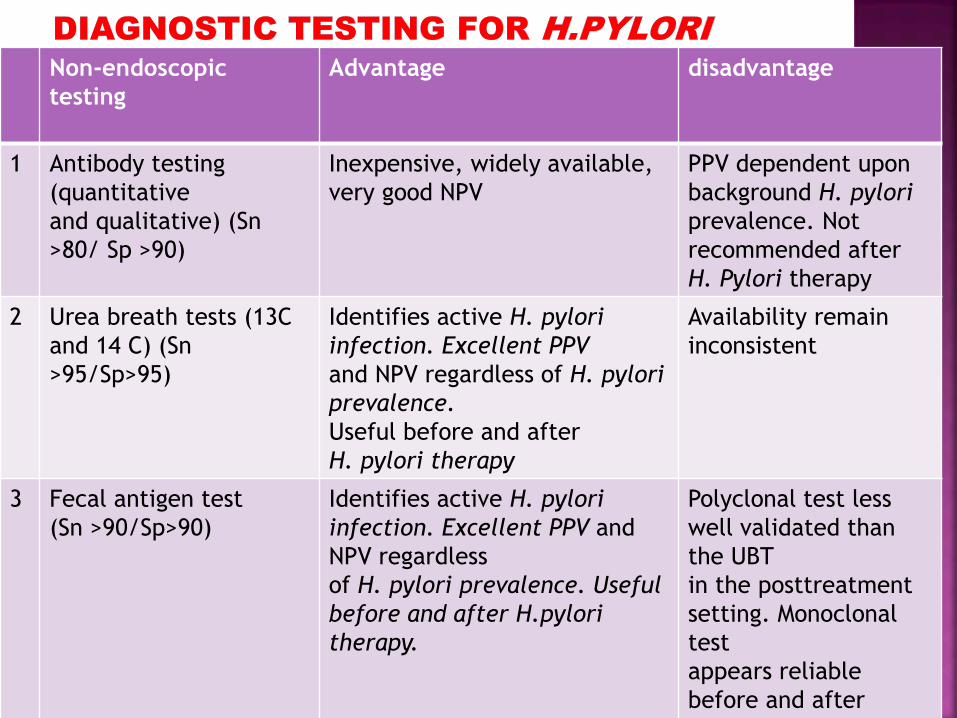
Non-endoscopic
testing
Advantage disadvantage
1 Antibody testing
(quantitative
and qualitative) (Sn
>80/ Sp >90)
Inexpensive, widely available,
very good NPV
PPV dependent upon
background H. pylori
prevalence. Not
recommended after
H. Pylori therapy
2 Urea breath tests (13C
and 14 C) (Sn
>95/Sp>95)
Identifies active H. pylori
infection. Excellent PPV
and NPV regardless of H. pylori
prevalence.
Useful before and after
H. pylori therapy
Availability remain
inconsistent
3 Fecal antigen test
(Sn >90/Sp>90)
Identifies active H. pylori
infection. Excellent PPV and
NPV regardless
of H. pylori prevalence. Useful
before and after H.pylori
therapy.
Polyclonal test less
well validated than
the UBT
in the posttreatment
setting. Monoclonal
test
appears reliable
before and after
antibiotic
The UBTs and fecal antigen tests provide reliable
means of identifying active H. pylori infection
before antibiotic therapy.
The UBT is the most reliable nonendoscopic test to
document eradication of H. pylori infection.
The monclonal fecal antigen test provides another
nonendoscopic means of establishing H. pylori cure
after antibiotic treatment.
Testing to prove H. pylori eradication: should
performed at least 4 wk after the completion of
antibiotic therapy.
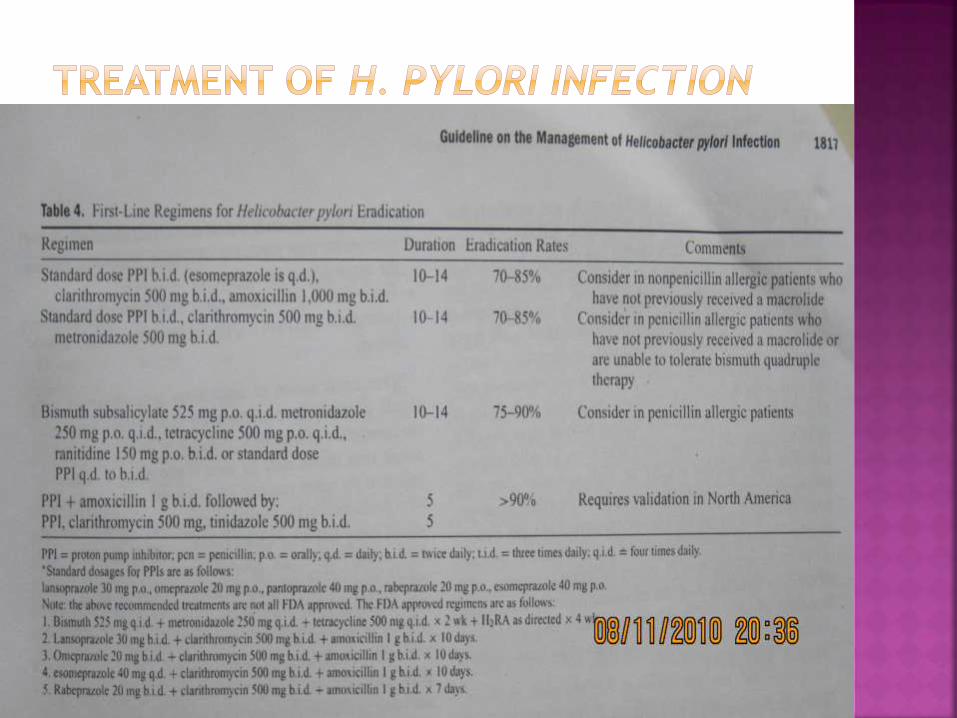
Any treatment regimen should achieve
eradication rate of >= 80%
Quadruple therapies are alternative first
choice treatment.
Bismuth based quadruple therapies remain
the second chice treatment, if not, a PPI,
amoxycillin or tetracycline and
metronidazole are recommended.
Initial treatment fails in up to 25% of
patients.
Reasons for that
• Antibiotic resistant organism,
• Poor compliance,
• Prior antibiotic use,
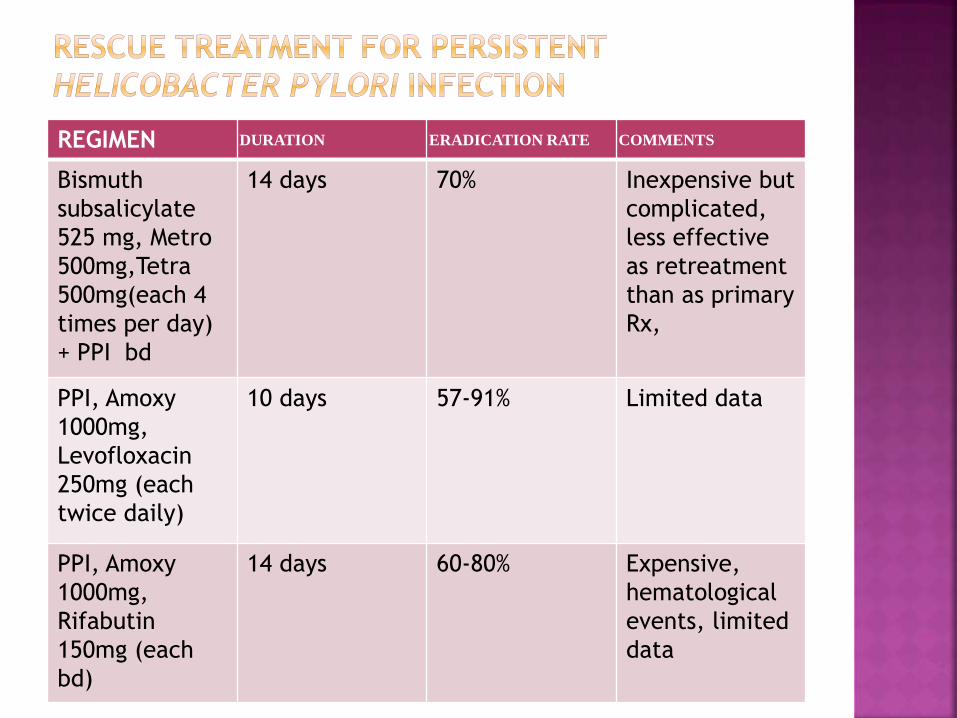
REGIMEN DURATION ERADICATION RATE COMMENTS
Bismuth
subsalicylate
525 mg, Metro
500mg,Tetra
500mg(each 4
times per day)
+ PPI bd
14 days 70% Inexpensive but
complicated,
less effective
as retreatment
than as primary
Rx,
PPI, Amoxy
1000mg,
Levofloxacin
250mg (each
twice daily)
10 days 57-91% Limited data
PPI, Amoxy
1000mg,
Rifabutin
150mg (each
bd)
14 days 60-80% Expensive,
hematological
events, limited
data
PPIs : headache and diarrhea, occurring in up to 10% of patients.
Macrolide (clarithromycin): GI upset, diarrhea, and altered taste.
Penicillin(amoxicillin): GI upset, headache & diarrhea.
Metronidazole: Dose related and include a metallic taste in the mouth, dyspepsia, and a disulfiram-like reaction with alcohol consumption.
Tetracycline: GI upset and photosensitivity. This antibiotic should not be used in children <8 yr of age.
Bismuth compounds: Darkening of the tongue and stool, nausea, and GI upset.
In United states
Metronidazole resistance: 40% strains
Clrithromycin strains: 11%
Teracyclin, Amoxycillin: <15%
INDIAN SCENARIO:
Due to antibiotic use or misuse widely
prevalent; high frequency of antibiotic
resistance.
several fixed-dose combinations of proton-pump
inhibitor with amoxicillin and tinidazole is the
most widely prescribed.
Fixed-dose combinations available: the dose of
amoxicillin is suboptimal, being 750 mg BID
rather than 1 g BID as recommended.
Form Packing/Price Photo PANTOCID-HP kit
1's (IRP: rupee 118) Related PANTOCID-HP
kit information Contents amoxycillin 750
mg, clarithromycin 600 mg, pantoprazole 40
mg CIMS Class Antacids, Antireflux Agents &
Antiulcerants Packing/Presentation
In multi-center study from India, 259 isolates
of H. pylori were tested for in vitro
susceptibility to antibiotics; of these,
77.9% -- metronidazole,
44.7% -- clarithromycin, and
32.8% -- amoxicillin.
In another study of 67 clinical isolates of H.
pylori from Kolkata,
85% -- metronidazole and
7.5% -- tetracycline,
but most were sensitive to clarithromycin,
furazolidone and amoxicillin.
Rates of recurrence of H. pylori infection
may be expected to be high in India.
H. pylori reinfection rates are very low in
Western populations,being less than 0.5 per
patient-year.
In one Indian study of 45 patients followed
up following eradication of H. pylori,
recurrence of infection was detected in only
one patient (2.4%) after one year.
The only other full publication on re-
infection in the Indian literature suggests
that recurrence of infection occurs in around
60% of patients.
REF: Nanivadekar SA, Sawant PD, Patel HD,
Shroff CP, Popat UR, Bhatt PP. Association or
peptic ulcer with Helicobacter pylori and the
recurrence rate. A three year follow up
study. J Assoc Physicians India 1990;38 (Suppl
1):703-6
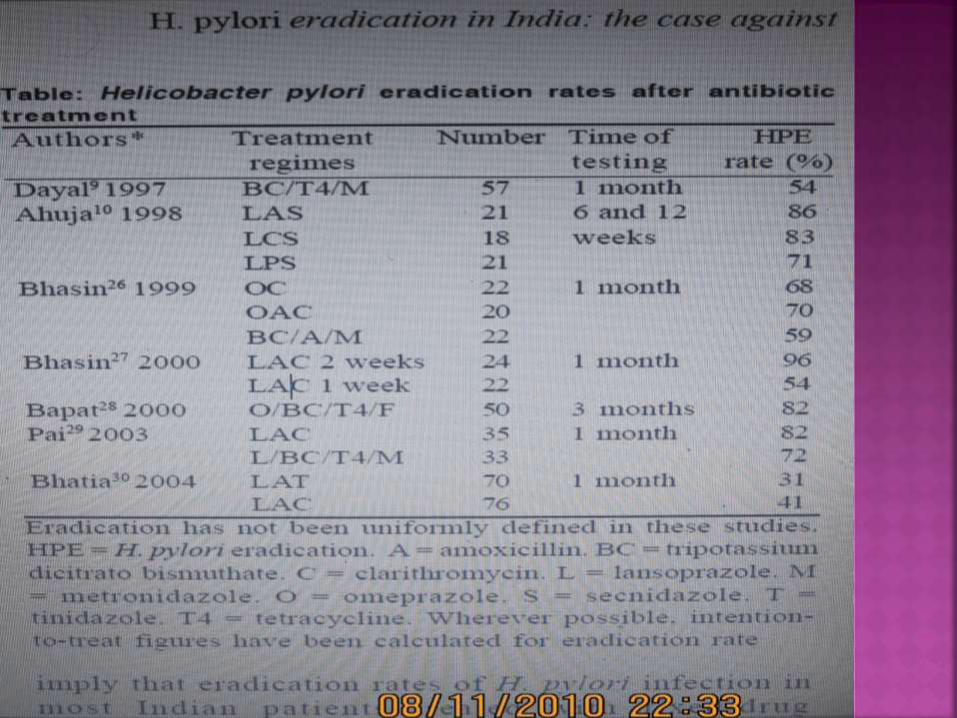
Studies from India suggest that between
75%-90% of DU in India heal with antibiotic
therapy aimed at H. pylori eradication.9,10
Ulcer relapse rates after antibiotic therapy
may be slightly higher in India than those
reported in the Western literature.
For instance, after an 11-month follow up, 5
of 31 (16%) patients who became H. pylori
negative had DU relapse compared to 8 of 12
patients (67%) who remained H. pylori
positive.9
Nanivadekar et al reported that among 66
cases with healed DU under follow up and
undergoing 152 endoscopic examinations,
ulcer relapse was seen in 6 of 61 (10%)
examinations without recurrence of H.
pylori infection and in 58 of 91 (63%)
examinations with recurrence of H. pylori
infection.11
Overall H. pylori resistance rate was
77.9% to metronidazole,
44.7% to clarithromycin and
32.8% to amoxycillin.
Multiple resistance was seen in 112/259
isolates (43.2%) and these were two/three
and four drug resistance pattern to
metronidazole, clarithromycin, amoxycillin
observed (13.2, 32 and 2.56%, respectively).
Metronidazole resistance was high in
Lucknow, Chennai and Hyderabad (68, 88.2
and 100%, respectively) and moderate in
Delhi (37.5%) and Chandigarh (38.2%).
Ciprofloxacin and tetracycline resistance was
the least, ranging from 1.0 to 4%.
The prevalence of resistance of H. pylori is
very high to metronidazole,
moderate to clarithromycin and amoxycillin and
low to ciprofloxacin and tetracycline.
The rate of resistance was higher in southern
India than in northern India.
Prevalence of the
CagA gene -- in 96% (90/94) of patients, and
VacA m2 -- 60% (56/94),
VacA m1 -- 32% (30/94).
A significant association between the cagA
and vacA m2 region (chi2 = 5.556; p < 0.01)
was found in ulcer patients.
The vacA m2 genotype showed a near-
significant value (chi2 = 3.943; p < 0.047) in
ulcer patients when compared with vacA m1.
These findings suggest that H. pylori strains
with the vacA m2 region were predominant
in South India, especially in and around
Chennai